From www.bloodjournal.org by guest on March 4, 2016. For personal use only.
LYMPHOID NEOPLASIA
Mutated RAS and constitutively activated Akt delineate distinct oncogenic
pathways, which independently contribute to multiple myeloma cell survival
Torsten Steinbrunn,1 Thorsten Stühmer,1 Stefan Gattenlöhner,2 Andreas Rosenwald,3 Anja Mottok,3 Christian Unzicker,1
Hermann Einsele,1 Manik Chatterjee,1 and Ralf C. Bargou1
1Department of Internal Medicine II, Division of Hematology and Medical Oncology, and Comprehensive Cancer Center Mainfranken, University of Würzburg,
Würzburg, Germany; 2Institute of Pathology, Medical University of Graz, Graz, Austria; and 3Institute of Pathology, University of Würzburg, Würzburg, Germany
We have recently shown that approximately half of primary multiple myeloma
(MM) samples display constitutive Akt
activity, which disposes them for sensitivity to Akt inhibition. The Akt pathway
counts among the signaling conduits for
oncogenic RAS and activating mutations
of K- and N-RAS frequently occur in MM.
We therefore analyzed the relation between RAS mutation and Akt dependency
in biopsies and CD138-purified cells from
MM patients (n ⴝ 65) and the function of
oncogenic RAS for MM cell survival in a
range of MM cell lines with differing RAS
status. Whereas RAS mutations do not
predict Akt dependency, oncogenic RAS
retains an important role for MM cell
survival. Knockdown of either K- or
N-RAS strongly decreased the viability of
MM cells that harbored the respective
oncogenic isoform, whereas ablation of
wild-type RAS isoforms had little or no
effect. Silencing of oncogenic RAS did
not affect the Akt pathway, again indicat-
ing lack of a direct link. Combined inhibition of RAS and Akt strongly enhanced
MM cell death. These data suggest that
oncogenic RAS and Akt may independently contribute to MM cell survival. Targeting of both pathways could provide an
attractive therapeutic strategy for patients with oncogenic RAS and dysregulated Akt signaling. (Blood. 2011;117(6):
1998-2004)
Introduction
Multiple myeloma (MM) is an incurable neoplasia of the terminally differentiated plasma cell and accounts for approximately
10% of all hematologic cancers.1 Intrinsic genetic lesions as well as
the bone marrow microenvironment contribute to the activation of
proliferation and survival pathways, impairment of cell death
mechanisms, and drug resistance.2-5 Two pathways commonly
dysregulated in MM involve activation of the serine/threonine
kinase Akt (Akt pathway) and of the guanine nucleotide exchange
factor RAS (RAS/MAPK pathway). The Akt pathway has repeatedly been found to be important for MM cell survival,6,7 and we
have recently shown that approximately 50% of primary MM
samples display an Akt-dependent, phospho-Akt-positive phenotype.7 Little is known about the mechanisms that lead to constitutive Akt activation in MM, but suitable genetic lesions, such as
deletion of PTEN8,9 or activating mutations of PIK3CA,10,11 appear
to be relatively rare in this disease. Conversely, the reported
prevalence of activating mutations of K- and N-RAS in MM ranges
from approximately 30% to 50% of patient samples.12-17 The
occurrence of RAS mutation appears independent of clinical
stage,13,17 but oncogenic RAS is associated with disease progression, aggressive phenotype, and shorter survival.12,17-19 It is also
implied in the transition to MM because RAS mutations are rarely
found in monoclonal gammopathy of undetermined significance.13,16 However, analyses of the functional role of oncogenic
RAS in MM are rare, mainly because of the entire lack of specific
inhibitors. Prenylation blockers, such as farnesyltransferase inhibitors, had initially been developed to curb RAS signaling. Encouraging preclinical data, however, did not translate into clinical
efficiency, and it has subsequently been shown that the observed
effects were largely independent of oncogenic RAS.20-23 It has been
reported that ectopic overexpression of oncogenic RAS induces
MM cell proliferation24 and lowers drug efficacy.25 However, it is
unknown whether endogenous oncogenic RAS still contributes to
the malignant phenotype of clinically overt MM and whether it
therefore constitutes a potential therapeutic target in its own right.
