as a PDF
advertisement

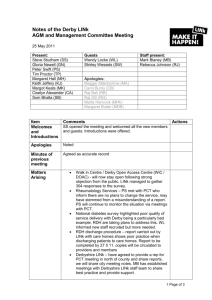
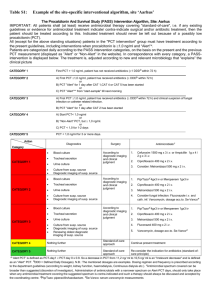
Clinical Chemistry 46:10 1583–1587 (2000) Evidence-based Laboratory Medicine and Test Utilization Serum Procalcitonin Concentrations in Term Delivering Mothers and Their Healthy Offspring: A Longitudinal Study Marcello Assumma,1 Fabrizio Signore,2 Lucia Pacifico,3,5 Naila Rossi,1 John F. Osborn,4 and Claudio Chiesa3,5* Background: The reported sensitivities and specificities of procalcitonin (PCT) concentrations for the diagnosis of neonatal infection vary widely. A postnatal increase of PCT has been observed in healthy term newborns with a peak at ⬇24 h of age, and many questions remain regarding maternal and perinatal factors that may influence the normal PCT kinetics during the immediate postnatal period. Methods: We prospectively investigated the association between the serum PCT values obtained from 121 mothers at delivery and serum PCT in their healthy, term offspring at birth as well as at 24 and 48 h of age. We also analyzed whether obstetric and perinatal factors would alter maternal and neonatal PCT response. Results: PCT concentrations in the babies at birth were significantly higher than in the mothers (P <0.0001), with even larger differences at 24 and 48 h of age. None of the variables identified from maternal and perinatal histories had a significant effect on maternal PCT response. In the healthy neonate, the variables that significantly affected the concentration of PCT at birth were the mothers’ PCT (P <0.01), maternal group B streptococcus colonization (P <0.05), and rupture of membranes >18 h (P <0.01). The coefficient of linear correlation between the mother’s PCT concentration and that of the baby at birth was 0.32 (P <0.01). The only variable that significantly altered the PCT concentration at both 24 (P <0.01) and 48 (P <0.01) h of age was rupture of Divisions of 1 Neonatology and 2 Obstetrics, S. Camillo Hospital, 00152 Rome, Italy. Institutes of 3 Pediatrics and 4 Hygiene, “La Sapienza” University of Rome, 00161 Rome, Italy. 5 Institute of Experimental Medicine, National Research Council, 00161 Rome, Italy. * Address correspondence to this author at: Institute of Pediatrics, La Sapienza University of Rome, Viale R. Elena, 324 00161 Rome, Italy. Fax 39-06-49-218-480; e-mail Claudio.Chiesa@Uniroma1.it. Received May 12, 2000; accepted July 31, 2000. membranes >18 h. Nonetheless, the PCT response observed during the 48-h period after birth among healthy babies born to mothers with risk factors for infection was well below that reported previously among agematched neonates with sepsis. Conclusions: The postnatal increase of PCT observed in the healthy neonate with peak values at 24 h of age most likely represents endogenous synthesis. In estimating the sensitivities and specificities of PCT for diagnosis of sepsis throughout the initial 48 h of life, it is important to consider the normal PCT kinetics and the pattern(s) of PCT response in the healthy neonate. © 2000 American Association for Clinical Chemistry High serum concentrations of procalcitonin (PCT),6 the prohormone of calcitonin, have been reported in adults and children with invasive bacterial or fungal infections (1– 6 ). Although it has been suggested that PCT may be a useful marker of septicemia in newborns, the estimates of sensitivity and specificity for the diagnosis of neonatal infection vary widely, especially during the 48-h period after birth (7–14 ) when the majority of diagnostic problems are encountered. In a previous cross-sectional study (9 ), we showed that in the healthy neonates circulating concentrations of PCT increase gradually from birth to reach peak values at about 24 h of age and then decrease gradually by 48 h of life, primarily reflecting a physiologic postnatal surge of PCT. However, many questions remain unanswered about maternal and perinatal factors that may influence the normal PCT kinetics during the immediate postnatal period. Given the low molecular mass (⬇12 kDa) of PCT (15 ), it is not surprising that transplacental passage has been suggested as a possible source of 6 Nonstandard abbreviations: PCT, procalcitonin; GBS, group B streptococcus; CI, confidence interval; TNF-␣, tumor necrosis factor-␣; and IL-6, interleukin-6. 