POAC Paediatric Guideline Diarrhoea and
advertisement

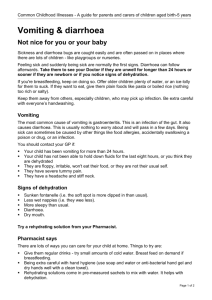
POAC Paediatric Guideline Diarrhoea and Vomiting caused by Gastroenteritis EXCLUDE • • • CAUTION Child presents with Diarrhoea and/or Vomiting age <2 months pre-existing conditions i.e. diabetes, inflammatory bowel disease, ileostomy/colostomy acute surgical pathology i.e. intussusception, obstructed inguinal/femoral hernia-(see note 1) No clinically detectable dehydration Appears well Alert and responsive Normal urine output Skin colour unchanged Warm extremities Eyes not sunken Moist mucous membranes Normal heart rate Normal breathing pattern Normal peripheral pulses Normal capillary refill time Normal skin turgor Assess severity of illness Clinical dehydration Altered behaviour (eg irritable, lethargic) Mildly decreased urine output Skin colour unchanged Warm extremities Sunken eyes Dry mucous membranes (except for ‘mouth breather') Mild tachycardia Mild tachypnoea Normal peripheral pulses Normal capillary refill time Reduced skin turgor Consider alternative diagnosis to gastroenteritis for: • Abdominal pain for >24hrs • Vomiting without diarrhoea • Bile stained vomit- means bowel obstruction until proven otherwise • Bloody diarrhoea • Signs of hypernatraemia (more lethargic than expected from level of dehydration) Clinical shock Appears to be unwell or deteriorating Decreased level of consciousness Decreased or absent urine output Pale or mottled skin Cold extremities No tears Tachycardia Tachypnoea Weak peripheral pulses Prolonged capillary refill time Initiate POAC Admit Standard Primary Care NOT ELIGIBLE FOR POAC FUNDING Discharge Home with advice sheet If high risk for deterioration consider review within 24 hours Parents/carers should seek medical review if : Measure baseline weight Rehydrate over 2-4 hours with Oral Rehydration Solution (ORS) ...(Note 2) • Consider Ondansetron ...(Note 3) Note: Vomiting is not a contraindication for ORS. If a child vomits wait 5-10 minutes and restart but more slowly • • Clinical review following ORS • • • child appears more drowsy than usual there is any blood in the diarrhoea or vomit that was not there previously parent/carer feels the child is less well than when they previously sought advise Policy date: February 2013 Review date: August 2013 Review daily for up to 48 hours Re weigh patient following rehydration period • If improving then discharge home with advice sheet and daily review • If worsening condition or not improving discuss with on call paediatrician • • To Hospital NOTE: If there are doubts regarding the child’s clinical state or social situation then discuss with Consultant Paediatrician DISCLAIMER: This management guideline has been prepared to provide general guidance with respect to a specific clinical condition. It should be used only as an aid for clinical decision making and in conjunction with other information available. The material has been assembled by a group of primary care practitioners and specialists in the field and adapted from the Starship Children’s Health Clinical Guideline. POAC Paediatric Guideline Diarrhoea and Vomiting caused by Gastroenteritis Aim: To enable the parent/carer to safely continue the patient care at home to reduce hospital referrals. Note 1 Not all vomiting is gastroenteritis. Bile stained vomiting means bowel obstruction until proven otherwise. Surgical conditions that may present with vomiting include pyloric stenosis (typical age about 6 weeks), intussusceptions (typical age about 6-10 months), appendicitis or intestinal malrotation. Non GI conditions that can potentially present with vomiting are: UTI, meningitis and pneumonia Note 2 Oral Rehydration Therapy (ORT) This is the treatment of choice for dehydration from gastroenteritis. It is safer and more effective than IV therapy for all degrees of dehydration except shock. Wherever possible continue breastfeeding or use expressed breast milk otherwise bubblegum Pedialyte is the ORS of choice. This takes advantage of glucose/sodium co-transport mechanisms in the small bowel. Assuming not note 1, consider stat Oradispersible Ondansetron in children >12 months. Single dose 2mg (1/2 tab) in children<15kg, 4mg single dose in children >15kg. Certain principles must be remembered: • ORT is intensive. It depends on a lot of input from the child’s caregiver • Fluid is given at a rate of 5ml per minute, by teaspoon or syringe. The small volumes decrease the risk of vomiting. The rate (1 teaspoon/minute) is easy to calculate and administer for a parent 25mls every 5 minutes can also be