Because oncogenic RAS is a potential activator of the PI3K/Akt
signaling axis,26-29 we investigated the correlation between RAS
mutation and presence of/dependence on activated Akt in primary
MM samples. We also used knockdown approaches in MM cell
lines to assess the effects of oncogenic RAS depletion on MM cells.
We show that isoform-specific knockdown of RAS reduces the
viability of MM cells harboring the respective oncogenic K- or
N-RAS mutation, whereas little or no effects are seen when RAS
isoforms are lost against a wild-type background. Because RAS
mutation was not predictive for sensitivity to Akt blockade and
knockdown of oncogenic RAS did not affect Akt activation,
constitutively activated RAS and Akt appear to contribute independently to MM cell survival. These observations might have direct
implications for the development of targeted therapies in MM.
Submitted May 10, 2010; accepted November 24, 2010. Prepublished online
as Blood First Edition paper, December 13, 2010; DOI 10.1182/blood-2010-05284422.
The publication costs of this article were defrayed in part by page charge
payment. Therefore, and solely to indicate this fact, this article is hereby
marked ‘‘advertisement’’ in accordance with 18 USC section 1734.
The online version of this article contains a data supplement.
© 2011 by The American Society of Hematology
1998
Methods
Cell culture and primary MM cells
The human MM cell lines AMO-1, JJN-3, and U266 were obtained from the
German Collection of Microorganisms and Cell Cultures (DSMZ). MM.1S
BLOOD, 10 FEBRUARY 2011 䡠 VOLUME 117, NUMBER 6
From www.bloodjournal.org by guest on March 4, 2016. For personal use only.
BLOOD, 10 FEBRUARY 2011 䡠 VOLUME 117, NUMBER 6
cells were purchased from LGC Biolabs (ATCC-CRL-2974). Cell line
INA-6 was a gift from Prof Martin Gramatzki (Kiel, Germany). MM cell
culture conditions and acquisition of primary MM cells are described in
detail by Stühmer et al.30 All cell cultures were regularly tested for
mycoplasma. Bone marrow aspirates from myeloma patients were obtained
after informed consent. Permission was granted by the Ethics Committee of
the Medical Faculty of the University of Würzburg, Würzburg, Germany
(reference no. 73/05).
Application of drugs
MM cells were seeded in 100 L full medium in 96-well-plates. An equal
amount of medium was added containing the respective drug in double
concentration. Control incubations with dimethyl sulfoxide were always
included. Akti-1,2 was obtained from Merck, and PD184352 was from
Axon Medchem.
Cell viability assay
The fraction of apoptotic cells was identified by flow cytometry as
described before.31 Briefly, cells were washed in phosphate-buffered saline,
stained with propidium iodide and annexin V-fluorescein isothiocyanate or
annexin V-allophycocyanin (Bender MedSystems), and analyzed using a
FACSCalibur with CellQuest software Version 5.2 (BD Biosciences).
ONCOGENIC RAS AND Akt IN MULTIPLE MYELOMA
1999
sion vector34 (pCAGGS/SE-HA-K-RAS wt). This construct produced
considerably better expression levels of HA-tagged K-RAS in MM cells.
To generate HA-tagged N- and H-RAS expression vectors, the Quik
Change II Site-Directed Mutagenesis Kit (Agilent Technologies) was used
to introduce an in-frame Bst1107I restriction site between the triple-HA-tag
and the K-RAS coding sequences in pBluescript-HA-K-RAS wt. Firststrand cDNA generated from U266 cells was used to amplify N- and H-RAS
genes with primers 5⬘-AGTCGTATACTGAGTACAAACTGGTGG-3⬘
(N-RAS forward), 5⬘-AGTCCTCGAGTTACATCACCACACATG-3⬘
(N-RAS reverse), 5⬘-AGTCGTATACGGAATATAAGCTGGTGG-3⬘
(H-RAS forward), and 5⬘-AGTCCTCGAGTCAGGAGAGCACACACT-3⬘
(H-RAS reverse). The primers introduce Bst1107I and XhoI restriction sites
(boldface type) to immediately flank the 5⬘- and 3⬘-ends of the coding
regions, and they lead to deletion of the native start codons. The genes were
cloned to replace K-RAS in pBluescript-HA-K-RAS wt and again transferred to pCAGGS/SE.
