CLINICAL GUIDELINE FOR INTRAVENOUS MORPHINE
ADMINISTRATION IN CLINICAL AREAS FOR ADULTS
1. Aim/Purpose of this Guideline
To provide guidance for the appropriate and safe administration of Intravenous (IV)
Morphine in clinical areas.
2. The Guidance
IV Morphine should be used for the initial control of acute severe pain only. It is
not recommended that IV Morphine is used for acute exacerbations of chronic
pain (British Pain Society 2010)
2.1. Ensure intravenous Morphine has been prescribed.
2.2. 10mg of Morphine should be made up to 10mls, with 0.9% sodium chloride, using
an aseptic non-touch technique. Label the syringe with contents immediately.
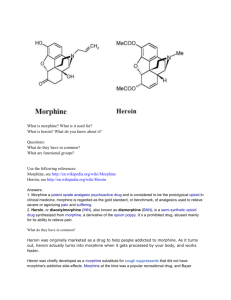
2.3. After this, follow the algorithm below to titrate intravenous analgesia, and monitor for
15 minutes after the last dose of Morphine.
The morphine should be given in 2mg boluses at 5-minute intervals until the maximum
prescribed dose has been achieved, or until the patient is comfortable. If the maximum
dose prescribed fails to establish good pain relief, contact admitting team.
No
Severe Pain
Equal to 3
Monitor for 15 mins
Yes
No
Sedation score less than/equal to 23.
Yes
No
Respirations greater than/equal to 84.
Yes
Administer IV morphine 2mg
5.
Reassess in 5 mins
Contact doctor if the respiratory rate
is less than 8 and /or sedation
score 3. Give oxygen 4 litres and
inform medical staff. Consider
giving naloxone. If respiratory rate
<5 and sedation score 3 give
naloxone (see below).
Draw up 400mcg (1ml) of naloxone and6.3mls of sodium chloride 0.9% and give in 1ml
increments. Naloxone should be given in7.increments of 100mcg every 5 minutes. This
should be given until respiratory rate >8 and
8. sedation score <2. Observe pain and sedation
scores closely. If not resolved after
9. 0.4mg, seek further medical advice.
Clinical Guideline for Intravenous Morphine Administration in Clinical Areas for Adults
Page 1 of 6
2.4. During injection observe the surrounding area for extravasation or local sensitivity
reactions. Mild reactions can occur after administration of IV Morphine. Significant redness
or swelling should be reviewed by a doctor.
2.5. Monitor the patient’s conscious level, blood pressure, pulse, respiratory rate and
oxygen saturation every 5 minutes AND for 20 minutes after the last dose of morphine has
been injected.
2.6. For safety, it is not recommended that patients leave the ward for 1 hour after
receiving IV Morphine.
NB. Patients with cancer may already be on large doses of opioids. Please contact
Palliative Care, Oncology or Pain Team for advice, as the intravenous doses may be
larger.
3. Monitoring compliance and effectiveness
Element to be
monitored
Adherence to guideline for IV morphine administration in clinical
areas.
Dr Nicholas Marshall, Consultant Anaesthetist, Acute Pain Lead.
Lead
Datix reports will be investigated.
Tool
Audits will be completed 4 yearly.
Frequency
The audit results will be reported to the Acute Pain Lead
Reporting
Consultant and the Pain Service Governance Lead Consultant.
arrangements
Documented recommendations made, acted on and amended
Acting on
within a specified time frame by Acute Pain Team and Dr.
recommendations
Nicholas Marshall.
and Lead(s)
Required changes to practice will be identified and actioned within
Change in
1 month depending on changes required. A lead member of the
practice and
team will be identified to take each change forward where
lessons to be
appropriate. Lessons will be shared with all relevant stakeholders.
shared
4. Equality and Diversity
4.1 This document complies with the Royal Cornwall Hospitals NHS Trust service
Equality and Diversity statement which can be found in the ‘Equality, Diversity
and Human Rights policy’ or the Equality and Diversity website.
4.2 Equality Impact Assessment
The Initial Equality Impact Assessment Screening Form is at Appendix 2.
Clinical Guideline for Intravenous Morphine Administration in Clinical Areas for Adults
Page 2 of 6
Appendix 1. Governance Information
Document Title
Clinical Guideline for Intravenous Morphine
Administration in Clinical Areas.
Date Issued/Approved:
13th October 2015
Date Valid From:
13th October 2015
Date Valid To:
13th October 2018
Theatres and Anaesthetic Directorate,
Pain Services
Cheryl Jewell, Pain Specialist Nurse.
Directorate / Department responsible
(author/owner):
Contact details:
01872 252095
Brief summary of contents
Guidelines for nursing staff administering
Intravenous Morphine in Clinical Areas.