used. • This rate of replacement is already maximal, and is not supplemented for ongoing losses. If the child’s ongoing losses exceed an intake at this rate, the child will require nasogastric or IV fluids and should therefore be referred to hospital. • Hourly review is recommended • Vomiting is not a contra-indication. Most children with gastroenteritis, who vomit, will still absorb a significant percentage of any fluid given by mouth. Policy date: February 2013 Review date: August 2013 POAC Paediatric Guideline Diarrhoea and Vomiting caused by Gastroenteritis ON CALL PAEDIATRICIAN CONTACT NUMBERS Starship ....................................................................021 740 271 Kidz First (Middlemore) ............................................021 516 908 North Shore & Waitakere .........................................0800 244 533 POAC Funding Policy and Eligibility Criteria It is expected that the initial assessment and management of the child with Gastroenteritis is standard primary care and POAC is initiated when extended observation and treatment, (> 30 minutes) is required. Please note it is POAC policy that full clinical documentation is required and must demonstrate clinical eligibility (including initial assessment and observations undertaken throughout the episode of care). DISCLAIMER This management guideline has been prepared to provide general guidance with respect to a specific clinical condition. It should be used only as an aid for clinical decision making and in conjunction with other information available. This guideline has been developed by the POAC paediatric working group which includes the Clinical Directors from the 3 regional DHB’s: Dr Mike Shepherd (Starship), Dr Adrian Trenholme (Kidz First, CMDHB) and Dr Tim Jelleyman (WDHB) References: Starship Children’s Health Clinical Guideline: Dr Raewyn Gavin / Gastroenteritis Pathway Team 2006 Childhood Gastroenteritis Guideline, Waitako DHB 2004 NICE Clinical Guideline 84: Diarrhoea and vomiting in children Diarrhoea and vomiting caused by gastroenteritis: diagnosis, assessment and management in children younger than 5 years Policy date: February 2013 Review date: August 2013 POAC Paediatric Guideline Diarrhoea and Vomiting caused by Gastroenteritis PARENT ADVICE SHEET • • • • • • • • Gastroenteritis (“gastro”) is a bowel infection causing diarrhoea and sometimes vomiting Diarrhoea means runny, watery bowel motions (poo) The diarrhoea can last up to 10 days and your child may have tummy pain or fever Gastroenteritis is usually caused by a virus commonly called rotavirus It affects all age groups, but is more common, and can be worse in babies and young children The main concern is dehydration. Dehydration is the loss of fluid, due to vomiting and diarrhoea. Fluid replacement should be given in small amounts, frequently The younger the child, the easier it is for them to become dehydrated Signs of dehydration include fewer wet nappies, weight loss, more tired and sleepy than usual, sunken eyes, cold hands and feet and a dry mouth When to seek further help • Your child is unable to keep any fluids down or has a lot of diarrhoea (8-10 watery motions per day) • There is any blood in the diarrhoea or vomit, or severe stomach pains occur • Your child shows any signs of dehydration (as detailed in this sheet) • If your child is younger than 6 months, has other health problems and is not getting better or • If you are worried for any other reason See your family Doctor, local Accident and Medical Clinic or Childrens Emergency Department for urgent review Gastro spreads very easily to others. You can help to reduce the chance of this by: • Thorough hand washing- especially after using the toilet, changing nappies and before preparing food. Encourage children to wash and dry their hands after using the toilet • Thorough cleaning of toilet and bathroom areas • Dirty soiled clothing should be washed-in hot water preferably and separately from the rest of the family washing • Avoid sharing food and drinks • Keep your sick child away from friends and other children until vomiting and diarrhoea have stopped. This includes day care, Kohanga Reo and School until the diarrhoea has stopped MY INFORMATION GP Phone (call if any problems): ____________________________________________________________________________ POAC Case Reference Number: ______________________________________________________________________________ Appointments: ______________________________________________________________________________________________ Policy date: February 2013 Review date: August 2013