1583 1584 Assumma et al.: Procalcitonin in Mother-Newborn Pairs the postnatal increase of PCT (16 ), although we are not aware of any study dealing specifically with this issue. The main objective of the present study was to investigate the association, if any, between serum PCT concentrations in mothers at delivery and serum PCT in their healthy babies at birth as well as at 24 and 48 h of age. The three fixed neonatal ages 0, 24, and 48 h could provide this information given that the half-life of PCT is 22–29 h (17 ). Also, we investigated whether maternal and perinatal factors could confound these associations. Materials and Methods patients This study was performed at the Obstetric Unit and the well-baby nursery of the Saint Camillo Hospital, Rome. As part of an ongoing prospective investigation of serum PCT values in complicated and uncomplicated pregnancies, mothers were eligible for enrollment if: (a) they agreed to participate in the study and signed consent forms approved by the Institutional Review Board of the Saint Camillo Hospital; and (b) they delivered singleton term newborns with normal birth weights (ⱖ2500 g) and with normal results on physical examination at birth implying, therefore, no need of empiric management. The mother-infant pair was included in the present study if all the following criteria were met: (a) a blood sample was collected at the time of delivery from the mother; (b) a blood sample was obtained at birth, at 24 h, and at 48 h after birth from each infant; and (c) the neonate had a continuous, uncomplicated hospital stay until discharge on day 3 after vaginal or day 4 after cesarean delivery and also normal assessments at the 2- and 4-week follow-up visits. We excluded parturients with: (a) multiple preexistent or pregnancy-related noninfectious complications; or (b) clinically evident intraamniotic infection [defined as intrapartum fever (ⱖ38 °C) accompanied by at least two of the following: tachycardia (maternal, ⱖ100 beats/min; fetal, ⱖ160 beats/min), uterine tenderness, purulent amniotic fluid, or increased peripheral white blood cell count (⬎15 000/mm3)]. All antepartum and intrapartum data were collected prospectively and included maternal age, pre-existent or pregnancy-related diseases, mode of delivery, use of anesthesia, duration of active labor (18 ), interval between rupture of membranes and delivery, maternal group B streptococcus (GBS) colonization, intrapartum antimicrobial administration, and abnormalities in intrapartum fetal heart monitoring. The institutional policy was to give term women with rupture of membranes ⱖ18 h intrapartum penicillin or broad-spectrum antibiotics, if results of GBS cultures were not known at the time of labor (19 ). Late prenatal cultures (35–37 weeks) including vaginal specimens for GBS culture (20 ) were considered a part of good antenatal care. For those with poor or no antenatal care, intrapartum vaginal specimens were obtained for culture. For term women with rupture of membranes ⬍18 h, the institutional policy was to treat those patients with late prenatal cultures positive for GBS. Neonatal data collected included gestational age, birth weight, gender, and Apgar scores at 1 and 5 min. pct determination Blood for PCT determination was centrifuged within 30 min of collection, and the serum was stored at ⫺70 °C until analysis. PCT was first determined by the LUMItest威 PCT method (BRAHMS Diagnostica) as described in detail elsewhere (9 ). According to the manufacturer, this immunoluminometric assay has a detection limit of 0.1 g/L. Interassay and intraassay variations at both low and high concentrations were ⬍8% and 7%, respectively. Samples with PCT concentrations below the detection limit of the LUMItest PCT assay were subsequently tested with the LUMItest ProCa-S assay (BRAHMS Diagnostica), which has been developed in a prototype format only. This immunoluminometric test is more sensitive (limit of detection, 0.005 g/L) than the LUMItest PCT assay. Duplicate determinations of PCT were performed for each serum sample, without knowledge of the maternal and neonatal clinical characteristics. statistical analysis The PCT values (Fig. 1) were distributed with a long tail to the right (positive skew), but the logarithms of the values of PCT were approximately normally distributed. Fig. 1. Distribution of crude PCT values among 121 delivering mothers and their healthy offspring at the three neonatal ages 0, 24, and 48 h. Œ, 10 subjects; F, 1 subject. 