Anorectal Malformations
advertisement

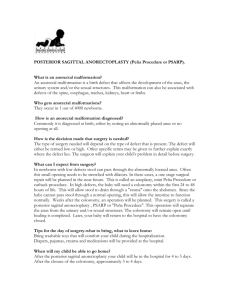
Anorectal Malformations Dr Hasan Nugud Consultant Paediatric Surgeon Anorectal Mlaformations Examination of the Perineum Anal opening Absent Present Normal Abnormal Normal size catheter can be passed Catheter cannot be passed beyond 2-3 cms Normal anus Rectal atresia Anal opening is very small Anal stenosis “microanus” Anal opening covered by skin bridge “Bucket handle” anomaly Perineal inspection •Anal dimple = EAS (cutaneoanal reflex, EMG) •Fistula visible? •Midline groove between buttocks and anal dimple (“flat buttocks”) decreased prominence ~ height of the fistula •Boys: –meconium or squamous epithelium in urine = fistula –white epithelial pearls = fistula •Girls: number of orifices + probing Anorectal Mlaformations Examination of the perineum Absent anal opening Anal dimple + Cough impulse + Low anomaly -normal skin -no meconium is seen Covered anus -Flat perineum -no natal cleft -no anal dimple -no cough impulse High anomaly -covered by -Fistulus opening in the a membrane meconium can perineum, be seen through median raphae, or scrotum, -meconium discharge Covered anus Anocutaneous fistula Anorectal Mlaformations Examination of the Perineum Abnormal anal opening Vestibule Perineum Ectopic anus Direction of the track Direction of the track Posterior Anocutaneous Fistula Upwards Rectocutaneous Fistula Posterior Anovestibular Fistula Upwards Rectovestibular Fistula Anorectal Mlaformations Examination of the Perineum High Anomaly Boys Girls Examination of genitalia Urine One opening Meconium stained Rectourethral Fistula Normal No Fistula Cloaca Meconium is passed per vagina Rectovaginal Fistula Two openings No meconium passed per vagina Rectal atresia Without fistula Anorectal Mlaformations Meconium is passing from the vestibule just anterior to the poster forshette and behind the posterior vaginal wall. Careful negotiation of the fistula track and meticulus dilataion defltes the baby and resolves distension Anorectal Mlaformations The rectal opening follows a subepithelial fistula tract in the midline raphe extending on the scrotum (may extend and involve the foreskin midline raphe) Black or white ribbon in the midline raphe presumes low anorectal malformarion. Anorectal Mlaformations Note the vaginal opening (the hymen) forward to the fistula which is wide and functioning Anorectal Mlaformations -Flat buttocks -No fistula can be notissed in the perineum - Impression high anomally Anorectal Mlaformations Wangensteen and Rise Invertogram PC Pubococcygeal line Ischial line (blue arrow) Intermediate line (white arrow) Note the end rectal shadow above the PC line indicating high anomally pattern Anorectal Mlaformations Wangensteen Rice Invertogram Marker Marker Stomach High Imperforate Anus with Dudenal atresia N.G.T. Prone cross-table lateral X-ray PC line and I point = levator complex •After 24 hours! •Wait 3 minutes in this position •Accurate centering on greater trochanter •Cave meconium plugs, crying, levator muscle contraction PC line and I point = levator complex Anorectal Mlaformations In normal individuals, the voluntary striated muscle structures responsible for fecal control are represented by a funnel-like muscle structure that inserts in the pubic bone, the lowest part of the sacrum and the middle portion of the pelvis. From there, this diaphragm-like muscle structure extends medially, surrounding the rectum all the way down to the perianal skin. The upper portion of this funnel-like structure is known as the “levator muscle”, and the lower portion as the “external sphincter”. Anorectal Mlaformations Different slings and subdivisions of these structures have been described, including the “ischiococcygeus”, “ileococcygeus”, “pubococcygeus”, “puborectalis”, “deep external sphincter”, and “superficial external sphincter”. Experience obtained through posterior sagital exploration of normal individuals with pelvic tumors, demonstrates continuum of striated muscles that run around the rectum and parallel to it down to the skin. Anorectal Mlaformations The external sphincter is parasagital muscle fibers that meet anterior and posterior to the anus. The levator muscle fibers come from upper insertion and run parallel to the rectum (perpendicular to the parasagital fibers). The upper portion of the funnel is the (levator muscle), the lower portion is the (external sphincter), while the intermediate portion, vertical, fibers, is the (muscle complex). Anorectal Mlaformations The internal sphincter in a normal individual is represented by the thickening of the circular layer of the