Point mutated forms of K-RAS (representing the mutation in MM.1S
cells) and N-RAS (as mutated in INA-6 cells; supplemental Table 1B,
available on the Blood Web site; see the Supplemental Materials link at the
top of the online article) were generated with the Quik Change II kit in the
respective pBluescript constructs described above, and subcloned into
pCAGGS/SE.
Transfection of MM cells by electroporation
RAS mutation analysis
Primary MM samples and cell lines were screened for K- and N-RAS
mutations at codons 12, 13 (both exon 2), and 61 (exon 3). A total of
105 cells from freshly isolated (CD138⫹ selected) patient samples or from
cultured MM cell lines were washed twice with ice-cold phosphatebuffered saline and either genomic DNA (using digestion buffer, pH
8, containing 5M NaCl, 1M Tris, 0.5M ethylenediaminetetraacetic acid,
10% sodium dodecyl sulfate, 0.1 mg/mL proteinase K, followed by
phenol-chloroform extraction) or total RNA (using the RNeasy Mini Kit,
QIAGEN) were prepared. cDNA was synthesized using the RevertAid
First-Strand cDNA Synthesis Kit (Fermentas). Polymerase chain reaction
was performed for 35 cycles, with 1 minute each for denaturation (94°C),
annealing (61°C), and extension (72°C). Polymerase chain reaction products were isolated from agarose gels and sequenced at LGC Genomics. The
following primers for amplification off of genomic DNA were used:
5⬘-ACCTTATGTGTGACATGTTC-3⬘ (K-RAS forward for exon 2), 5⬘AATGGTCCTGCACCAGTAAT-3⬘ (K-RAS reverse for exon 2), 5⬘GCACTGTAATAATCCAGACT-3⬘ (K-RAS forward for exon 3), 5⬘ATTACTCCTTAATGTCAGCT-3⬘ (K-RAS reverse for exon 3), 5⬘AGTACTGTAGATGTGGCTCG-3⬘ (N-RAS forward for exon 2), 5⬘TGATCCGACAAGTGAGAGAC-3⬘ (N-RAS reverse for exon 2), 5⬘CCTTGGCAATAGCATTGCAT-3⬘ (N-RAS forward for exon 3), and
5⬘-AATGCTCCTAGTACCTGTAG-3⬘ (N-RAS reverse for exon 3). For
amplification off of first-strand cDNA, the primers 5⬘-GCCTGCTGAAAATGACTGAA-3⬘ (K-RAS forward), 5⬘-CTTGCTAAGTCCTGAGCCTG-3⬘
(K-RAS reverse), 5⬘-TCTGTCCAAAGCAGAGGCAG-3⬘ (N-RAS forward), and 5⬘-GTGTCAGTGCAGCTTGAAAG-3⬘ (N-RAS reverse)
were used.
Construction of shRNA and HA-tagged RAS expression vectors
shRNA expression constructs were based on pSUPER.32 The following
target sequences were used: 5⬘-GTTGGAGCTGGTGGCGTAG-3⬘ (human
K-RAS wild-type33), 5⬘-GTTGGAGCTGCTGGCGTAG-3⬘ (K-RAS as mutated in cell line MM.1S), 5⬘-GTTGGAGCAGGTGGTGTTG-3⬘ (human
N-RAS wild-type), 5⬘-GTTGGAGCAGATGGTGTTG-3⬘ (N-RAS as mutated in cell line INA-6), and 5⬘-ACGAGGGGAGTACATCAAGAC-3⬘
(human Akt17).