1585 Clinical Chemistry 46, No. 10, 2000 Thus, the data were analyzed after a logarithmic transformation, and the results were expressed as geometric means with 95% confidence intervals (CIs). The geometric mean concentration of PCT in the mothers was compared with that of the babies at birth and at 24 and 48 h of age by applying a matched-pairs t-test to the logarithms of the PCT values, from which the mean percentage difference and its CI can be derived. The nonparametric Wilcoxon test was also applied to confirm the result of the t-test. The association between the serum PCT values obtained from mothers and serum PCT in their healthy offspring at birth and at ages 24 and 48 h were investigated by multiple regression of the log PCT of the baby on the log PCT of the mother, whereas dummy variables were used to take account of the possible confounding effects of: gestational diabetes, pregnancy-induced hypertension, intrapartum fetal distress, maternal GBS colonization, type of delivery (spontaneous vaginal, elective cesarean section, emergency cesarean section, and induced delivery), duration of active labor, interval (h) between rupture of the membranes and delivery, intrapartum antimicrobial administration, and use of epidural or general anesthesia. All statistical tests were considered significant if P ⬍0.05. Results One hundred fifty-two neonates born on 42 randomly selected study days were enrolled at birth. Thirty-one neonates were subsequently excluded from the study because: 6 infants were transferred to the intermediate nursery 12–18 h after birth, in 20 infants the PCT measurements were not made according to the protocol design, and 5 infants were inadequately followed-up after discharge from hospital. Thus, data from a total of 121 mother-newborn pairs were available for analysis. The characteristics of mothers and their healthy infants are summarized in Table 1. Table 2 shows the geometric mean PCT concentration in delivering mothers and in their healthy newborns at each postnatal age. PCT concentrations in the babies at birth were significantly higher than in the mothers (P ⬍0.0001 by t-test; P ⬍0.0001 by Wilcoxon test), with even larger differences at 24 and 48 h of life. At 24 and 48 h after birth, the geometric mean concentration of PCT in the babies was 220 and 76 times higher than the concentration observed in the delivering mothers, respectively (Table 2). By multiple regression analysis, none of the variables identified from maternal and perinatal history had a significant effect on PCT response in parturient mothers. Multiple regression analysis of PCT values observed in the babies at delivery on the mother’s PCT and the confounders identified from antepartum and intrapartum data (see Statistical Analysis) revealed that the variables that significantly affected PCT concentrations in the babies at birth were the PCT concentrations in the delivering mothers, maternal GBS colonization, and rupture of membranes for 18 h or longer. The crude product–moment Table 1. Maternal and neonatal characteristics. Maternal Mean age, years Complications during pregnancy Gestational diabetes Pregnancy-induced hypertension Mode of delivery Spontaneous vaginal Induced vaginal Emergency cesarean section Elective cesarean section Use of epidural anesthesia Use of general anesthesia Mean length of active labor, h Mean time of ruptured membranes, h Ruptured membranes ⱖ18 ha GBS colonizationa (35–37 weeks of gestation) Intrapartum antibimicrobial administration Infant Mean birth weight, g Mean gestational age, weeks Male gender Apgar scores ⱕ7 at 1 min ⱕ8 at 5 min a 31.0 (SD, 4.6) 5 (4.1%) 9 (7.4%) 54 (44.6%) 24 (19.8%) 12 (9.9%) 31 (25.6%) 23 (19.0%) 20 (16.5%) 2.9 (SD, 2.6) 4.9 (SD, 11.2) 13 (10.7%) 11 (9.0%) 24 (19.8%) 3230 (SD, 396) 39.2 (SD, 1.2) 65 (53.7%) 0 0 Occurring as an isolated event. coefficient of linear correlation, r, between the mother’s PCT values and those of the baby at birth was 0.32 (P ⬍0.01), and the Spearman rank correlation was 0.38. The baby’s PCT concentration at birth was increased by a factor of 1.45 (95% CI, 1.05–1.99; P ⬍0.05) if the mother had GBS colonization and 1.50 (95% CI, 1.12–2.0; P ⬍0.01) if the time from rupture of the membranes was ⱖ18 h. In contrast, the multiple regression showed that the mothers’ PCT had no significant association with the baby’s concentration at both 24 (r ⫽ 0.021; P ⫽ 0.41) and 48 (r ⫽ 0.025; P ⫽ 0.40) h of age. Likewise, the rank correlation coefficients were 0.023 and 0.004, respectively. Indeed, at both postnatal hours 24 and 48, the only variable found to be associated with the babies’ values of PCT was the time since rupture of the membranes. If this time was ⱖ18 h, the concentration of PCT was increased by a factor of 2.84 Table 2. Geometric mean PCT values in 121 delivering mothers and their healthy newborns at ages 0, 24, and 48 h of life and the ratios of the geometric means of the newborns to that of the mothers. PCT (g/L) Geometric mean (95% CI) Mothers Newborns At birth At 24 h At 48 h Ratio newborn/mother (95% CI) 0.010 (0.009–0.013) 0.094 (0.084–0.10) 2.47 (1.97–3.09) 0.83 (0.67–1.02) 8.5 (7.1–10.2) 220 (163–297) 76 (57–102) 1586 Assumma et al.: Procalcitonin in Mother-Newborn Pairs (95% CI, 1.50 –5.48; P ⬍0.01) at 24 h of life and by 2.47 (95% CI, 1.29 – 4.73; P ⬍0.01) at 48 h. In fact, for babies born to mothers with rupture of the membranes ⱖ18 h, the geometric mean PCT values were 5.96 g/L (95% CI, 2.50 –14.18) at 24 h of age and 1.82 g/L (95% CI, 0.73– 4.53) at 48 h. In contrast, if the time since rupture of the membranes was ⬍18 h, the geometric mean values of PCT were 2.16 g/L (95% CI, 1.74 –2.69) at 24 h of age and 0.74 g/L (95% CI, 0.61– 0.92) at 48 h. Discussion In the early neonatal period, especially in the first 2 days after birth, various kinds of laboratory values may change considerably, and their mean “normal” values differ from those measured in later periods. Variable intervals that change rapidly have been, for example, observed for bilirubin, aspartate aminotransferase, oxygen tension, hemoglobin, and neutrophilic cells as well as for hormones and cytokines (21, 22 ). Some of the differences are attributable to direct stress on the baby during the perinatal period or to maladaption to the extrauterine environment, causing the activation or suppression of certain substances. Creatine kinase and thyroid-stimulating hormone are in this category. Other changes are attributable to influx from the placenta. For example, immunoglobulin G that crosses the placenta raises the concentrations in the infants toward the concentrations in the mother. The modest positive association between PCT values in paired maternal and cord sera found in our study suggests that PCT may cross the placental barrier, but the findings of higher PCT concentrations in cord sera compared with maternal samples, with even larger differences at 24 and 48 h of age, cannot be explained on the basis of maternal transfer alone. Therefore, the postnatal surge of PCT most likely represents endogenous synthesis. Most previous studies did not assess the postnatal course of PCT (7, 8, 10 –14 ) in the healthy term baby, neither did they provide information as to whether maternal and perinatal factors may affect the interpretation of what constitutes the abnormal (and as importantly the normal) postnatal PCT value. Consequently, the reported “normal” ranges have been relatively broad and have made uncertain the use of PCT as a discriminatory tool for differentiating infected from uninfected neonates during the immediate postnatal period. The present study, which is the first to analyze the PCT response of a cohort of healthy, full-term neonates born under different clinical scenarios, shows that pathologic prenatal noninfectious conditions, such as gestational diabetes or pregnancyinduced hypertension, do not affect the babies’ PCT concentration during the 48-h period after birth. Additionally, perinatal stress, surgical trauma, and anesthesia did not significantly alter PCT response in such neonatal population. However, the novel finding observed in the current investigation is that neonates born to intrapartumtreated mothers with isolated risk factors for infection, although totally asymptomatic, had significantly in- creased PCT concentrations when compared with those who were born to mothers who were either