smooth involuntary muscle of the bowel located in the anorectal area. The internal sphincter is present in patients with anorectal malformations regardless of the height of the defect. This involuntary sphincter seems to be located in the most distal part of the rectum. Very high defects are associated with abnormal sacrums and poor muscle development. Anorectal Mlaformations The genitourinary tract is the most serious and frequent of associated defects in anorectal malformations. It is true that the higher the malformation (cloaca or rectovesical fistula), the more frequently is associated with severe urologic problems, Anorectal Mlaformations The sacrum is frequently abnormal, Sacral vertebrae may be deformed or reduced in number, It is well known that the absence of more than three sacral vertebrae is associated with severe neurogenic deficit including neurogenic bladder and lack of bowel control, The upper spine frequently shows hemivertebrae. Anorectal Mlaformations The normal descent of the rectum has been halted, therefore the parasagital fibers get closer together in the midline. Below the lowest part of the rectum all the striated muscle meet together forming a solid mass of muscle. It’s length depends on the height of the defect of anorectal malformation. The lower the defect the shorter the mass of muscles and the wider the funnel-like muscle structure. Anorectal Mlaformations M Male Newborn with Anorectal malformation Perianal Inspection And Urinalysis Clinical evidence 80-90 % Questionable 20-10 % Anorectal Mlaformations Clinical evidence 80 – 90 % Perianal fistula “Bucket handle” Midline raphe fistula Anal stenosis Anal membrane Flat buttom Meconium in urine Air in bladder Colostomy Minimal PSARP Newborn No colostomy PSARP Anal stenosis Bucket handle Anal membrane Covered anus Anorectal Mlaformations Questionable 20-10% Wangensteen and Rice Invertogram > 1 cm bowel-skin distance Colostomy 4-8 weeks rule out Associated malf. Verify normal growth < 1cm bowel-skin distance PSARP Minimal PSARP Newborn No colostomy Anorectal Mlaformations Perineal inspection in female babies with anorectal malformations is more valuable than in male patients, e.g. single perineal orifice is a cloaca where 90% of them having an associated urological defect which needs urgent urological intervention. Such a patient may need urgent colostomy and sometimes vesicostomy, Imperforate anus without a fistula is very rare in female patients. Anorectal Mlaformations Female Newborn with Anorectal Malformations Perineal Inspection Fistula (approximately 90%) No fistula (approx. 10%) Anorectal Mlaformations Fistula (90%) Cloaca Emergency UT evaluation Colostomy and if nessecary Vesicostomy, Vaginostomy, or other urinary diversion 6 month Cutaneous Perineal Vagainal or Vestibular Minimal PSARP Newborn No colostomy Colostomy PSARVUP 4-8 weeks, rule out Associated malFormations, Verify normal growth PSARP Vestibular fistula Common wallbetweenrectum andvagina Anorectal Mlaformations No Fistula (10%) Wangensteen Rice invertogram < 1 cm bowel-skin distance Minimal PSARP Newborn No colostomy > 1 cm bowel-skin distance 4-8 weeks, rule out assoc. malform. Verify normal growth Colostomy PSARP International classification for anorectal malformations (Krickenbeck) Major clinicalgroups –All: •No fistula •Anal stenosis •Perineal (cutaneous) fistula •Rectovesical fistula –Female: •Vestibularfistula •Cloaca –Male: • Rectourethralfistula •Bulbarfistula •Prostatic fistula Imaging –Prone cross-table lateral film –Cystourethrography –Ultrasound abdomen •Kidney, pelvis (genitourinary) –Transperineal ultrasonography for location of distal rectal pouch (> 15 vs. < 15mm) and fistula –Echocardiography –Spine •X-ray spine •X-ray pelvis-sacrum •US spine for detection of spinal dysraphism •MR spine Sacral ratio cave pelvic tilting Normal sacral ratio: a/b ≥0.74 (anteroposterior) If sacral ratio < 0.5: bad prognostic sign for ultimate continence Anorectal Mlaformations Distal Colostogram prior to the final repair to determine the precise type of the anatomical defect as it has important prognosis and therapeutic implications. Using Foley catheter, through distal stoma with balloon inflated, with the patient on the lateral position, hydro-soluble contrast injected using pressure to overcome the contraction of the funnel-shaped muscle structure that surrounds the lowest part of the rectum to see the real fistula site. Anorectal Mlaformations During distal colostogram, the lower the defect, the more hydrostatic pressure the surgeon must apply to fill up the distal part of the colon, The study must be done preferably