Imaging Features of Heterotopic Mesenteric Ossification: A Case
advertisement

中華放射醫誌 Chin J Radiol 2005; 30: 55-58
55
Imaging Features of Heterotopic Mesenteric
Ossification: A Case Report and Literature
Review
H UNG -W EN K AO C HANG -H SIEN L IOU * W EI -C HOU C HANG C HIH -Y UNG Y U C HENG -Y U C HEN
Department of Radiology, Tri-Service General Hospital, National Defense Medical Center
Heterotopic mesenteric ossification is extremely
rare. Here, we report a case of heterotopic mesenteric ossification in a 60-year-old man who underwent a Hartmann procedure with ileostomy for
treatment of diverticulitis spanning the descending
and sigmoid colon about 2 months ago. Imaging
studies of the abdomen, including roentgenography,
ultrasound, and computed tomography (CT)
revealed diffuse curvilinear high densities with
mature trabecular texture dispersing within the
mesentery. The patient underwent a laparotomy
with partial resection of the lesions. Heterotopic
mesenteric ossification was diagnosed by pathologic
examination. The characteristic imaging features of
this rare entity were discussed and literature was
reviewed.
Heterotopic mesenteric ossification is an
uncommon entity and frequently associated with complications such as bowel obstruction and even
intestinal perforation, posing critical clinical issues.
Only eleven cases, almost sustaining traumatic events
to the mesentery, have been reported in the English literature. Among these cases, the imaging feature of this
disorder was rarely documented. Herein we present
such a case of heterotopic mesenteric ossification and
describe the imaging findings on abdominal
roentgenography, ultrasound, and CT. The characteristic imaging features combined with typical clinical
history could make the correct pre-operative diagnosis
and therefore lead to appropriate patient care.
Key words: Mesentery, CT; Mesentery, disease;
Heterotopic ossification
A 60-year-old male was admitted to our hospital
for delayed ileo-anal anastomosis because he had
undergone a Hartmann procedure with a temporal
ileostomy for severe colonic diverticulitis two months
ago. During that operation, the segment of colonic
diverticulitis was successfully resected without other
abnormal findings.
After admission, the physical examination of the
abdomen revealed no tenderness or palpable mass. The
laboratory examination also appeared unremarkable.
Routine abdominal roentgenography revealed diffuse
amorphous opacifications with mature trabeculations
in the abdomen (Fig. 1). Ultrasound showed hyperechoic strands with strong acoustic shadows within the
mesentery (Fig. 2). Non-enhanced abdominal CT
demonstrated diffuse curvilinear high densities dispersing within the mesentery extending even to the
ileostomy stoma (Fig. 3). No evidence of ascites, intraabdominal neoplasm, or lymph node enlargement was
identified on the CT study.
The laparotomy for ileo-anal anastomosis was
performed but failed due to the presence of extensive
heterotopic bones in amorphous configuration within
Reprint requests to: Dr. Chang-Hsien Liou
Department of Radiology, Tri-Service General Hospital.
No. 325, Sec. 2, Cheng Kung Road, Taipei 114, Taiwan,
R.O.C.
CASE REPORT
56
Heterotopic mesenteric ossification
the mesentery (Fig. 4) of the distal jejunum and ileum.
The peritoneum and abdominal wall were not
involved. Only a small portion of the bone within the
mesentery can be resected during the operation.
Pathologic examination confirmed the presence of heterotopic bone formation within the mesentery.
Histopathology of these heterotopic bones showed
mature trabeculation without presence of bone marrow
or zonal phenomenon. Although the mesenteric ossification was not totally removed, the patient did not
experience significant symptoms of bowel obstruction
in the following year.
DISCUSSION
Heterotopic mesenteric ossification is a rare
disorder describing a metaplastic process that occurs
within the mesentery. The term “heterotopic ossification” refers to formation of bone outside the skeletal
system. Occurring in somatic soft tissues, myositis
ossificans is the most familiar form of heterotopic
ossification usually associated with blunt or tearing
trauma. Post-traumatic heterotopic ossification can be
found at any site. Hip is the most common site after
total hip arthroplasty, traumatic brain injury, or spinal
cord injury. As intraabdominal counterpart of myositis
ossificans, heterotopic mesenteric ossification usually
developed after abdominal operation. It may cause
intractable symptoms or functional limitations that
require surgical treatment. Frequent recurrence of the
ossification presents a therapeutic challenge [1].
To our knowledge, only eleven cases of heterotopic mesenteric ossification have been reported in the
English literature [1-5]. Most of the cases developed
small bowel obstruction by the ossifications after one
or more abdominal operations for nonneoplastic
disease [2]. Fortunately, our patient not yet experienced significant symptoms of bowel obstruction.
Among these cases, imaging feature of this disorder
was rarely documented. Hikim et al. described such a
case with trabecular-architecture radiodensities
evident on both roentgenography and CT study [5]. In
our case, similar curvilinear radiodensities with
mature trabecular texture within the mesentery were
also demonstrated on imaging studies.