Morphine
IV morphine
Intravenous Morphine
RCHT
PCH
Suggested Keywords:
Target Audience
Executive Director responsible for
Policy:
Date revised:
This document replaces (exact title of
previous version):
CFT
KCCG
Executive Medical Director, Dr Rob Parry
01 / 05 / 2015
Nursing Guidelines for Intravenous
Morphine Administration in Clinical Areas.
Pain Services, RCHT
Governance, RCHT
Approval route (names of
committees)/consultation:
Divisional Manager confirming
approval processes
Name and Post Title of additional
signatories
Signature of Executive Director giving
approval
Publication Location (refer to Policy
on Policies – Approvals and
Ratification):
Mr Duncan Bliss
Dr Keith Mitchell (Pain Governance Lead)
{Original Copy Signed}
Internet & Intranet
Intranet Only
Document Library Folder/Sub Folder
Document library and Pain sub folder
Links to key external standards
None
Related Documents:
Training Need Identified?
British Pain Society (2010) Opioids for
persistent pain: Good practice. Available
from URL:
https://www.britishpainsociety.org/static/u
ploads/resources/files/book_opioid_main.
pdf
Yes. Registered Nurse competent in
administering intravenous medication.
Clinical Guideline for Intravenous Morphine Administration in Clinical Areas for Adults
Page 3 of 6
Version Control Table
Date
1 Jul 15
Versio
n No
Summary of Changes
Changes Made by
(Name and Job Title)
V4.0
Changed onto new Trust template
British Pain Society guidance regarding IV
Morphine and chronic pain.
Recommendations not to leave the ward for 1
hour following administration of IV Morphine.
Change of policy name to identify appropriate
patient demographic.
Cheryl Jewell
Pain Specialist Nurse
All or part of this document can be released under the Freedom of Information
Act 2000
This document is to be retained for 10 years from the date of expiry.
This document is only valid on the day of printing
Controlled Document
This document has been created following the Royal Cornwall Hospitals NHS Trust
Policy on Document Production. It should not be altered in any way without the
express permission of the author or their Line Manager.
Clinical Guideline for Intravenous Morphine Administration in Clinical Areas for Adults
Page 4 of 6
Appendix 2. Initial Equality Impact Assessment Form
Name of Name of the strategy / policy /proposal / service function to be assessed (hereafter
referred to as policy) (Provide brief description): Clinical guideline for Intravenous Morphine
Administration in Clinical Areas.
Directorate and service area:
Is this a new or existing Policy?
Anaesthetics/Pain
Existing
Name of individual completing
Telephone:
assessment: Cheryl Jewell
(01872) 252095
1. Policy Aim*
Aimed at nursing and medical staff.
Who is the strategy /
policy / proposal /
service function
aimed at?
2. Policy Objectives*
To maintain safe standards for the delivery of IV morphine as a
pain control.
3. Policy – intended
Outcomes*
4. *How will you
measure the
outcome?
5. Who is intended to
benefit from the
policy?
6a) Is consultation
required with the
workforce, equality
groups, local interest
groups etc. around
this policy?
Patients requiring IV Morphine are cared for safely and
effectively. Side effects and complications identified promptly
and dealt with safely. Requirement for additional training
identified.
Regular audit.
Monitoring of DATIX reports.
Patient satisfaction regarding pain control.
Patients, medical, nursing and allied health care professional
team.
No
b) If yes, have these
*groups been
consulted?
C). Please list any
groups who have
been consulted about
this procedure.
7. The Impact
Please complete the following table.
Are there concerns that the policy could have differential impact on:
Equality Strands:
Age
Sex (male, female, trans-
Yes
No
x
Rationale for Assessment / Existing Evidence
x
gender / gender
reassignment)
Clinical Guideline for Intravenous Morphine Administration in Clinical Areas for Adults
Page 5 of 6
Race / Ethnic
communities /groups
x
Disability -
x
learning
disability, physical
disability, sensory
impairment and
mental health
problems
Religion /
other beliefs
x
Marriage and civil
partnership
x
Pregnancy and maternity
x
Sexual Orientation,
x
Bisexual, Gay, heterosexual,
Lesbian
You will need to continue to a full Equality Impact Assessment if the following have been
highlighted:
You have ticked “Yes” in any column above and
No consultation or evidence of there being consultation- this excludes any policies
which have been identified as not requiring consultation. or
Major service redesign or development
No
8. Please indicate if a full equality analysis is recommended.
9. If you are not recommending a Full Impact assessment please explain why.
Signature of policy developer / lead manager / director
Names and signatures of
members carrying out the
Screening Assessment
Date of completion and submission
1.
2.
Keep one copy and send a copy to the Human Rights, Equality and Inclusion Lead,
c/o Royal Cornwall Hospitals NHS Trust, Human Resources Department, Knowledge Spa,
Truro, Cornwall, TR1 3HD
A summary of the results will be published on the Trust’s web site.
Signed _______________
Date ________________
Clinical Guideline for Intravenous Morphine Administration in Clinical Areas for Adults
Page 6 of 6
 0
0