with video, No MCUG is needed as the bladder will be filled through the fistula, In addition to the distal colostogram, it may be necessary to inject die through the single orifice in the perineum in order to fill the three structures that constitue the cloaca (Bladder, Vagina, Rectum). Voiding cystourethrography •Antegrade urethrogram + retrograde whilst removing the catheter •In all patients –Renal tract anomalies? –Fistula? (but less reliable than colostogram) Anorectal Mlaformations Male defects as in all anorectal malformations are part of a wide spectrum that goes from a very low and simple malformation (perineal or cutaneous fistula) to the extremely complex malformation (with a rectobladder neck fistula). In between these two extremes are, the recto-urethral bulbar fistula and rectourethral prostatic fistula. However, most anorectal defects in male fall within these four categories and it must be remembered that the surgeon is dealing with spectrum. Anorectal Mlaformations Imperforate anus Note passage of meconium through the urethra Can be any of the wide range of high or intermediate type of recto urethral fistula Rectovesicalfistula •= rectobladder Rectovesical fistula •= rectobladder neck fistula •Flat perineum •Sacrum and pelvis can appear dysmorphic Anorectal Mlaformations Moving more towards the simpler side of the spectrum (low), there is a better chance of having a normal sacrum, good muscles, and a good looking perineum, While moving towards the complex side (high), the chances significantly worsen. Very poorly developed sacrum, and therefore poor innervation, underdeveloped muscles, narrow pelvis and decreased potential for continence. Anorectal Mlaformations Only recto-bladder fistula will require an abdominal approach in addition to posterior sagital approach, The rest can be repaired only through posterior sagital incision, Low anomalies are repaired by minimal posterior sagital anoplasty. Anorectal Mlaformations In low defects the rectum opens in the perineum anterior to the center of the external sphincter, with most of the rectum passing through the funnel-like muscle mechanism, intimately attached to the posterior urethra, with only the most distal part of the rectum anteriorly deviated, The perineal fistula usually causes obstruction because it is very narrow Anorectal Mlaformations Many times the rectum does not open directly into the perineum, but rather follows a subepithelial fistula tract in the midline raphae, opening somewhere, at the base of the scrotum, at the scrotum itself, at the base of the penis, or even at the foreskin, Therefore, a “black ribbon” type of structure located in the midline raphae, should alert the surgeon of the presence of one of these low defects. Anorectal Mlaformations Black ribbon -Perineal cutaneous Fistula -Covered anus -Incomplete commonest male fistula “White epithelial pearl” Anorectal Mlaformations Anal membrane is a thin epithelial layer covering the anus, through which the meconium can be seen. Simple excision of the membrane solves the problem, The so called “Bucket handle” malformation, is a prominent midline skin tag, below which a fine instrument can be passed as an evidence of a low defect type and no other studies are required to make the diagnosis. Anorectal Mlaformations It is important to place a Foley catheter in the bladder before prone positioning for operation with the pelvis elevated Protective colostomy is not necessary , The dissection is carried out very carefully, particularly in the anterior aspect of the rectum to prevent urethral damage, The electrical stimulator proved to be very effective and helpful in identifying all striated muscle structures and preserving them intact with dissection in the midline. Anorectal Mlaformations Imperforate anus without fistula (5%). In both males and females the rectal end lay about 2 cm from the perineal skin, Most of these patients have good sacrum and good muscles with good prognosis, Despite the fact that there is no fistula, rectum and urethra share a common wall and have intimate contact requiring sub-mucosal dissection to separate the rectum from the urinary tract, Rectal atresia and stenosis are very unusual in males. Anorectal Mlaformations Of female spectrum of defects, the simplest is the perineal or cutaneous fstula with a very obvious good plain of separation between the rectum and the vagina. The rectum passes through most of the muscle mechanism and is only deviated anteriorly in it’s most distal part. The fistula opens in the middle of the perineal body, and therefore is called perineal or cutaneous fistula. Anorectal