The differential diagnoses of heterotopic mesenteric ossification include barium extravasation, dystrophic calcification, or osseous neoplasm. However,
the mature trabecular texture of the opacifications on
the abdominal roentgenography should help distinguishing heterotopic mesenteric ossification from
these mimicking diagnoses. Furthermore, whether
barium extravasation occurs could be certain with the
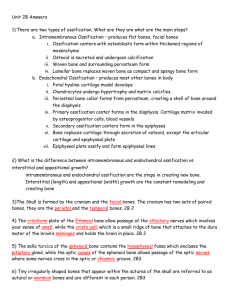
Figure 1. Abdominal roentgenography showed diffuse
amorphous opacifications with mature trabecular texture
(arrows) in the abdomen.
Figure 2. Ultrasound of the middle abdomen showed
hyperechoic strands (arrow) with strong acoustic shadow
indicating calcifications.
knowledge of clinical history. In our case, the fact that
barium contrast study was not performed before the
CT examination excluded the possibility of barium
extravasation.
In contrast to the location of mesentery, incision
scar is the more common site of heterotopic ossification that develops after abdominal surgery [6]. As a
form of myositis ossificans traumatica, heterotopic
Heterotopic mesenteric ossification
57
In summary, heterotopic mesenteric ossification
is a rare disorder, usually developing after abdominal
operation and causing complications such as bowel
obstruction and even intestinal perforation. The characteristic imaging features of heterotopic mesenteric
ossification should be kept in mind, which could lead
◆
to the correct pre-operative diagnosis.
REFERENCES
Figure 3. Non-enhanced abdominal CT at the level of
ileostomy stoma revealed diffuse curvilinear high
densities (arrows) dispersed within the mesentery
extending to the stoma.
Figure 4. A segment of resected bowel (arrowheads)
clearly demonstrated a heterotopic ossification (arrow)
within the mesentery.
ossification of abdominal surgical scars usually occurs
within longitudinal incisions and has distinct location
different from that of mesenteric ossification.
The pathogenesis of the heterotopic ossification
involves the local differentiation of multipotent mesenchymal cells [7]. The contributing factors may
include local trauma, inflammation, and venous stasis
[8, 9]. In addition, a local osteo-productive factor
named bone morphogenetic protein has been identified
contributing to heterotopic ossification [10, 11]. It
causes chemotaxis, proliferation of mesenchymal
cells, cartilage deposition and osteoblast-mediate
osteogenesis. Finally, normal lamellar bone developed
after remodeling.
1. Myers MA, Minton JP. Heterotopic ossification within
the small-bowel mesentery. Arch Surg 1989; 124: 982983
2. Wilson JD, Montague CJ, Salcuni P, Bordi C, Rosai J.
Heterotopic mesenteric ossification ('intraabdominal
myositis ossificans'): report of five cases. Am J Surg
Pathol 1999; 23: 1464-1470
3. Hansen O, Sim F, Marton PF, Gruner OP. Heterotopic
ossification of the intestinal mesentery. Report of a case
following intraabdominal surgery. Pathol Res Pract
1983; 176: 125-130
4. Yannopoulos K, Katz S, Flesher L, Geller A, Berroya R.
Mesenteritis ossificans. Am J Gastroenterol 1992; 87:
230-233
5. Hakim M, McCarthy EF. Heterotopic mesenteric ossification. AJR Am J Roentgenol 2001; 176: 260-261
6. Jacobs JE, Birnbaum BA, Siegelman ES. Heterotopic
ossification of midline abdominal incisions: CT and MR
imaging findings. AJR Am J Roentgenol 1996; 166:
579-584
7. Eidelman A, Waron M. Heterotopic ossification in
abdominal operation scars. Arch Surg 1973; 107: 87-88
8. Blane CE, Perkash I. True heterotopic bone in the paralyzed patient. Skeletal Radiol 1981; 7: 21-25
9. Stover SL, Hataway CJ, Zeiger HE. Heterotopic ossification in spinal cord-injured patients. Arch Phys Med
Rehabil 1975; 56: 199-204
10. Urist MR, Lietze A, Mizutani H, et al. A bovine low
molecular weight bone morphogenetic protein (BMP)
fraction. Clin Orthop 1982: 219-232
11. Kishimoto KN, Watanabe Y, Nakamura H, Kokubun S.
Ectopic bone formation by electroporatic transfer of
bone morphogenetic protein-4 gene. Bone 2002; 31:
340-347
58
Heterotopic mesenteric ossification
腸繫膜異位性骨化之影像表現:病例報告及文獻回顧
高鴻文 劉昌憲 張維洲 余之泳 陳震宇
國防醫學院 三軍總醫院 放射診斷部
腸繫膜異位性骨化十分罕見,我們報告一位 60 歲男性在 2 個月前因降結腸及乙狀結腸有憩
室炎,接受 Hartmann 手術治療。一系列的腹部影像檢查,包括 X 光素片、超音波、及電腦斷
層顯示出曲線狀高密度病灶合併成熟的骨樑結構散布於腸繫膜中。之後病人接受腹腔手術,病
理檢查確定診斷為腸繫膜異位性骨化。我們在文中討論這種罕見疾病的影像特徵並回顧文獻報
告。
關鍵詞:腸繫膜,電腦斷層攝影;腸繫膜,疾病;異位性骨化