A pcDNA3.1-based expression vector for N-terminally triple-hemagglutinin (HA)-tagged human K-RAS was purchased from the University of
Missouri-Rolla cDNA Resource Center (no. RASK20TN00). The insert
was excised by KpnI/XhoI digest and subcloned into pBluescript (SK)
(yielding plasmid pBluescript-HA-K-RAS wt), from which the insert was
transferred via KpnI/NotI digest into a modified pCAGGS protein expres-
AMO-1, INA-6, JJN-3, MM.1S, and U266 cells were washed and
resuspended in fresh, pure RPMI 1640 medium at a density of up to
1.5 ⫻ 107 cells/500 L. Transient transfection of shRNA and protein
expression vectors was performed at 950 F and 280 V (310 V for MM.1S
cells; Gene Pulser 2, Bio-Rad; in 4-mm cuvettes, PeqLab). AMO-1, JJN-3,
MM.1S, and U266 cells were cotransfected with an expression plasmid for
enhanced green fluorescent protein (pcDNA3.1-EGFP), INA-6 cells were
cotransfected with an expression plasmid for truncated CD4.31 Cells were
kept for one day in full RPMI 1640 medium with 10% fetal bovine serum,
and purification of strongly transfected cells was achieved either by CD4
microbead selection31 or by cell sorting of EGFP⫹ cells (MoFlo; Beckman
Coulter). For electroporation of control cells, shRNA-expressing pSUPER
constructs were substituted for the same amount of empty pSUPER vector.
For Western analyses, cells were harvested 2 days after electroporation.
After one wash in ice-cold phosphate-buffered saline, cell pellets were snap
frozen in liquid nitrogen and stored at ⫺80°C until further use.
Western analysis
Western blotting was performed essentially as described before.35 Briefly,
cell pellets were dissolved in 20 L of lysis buffer, protein concentrations
determined, and equal amounts mixed with Laemmli buffer run on sodium
dodecyl sulfate 10%-polyacrylamide gels before blotting on nitrocellulose
membranes. The antiHA-tag antibody (ab9110) was purchased from
Abcam, antiK-RAS (sc-30, lot A2309) and antiN-RAS antibodies (sc-31,
lot K1709) were from Santa Cruz Biotechnology. Antibodies detecting
pan-Akt (no. 9272), phospho-Akt (Ser473, no. 4058), phospho-Akt (Thr308,
no. 2965), ERK1/2 (no. 9102), phospho-ERK1/2 (no. 9101), phosphoFOXO1/3a (no. 9464), and phospho-GSK-3 (no. 9336) were purchased
from Cell Signaling Technology. Anti-actin antibody (A5316) was from
Sigma-Aldrich, anti␣-tubulin (no. 03568) was from Biozol. Secondary
antibodies specific for rabbit (no. 111–036-045), mouse (no. 115036-003),
or rat (no. 112036-062) were from Jackson ImmunoResearch Laboratories.
Immunofluorescent histochemical stainings of
bone marrow biopsies
To analyze the expression of phospho-Akt (Ser473) and of phospho-Akt
(Thr308) in MM cells, immunofluorescent stainings were performed for
either antigen in combination with detection of CD138 in formalin-fixed,
paraffin-embedded bone marrow biopsies heavily infiltrated with MM cells.
For both the CD138/phospho-Akt (Ser473) and the CD138/phospho-Akt
(Thr308) double stainings, the primary antibodies were derived from
different species. The following antibodies were used: anti-CD138 (M7728,
From www.bloodjournal.org by guest on March 4, 2016. For personal use only.
2000
STEINBRUNN et al
1:50 dilution; Dako Germany), anti-phospho-Akt (Ser473, no. 4060),
anti–phospho-Akt (Thr308, no. 4056; both in 1:100 dilution; Cell Signaling
Technology), donkey anti–mouse CY2 (no. 715–225-151), and donkey
antirabbit CY3 (no. 711–165-152; both in 1:1000 dilution; Dako Germany).
A typical staining protocol used antibody diluent as blocking reagent for
15 minutes, followed by incubation with primary antibodies for 1 hour and
with fluorescent dye-marked secondary antibodies for another hour. Between steps, slides were washed 3 times for 5 minutes in Tris-buffered
saline. After staining, slides were mounted with antifading medium
(Fluormount G; Biozol) and kept at 4°C in the dark. The slides were
reviewed and scored by an experienced hematopathologist. The percentage
of positive tumor cells (ie, cells carrying a signal for phospho-Akt within
the CD138⫹ tumor cell population) varied from 0% to 80% between cases.