risk factor negative or who had only noninfectious clinical conditions. The exact site of PCT release during sepsis is unclear. Recently, Brunkhorst et al. (23 ) mentioned that one possible site of PCT production during inflammation is peripheral blood mononuclear cells, whereas Nijsten et al. (24 ) suggested that the liver is a major source of PCT production. There are few data to support either possibility. Likewise, the mechanism of PCT release remains uncertain. Dandona et al. (25 ) first showed that when endotoxin was administered to apparently healthy human volunteers, the expected release of tumor necrosis factor (TNF)-␣ and interleukin (IL)-6 was followed by an increase and prolonged peak of concentrations of circulating PCT. A tenable interpretation was that endotoxin might release PCT directly, without cytokine mediation. More recently however, Nijsten et al. (24 ) showed that, directly or indirectly, IL-6 and TNF-␣ release PCT. Whatever the site(s) and mechanism(s) of PCT release, the amount of PCT produced and the degree of increase in serum concentrations have been correlated with the extent of the inflammatory reaction to infection (1, 26 ). Al-Nawas et al. (2 ) reported higher PCT concentrations in adult patients with clinically documented infection than in those merely fulfilling the criteria of systemic inflammatory response syndrome. Similar observations have been reported recently by Martin-Denavit et al. (27 ) in neonates with unspecified gestational age. These authors showed that, among neonates born to intrapartumtreated mothers who presented a risk factor for infection (including premature rupture of membranes or maternal GBS colonization), mean PCT values at both 24 and 72 h of life were much higher in those with clinical signs of infection than in the ones without. In the current study, the magnitude of PCT response observed during the first 48 h of life among healthy term babies born to mothers with either rupture of membranes ⱖ18 h or GBS colonization remained modest, being well below the concentrations reached in symptomatic neonates with early-onset (i.e., within the first 48 h of life) infection (9 ). Nonetheless, it would be reasonable to postulate that the increased PCT concentrations in such neonates specifically represent a host inflammatory response to the infectious stimuli, and their presence may then remain a potential marker of infection. We cannot rule out subclinical infection in some of these infants born to intrapartum-treated mothers; however, none of them became symptomatic or received antibiotic treatment. Serum PCT values obtained in this longitudinal study from healthy neonates born to mothers without infectious risk factors are comparable with those reported in a previous cross-sectional study of the whole population of healthy neonates born after uncomplicated pregnancy and labor (9 ). The pattern(s) of PCT response and temporal course of the increase in PCT concentrations in the healthy neonate should be taken into account to Clinical Chemistry 46, No. 10, 2000 optimize the use of PCT in the diagnosis of early-onset neonatal sepsis. Mothers delivering at term had circulating PCT concentrations similar to those observed in the apparently healthy adult population (1, 3 ). The maternal concentration of PCT did not appear to be affected by pregnancyrelated disorders, mode of delivery, use and type of anesthesia, duration of active labor, and stressful labor. Importantly, although maternal GBS colonization per se or rupture of membranes ⱖ18 h per se appeared to be associated with a significant increase in the neonatal PCT concentration at or after birth, neither risk factor was associated with a significant increase in maternal PCT concentration at the time of delivery. Possibly the fetal compartment responds differently than the maternal compartment in the presence of such infectious risk factors. Future studies would be useful to clarify the role of maternal serum PCT in preterm and term labor under conditions of clinically overt or subclinical chorioamnionitis. References 1. Assicot M, Gendrel D, Carsin H, Raymond J, Guilbaud J, Bohuon C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet 1993;341:515– 8. 2. Al-Nawas B, Krammer I, Shah PM. Procalcitonin in diagnosis of severe infections. Eur J Med Res 1996;1:331–3. 