Mlaformations Anorectal malformation Note the position of the anal opening Can be mistaken for recto-vaginal fistula (two openings or Recto-vestibular fistula (three openings) Also note the place of the normal anus (arrow) Anorectal Mlaformations Next in complexity is the vestibular fistula. Quality wise, muscles and sacrum could be compared to the recto-urethral bulbar fistula in males with good prognosis. The characteristic part of this defect is that, the anterior rectal wall and the posterior vaginal wall fuse together into a simple common wall without a distinctive plain of separation. The fistula is located within the vestibular mucosa immediately behind the hymen. Protective colostomy is safer with Limited PSARP. Anorectal Mlaformations Few patients fall between the perineal fistula and the vestibular fistula and they are called fourchette fistula where the opening is located between the mucosa of the vestibule and the perineal skin. The cutaneous fistula does not require a colostomy, on the other hand patients with vestibular fistula, require a protective colostomy prior to the main repair (in both limited PSARP). fourchette fistula where the opening is located between the mucosa of the vestibule and the perineal skin. Anorectal Mlaformations Low vaginal fistula can not be seen even by separating the labia in a baby girl. Meconium seems to be coming from deep inside the vagina, Posterior rim of the hymen is not visible, Common vagina and ractal wall immediately above the fistula, Low vaginal fistula indicates that the fistula opens in the lower part of the vagina, but in fact it is not a synonym for low defect. Anorectal Mlaformations High vaginal fistula is equivalent to the recto bladder neck fistula seen in males, Muscle and sacrum quality are significantly poor, A good distal colostogram will demonstrate the fistula, Abdominal approach is required with a full posterior sagital anorectoplasty, Many require tapering of the bowel. Anorectal Mlaformations Rectal atresia (blind, usually separated by a very thin membrane or fibrous tissue), or stenosis (partially communicating), are located at the natural limit of rectum and anal canal (immediately above the pectinate line), with normal looking external anus, and anal canal not deeper than 1-2 cm, discovered by a nurse while taking temperature. Anorectal Mlaformations Rectal atresia or stenosis are rare anorectal malformations and usually seen in females, They have good prognosis if they are treated properly, because they have all necessary elements responsible for bowel control, Treatment consists of posterior sagital incision. Both upper and lower bowel ends are opened and reconnected with a wide anastamosis. Anorectal Mlaformations The main characteristic of this defect is the confluence of rectum, vaqgina and urinary tract into a single channel or persistent cloaca, The surgical management of a persistent cloaca represents the most serious technical challenge in pelvic paediatric surgery. Anorectal Mlaformations The length of the common channel varies from 2 to 7 cm (typical cloaca with short channel, or high cloaca with long channel), Muscle complex and external sphincter are located in a normal site, posterior to the single cloacal opening in the perineum, which is usually located at the site of normal urethral orifice, The genitalia look smaller than in a normal baby, (imperforate anus with small looking genitalia on a baby girl should alert the physician to this defect). Anorectal Mlaformations The degree of sacral abnormalities and muscle deficiencies, usually varies along with the height of the defect. High cloacas (3-7 cm long common channel), are more frequently associated with an abnormal sacrum and poor muscles. Presents a serious challenge for the pullthrough of the rectum, for the vaginal repair (not enough tissue to mobilize and repair the vagina) with prognosis not as good as in other types of cloaca. Anorectal Mlaformations High incidence of associated urological abnormalities, with the high type long common channel cloaca, such as ; hydronephrosis, megaureters, reflux, renal dyspalsty, renal agenesis and neurogenic bladder. Anorectal Mlaformations Very low type of cloaca (length of common channel 0.5 to 1.5 cm), called recto-low vaginal fistula, associated with female hypospadias, The ideal treatment is to separate the rectum from the cloaca, locating it within the external sphincter, and leaving the genitourinary portion of the defect untouched, (only two perineum openings) continue Anorectal Mlaformations The patient will be left with a high urethral opening at the anterior wall of the