An arbitrary cutoff of 20% positive tumor cells for at least one of the
2 phospho-Akt antibodies defined a case as positive or negative. Of the
34 positive cases, 15 showed positivity for both phospho-Akt (Ser473) and
phospho-Akt (Thr308), 9 showed reactivity for phospho-Akt (Ser473) only,
and 10 for phospho-Akt (Thr308) only. The average percentage of positive
tumor cells was 42% for all phospho-Akt (Ser473)-positive cases and
46% for all phospho-Akt (Thr308)-positive cases. The entire immunohistochemical evaluation of primary MM samples was conducted without any
knowledge of their RAS mutation status. Images were taken with a confocal
laser scanning system (Leica TCS SP2; Leica) connected to a Leica
DMRE microscope (original magnification ⫻400, objective HCX PL APO
40⫻/1.25-0.75 NA OIL CS; Leica), and imported into the Leica Confocal
Software Version 2.61, Build 1537. For each antibody combination, multiple
images were taken from different areas of the bone marrow trephine.
Statistical analysis
A 2-tailed Student t test was applied to perform statistical analysis of cell
viability assays. For categorical data, Fisher exact test was used. Results
were considered significant at P ⬍ .05. Calculations were performed with
IBM SPSS Statistics 18.
Results
RAS mutation status does not predict dependency on Akt in
primary MM
We have previously shown that the phospho-Akt status in MM cells
is largely predictive of cell death induction through inhibition of
Akt, and that for primary MM samples approximately 50%
displayed a phospho-Akt-positive/Akt inhibition-sensitive phenotype.7 Because a similar number has been reported for activating
mutations of RAS and oncogenic RAS is a potential upstream
activator of the PI3K/Akt pathway, we decided to analyze the
RAS/phospho-Akt status of primary MM samples (n ⫽ 65) and to
investigate the functional role of mutant RAS in MM cell lines.
Freshly isolated primary MM cells (CD138⫹ selection; purity ⬎ 95%) were treated with Akt inhibitor Akti-1,2 (10M), and
survival relative to dimethyl sulfoxide-treated controls was determined after 5 days in coculture with bone marrow stromal cells.
Simultaneously, the mutation status of K- and N-RAS genes was
determined by polymerase chain reaction off of genomic DNA
isolated from these samples and, where available, bone marrow
biopsies were retrospectively analyzed for the in situ presence of
phospho-Akt at positions Ser473 and/or Thr308 (Figure 1).
For all primary MM samples (n ⫽ 65), the genetic status of
K- and N-RAS was determined, and 25 samples (38.5%) were
found to harbor oncogenic point mutations, thus matching the
consensus based on published literature.12 Both genes were found
mutated with about the same frequency (12 K-RAS and 13 N-RAS
mutated samples). Twenty-five of these samples, of which
11 contained RAS mutations, could be evaluated for their sensitivity
BLOOD, 10 FEBRUARY 2011 䡠 VOLUME 117, NUMBER 6
against Akti-1,2 (Figure 1A). Comparing the distribution of
the survival rates between the RAS wild-type and RAS mutated
groups, we found no statistical correlation (P ⫽ .47, Student t test;
Figure 1A).
Correlation of these results with immunohistochemical detection of phosphorylated Akt (Ser473 and/or Thr308) in the matching
bone marrow biopsies, however, largely confirmed our previous
observations in that, of the 19 MM samples for which both
pharmacologic and immunohistochemical data were available, the
large majority of phospho-Akt-positive samples was sensitive to
Akt inhibition, whereas phospho-Akt-negative samples were mostly
resistant (P ⫽ .005, Student t test; Figure 1B). For the correlation
between phospho-Akt positivity in biopsies and the presence of
oncogenic RAS in the cognate MM samples, we found that mutant
RAS was present in 16 of 34 (47%) phospho-Akt-positive cases, as
well as in 8 of 25 (32%) phospho-Akt-negative samples (Figure
1C). These numbers do not imply a statistically significant correlation between the presence of oncogenic RAS and phospho-Akt
status (P ⫽ .29, Fisher exact test), although with the qualification
that at n ⫽ 59 the statistical power for these conclusions is still
limited. Collectively, these data suggest that oncogenic RAS is not
a primary driver of intrinsic Akt activity in MM.