3. Meisner M. PCT, procalcitonin–a new, innovative infection parameter. Berlin: Brahms Diagnostica, 1996:1– 80. 4. Chiesa C, Pacifico L, Mancuso G, Panero A. Procalcitonin in pediatrics: overview and challenge. Infection 1998;26:236 – 41. 5. Hatherill M, Tibby SM, Sykes K, Turner C, Murdoch IA. Diagnostic marker of infection: comparison of procalcitonin with C reactive protein and leucocyte count. Arch Dis Child 1999;81:417–21. 6. Gendrel D, Raymond J, Coste J, Moulin F, Lorrot M, Guérin S, et al. Comparison of procalcitonin with C-reactive protein, interleukin 6 and interferon-␣ for differentiation of bacterial vs. viral infections. Pediatr Infect Dis J 1999;18:875– 81. 7. Gendrel D, Assicot M, Raymond J, Moulin F, Francoual C, Badoual J, Bohuon C. Procalcitonin as a marker for the early diagnosis of neonatal infection. J Pediatr 1996;128:570 –3. 8. Monneret G, Labaune JM, Isaac C, Bienvenu F, Putet G, Bienvenu J. Procalcitonin and C-reactive protein levels in neonatal infections. Acta Paediatr 1997;86:209 –12. 9. Chiesa C, Panero A, Rossi N, Stegagno M. De Giusti M, Osborn JF, Pacifico L. Reliability of procalcitonin concentrations for the diagnosis of sepsis in critically ill neonates. Clin Infect Dis 1998;26: 664 –72. 10. Lapillonne A, Basson E, Monneret G, Bienvenu J, Salle BL. Lack of specificity of procalcitonin for sepsis diagnosis in premature infants [Letter]. Lancet 1998;351:1211–2. 1587 11. Sachse C, Dressler F, Henkel E. Increased serum procalcitonin in newborn infants without infection. Clin Chem 1998;44:1343– 4. 12. Petzold L, Guibourdenche J, Boissinot C, Benoist J-F, Luton D, Demelier J-F, Porquet D. Apport de la procalcitonine dans le diagnostic des infections materno-foetales. Ann Biol Clin 1998; 56:599 – 602. 13. Maire F, Héraud MC, Loriette Y, Normand B, Bègue RJ, Labbé A. Intérêt de la procalcitonine dans les infections néonatales. Arch Pédiatr 1999;6:503–9. 14. Franz AR, Kron M, Pohlandt F, Steinbach G. Comparison of procalcitonin with interleukin 8, C-reactive protein and differential white blood cell count for the early diagnosis of bacterial infections in newborn infants. Pediatr Infect Dis J 1999;18:666 –71. 15. LeMoullec JM, Jullienne A, Chenais J, Lasmoles F, Guliana JM, Milhaud G, Moukhtar MS. The complete sequence of human preprocalcitonin. FEBS Lett 1984;16:93–7. 16. Sachse C, Dressler F, Henkel E. Usefulness of procalcitonin in neonates at risk for infection [Letter]. Clin Chem 1999;45:441. 17. Brunkhorst FM, Heinz U, Forycki ZF. Kinetics of procalcitonin in iatrogenic sepsis. Intensive Care Med 1998;24:888 –9. 18. Weinschenk NP, Farina A, Bianchi DW. Neonatal neutrophil activation is a function of labor length in preterm infants. Pediatr Res 1998;44:942–5. 19. American Academy of Pediatrics, Committee on Infectious Diseases and Committee on Fetus and Newborn. Revised guidelines for prevention of early-onset group B (GBS) streptococcal infection. Pediatrics 1997;99:489 –96. 20. Krohn MA, Hillier SL, Baker CJ. Maternal peripartum complications associated with vaginal group B streptococci colonization. J Infect Dis 1999;179:1410 –5. 21. Van Lente F, Pippenger CE. The pediatric acute care laboratory. Pediatr Clin North Am 1987;34:231– 46. 22. Mizuno S. Granulocyte colony-stimulating factor and neonatal infection [Letter]. J Pediatr 1997;130:844 –5. 23. Brunkhorst FM, Eberhard OK, Brunkhorst R. Discrimination of infectious and noninfectious causes of early acute respiratory distress syndrome by procalcitonin. Crit Care Med 1999;27: 2172– 6. 24. Nijsten MWN, Olinga P, Hauw The T, de Vries EGE, Schraffordt Koops H, Groothuis GMM, et al. Procalcitonin behaves as a fast responding acute phase protein in vivo and in vitro. Crit Care Med 2000;28:458 – 61. 25. Dandona P, Nix D, Wilson MF, Aljada A, Love J, Assicot M, Bohuon C. Procalcitonin increase after endotoxin injection in normal subjects. J Clin Endocrinol Metab 1994;79:1605– 8. 26. Ugarte H, Silva E, Mercan D, De Mendonça A, Vincent J-L. Procalcitonin used as a marker of infection in the intensive care unit. Crit Care Med 1999;27:498 –504. 27. Martin-Denavit T, Monneret G, Labaune JM, Isaac C, Bienvenu F, Putet G, Bienvenu J. Usefulness of procalcitonin in neonates at risk for infection [Letter]. Clin Chem 1999;45:440 –1.