vagina (female hypospadias), with excellent functional prognosis, Their separation from the functional point of view ( to achieve complete repair), is not absolutely necessary. Anorectal Mlaformations Hydrocolpos is frequently seen in cloacas. Very large vagina, distended and filled with fluid, promoting UT obstruction and subsequent frequent UTI, which dramatically improves after surgical drainage of the vagina, Presence of hydrocolpos represents an advantage in terms of vaginal reconstruction, because the surgeon can use all the extra tissue of the enlarged vagina in the vaginal pullthrough Anorectal Mlaformations Sometimes urine passes from the short proximal urethra directly into the distended vagina and subsequently during the day the urine dripples out constantly from the vagina simulating incontinence (pseudourinary incontinence) which is changed to normal voiding pattern after total repair of this kind of defect in cases with normal sacrum Anorectal Mlaformations Another type of frequent cloacas is the one with double vagina and double uterus or partially bicornate uterus, with partial or complete vaginal septum, Unique oportunity exists to surgically fuse together both vaginas creating one. Anorectal Mlaformations In the newborn before colostomy, full urological evaluation to rule out the frequently associated urinary tract obstruction is mandatory, to treat it if any with colostomy in the same session, It is considered an error to establish a colostomy in a patient with a cloaca without being aware of associated urological defects, The total repair of the cloaca is carried out usually when the baby is 6 months old provided the baby growing and developing normally. Anorectal Mlaformations The operating surgeon must remember that the rectum and vagina share a common wall, but most importantly , the vagina and the urethra also share a common wall, No attempt is made to place a Foley catheter into the bladder prior to the operation because there is no control of the direction of the catheter through a single common channel. Anorectal Mlaformations In those cloaca cases where the vagina does not reach the perineum, the surgeon may use one of the following maneuvers : Skin or labia flap to fill a 1 or 2 cm gap, Vaginal replacement with a vascularized piece of intestine for long gap or total vaginal replacement, Vaginal dome flap in those cases with long common channel associated with a very large but high vagina (hydrocolpos). (Anterior) ectopic anus •Abnormally located anus, Scrotum mainly in girls –Girls: anal index < 0.34 –Boys: anal index < 0.46 •Surrounded by internal and external sphincter •Problem Constipation •In most cases no surgery needed Associated anomalies (1) • More associated anomalies in high lesions • Serious, potentially lethal defects • Vertebral - spinal deformities – hemivertebrae – sacral deformities – caudal regression syndrome – tethered cord? • skin lesion: lump, vascular nevus, sinus, angioma on the midline of the back, hypertrichosis, skin dimple, sacral lipoma • neurological or neuro-orthopedic abnormalities of lower extremities, scoliosis Neural tube defect of terminal spinal cord: • bladder and bowel dysfunction permanent - Vertebral abnormalities - Flat buttocks colostomy - Lower limb neurological deficit - Neurogenic bladder - ARM Male Perineal repair Cutback anoplasty Perineal operation (Browne, Potts 1954) –Cutback anoplasty (Browne) Colostomy formation Later high-pressure colostogram Stoma Mucus fistula Anorectal Mlaformations International groupingof surgical procedures (Krickenbeck) •Pull-through abdominoperineal (Rhoads, 1948) •Sacroperineal approach (Stephens 1953) •Perineal operation (Browne, Potts 1954) –Cutback anoplasty (Browne) –“Potts transfer anoplasty” •Pull-through abdominosacroperineal (Kiesewetter 1966 , Rehbein 1967) •PSARP (Peña-deVries, 1982) •Anterior sagittal approach (Mollard, 1989, Okada, 1992) •Pull-through laparoscopic-assisted (Georgeson, 2000) Anorectal Mlaformations PSARP Proper comfortable positioning Anorectal Mlaformations PSARP Anorectal Mlaformations Indicators of prognosis for bowel control in ARM patients Anorectal Mlaformations Conclusions •A good, simple classification is crucial for adequate comparison of data •Surgical and prognostic relevance •“high and low”is too general •Ectopic anus is not the same as ectopic anal canal •Multidisciplinary collaboration •Pediatrician, pediatric surgeon, radiologist, nursing team, psychologist, physiotherapy, stoma nurse… •Preoperative work-up •Meticulous surgical technique •Postoperative follow-up into adulthood •GI, urinary, sexual, psychosocial THANKS