Validation of isoform-specific shRNA expression constructs
against K- and N-RAS
Because of the lack of suitable inhibitors, it remains unclear
whether oncogenic RAS retains a functional role in MM. We
therefore decided to establish an isoform-specific knockdown
approach (ie, to investigate the loss-of-function consequences in
these gain-of-function phenotypes). Genetic analyses of 5 MM cell
lines suitable for transfection by electroporation showed that
AMO-1 and U266 cells are RAS wild-type, INA-6, and JJN-3 cells
display an activating N-RAS mutation, and MM.1S cells harbor
oncogenic K-RAS (supplemental Table 1B and supplemental
Figure 1; see legend to supplemental Figure 1 for comments on
discrepancies in the published RAS status for some of these cell
lines). Because of the high sequence homology of RAS isoforms at
protein as well as at DNA level, and to assess potential selectivity
for wild-type and mutant RAS alleles, it was mandatory to control
the specificity of the reagents. Complicating matters, isoformspecific RAS antibodies can display some cross-reactivity (supplemental Figure 2), and RAS proteins may be present in different
levels in different MM cells. We therefore cotransfected expression
vectors for HA-tagged wild-type and mutant RAS proteins to
assess the suitability of the allele- and isoform-specific shRNA
expression vectors. Both the K-RAS and the N-RAS-specific
knockdown constructs led to strong and selective depletion of their
respective target (Figure 2A). However, the constructs did not
distinguish between the wild-type and mutant alleles of either the
K-RAS (Figure 2B) or N-RAS isoform (data not shown), showing
that the single-base differences between target sequences were
insufficient to confer effective selectivity. The constitutively active
K- and N-RAS proteins are therefore of necessity always depleted
in concert with their respective wild-type twin.
Silencing of oncogenic RAS induces MM cell death
To assess the dependency of MM cells on oncogenic RAS, we
transfected each of the 5 MM cell lines (AMO-1, INA-6, JJN-3,
MM.1S, and U266) with K- or N-RAS knockdown constructs and
measured cell viability over the course of 5 days in culture.
Whereas the 2 RAS wild-type cell lines (AMO-1, U266) remained
From www.bloodjournal.org by guest on March 4, 2016. For personal use only.
BLOOD, 10 FEBRUARY 2011 䡠 VOLUME 117, NUMBER 6
ONCOGENIC RAS AND Akt IN MULTIPLE MYELOMA
2001
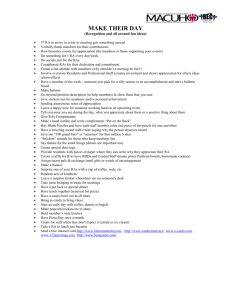
Figure 1. Analysis of RAS mutation and Akt activation in primary MM samples. (A) RAS mutation status and sensitivity to Akt blockade in freshly isolated primary MM cells
(n ⫽ 25). Viability measurements of MM cells cocultured with bone marrow stromal cells were performed after 5-day treatment with 10M Akti-1,2. Sensitivity to Akt inhibition
shows no obvious correlation with the presence or absence of RAS mutation. Medians are indicated. (B) Correlation between Akti-1,2 (10M) sensitivity of freshly isolated,
cocultured primary MM cells and the presence or absence of phospho-Akt in immunohistochemical stains of matched bone marrow biopsies (n ⫽ 19). Phospho-Akt positivity in
the biopsies was significantly (P ⬍ .05) correlated with sensitivity to Akt inhibition of the respective MM cells. (C) RAS mutation in primary MM cells and phospho-Akt status in
corresponding bone marrow biopsies (n ⫽ 59). RAS mutations were present in 16 of 34 phospho-Akt-positive and in 8 of 25 phospho-Akt-negative samples. (D) Two examples
of MM patient biopsies with immunofluorescent double staining for plasma-cell marker CD138 (green) and either phospho-Akt Ser473 or phospho-Akt Thr308 (both in red).
A phospho-Akt-negative (patient 6) and a phospho-Akt-positive (patient 20) sample are shown. Bar represents 75 m.
virtually unaffected by isoform-specific RAS depletion (Figure 3)
or by combined knockdown of K- and N-RAS (supplemental
Figure 3), the shRNA expression vectors led to decreased viability
specifically in those MM cells that harbor the respective oncogenic
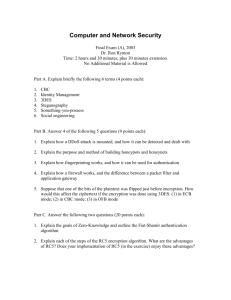
Figure 2. Verification of the isoform-specific shRNA
expression vectors. MM.1S cells were transiently transfected with expression vectors for HA-tagged K-, N-, or
H-RAS (1 g/mL, 10 g/mL, and 2 g/mL, respectively)
in combination with shRNA expression vectors against
either K- or N-RAS, or empty pSUPER vector (15 g/
mL). (A) Exemplarily shown are Western blots for wildtype RAS proteins in combination with shRNA expression constructs based on the wild-type RAS alleles.
Transfected cell fractions were purified and harvested
for Western blotting 2 days after electroporation. The
vertical white lines indicate that lanes representing a
nonfunctional H-RAS shRNA expression vector have
been deleted. (B) Expression of wild-type or mutant
(G12A; the mutation present in MM.1S) K-RAS in
MM.1S cells. Although allele-specific shRNA expression
vectors may show slightly better efficiency with their
perfect match, both lead to effective knockdown of
mutant or wild-type K-RAS, rendering mutation specific
knockdown impossible. -Actin served as loading control.
RAS isoform (Figure 3). Thus, knockdown of N-RAS entailed
significant cell death specifically in N-RAS mutated INA-6 (29%
viability relative to empty vector treated controls) and JJN-3 (46%
viability) cells. Conversely, MM.1S cells, which harbor oncogenic
From www.bloodjournal.org by guest on March 4, 2016. For personal use only.
2002
BLOOD, 10 FEBRUARY 2011 䡠 VOLUME 117, NUMBER 6
STEINBRUNN et al
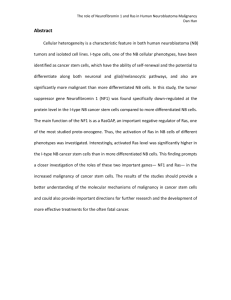
Figure 3. Isoform-specific shRNA-mediated RAS knockdown reduces cell
viability specifically in MM cell lines harboring the respective oncogenic
isoform. MM cells were transiently transfected with shRNA expression vectors
(20 g/mL) targeting K- or N-RAS and cell viability was measured after 5 days in
culture. N-RAS mutated cell lines INA-6 (G12D) and JJN-3 (Q61K) were specifically
sensitive to N-RAS knockdown, whereas K-RAS mutated MM.1S cells (G12A) were
most sensitive to K-RAS knockdown. The viability of MM cell lines AMO-1 and U266
(wild-type RAS) remained unaffected by knockdown of either RAS isoform.
K-RAS, were most sensitive to knockdown of K-RAS (39%
viability), although in this cell line a lesser effect was observed on
N-RAS depletion (67% viability), too (Figure 3). Of note, both the
respective mutation- and wild-type–directed shRNA expression
constructs produced largely similar results, as would be expected
from the fact that they do not discriminate between alleles
(supplemental Figure 4).
Knockdown of oncogenic RAS in MM.1S and JJN-3 cells
down-regulates signaling via the MAPK pathway but does not
affect levels of constitutively activated Akt
We analyzed the consequences of oncogenic K- or N-RAS
depletion on the activity of downstream signaling pathways in
MM.1S and JJN-3 cells, which display constitutive phosphorylation of ERK1/2 and of Akt. K-RAS knockdown in MM.1S and
N-RAS knockdown in JJN-3 cells markedly reduced the levels of
phosphorylated ERK1/2 but did not lead to notable decreases of
Akt phosphorylation at either Ser473 or Thr308 (Figure 4),
implying that oncogenic RAS may not signal via Akt and that in
turn the intrinsic Akt activity in MM.1S and JJN-3 cells is not
dependent on oncogenic RAS. Accordingly, the phosphorylation
levels of Akt substrates GSK-3 and FOXO1/3a were not affected
by K-RAS knockdown in MM.1S cells, either (Figure 4). Because
oncogenic RAS and Akt may therefore represent components of
2 independent survival pathways, we tested the effects of simultaneous inhibition of these proteins. An shRNA expression vector
against Akt1 (shown to be effectively inducing cell death in MM.1S
cells7) or the small molecule Akt1&2 inhibitor Akti-1,2 were
combined with the K-RAS knockdown vector (Figure 5). The
K-RAS mutant MM.1S cells, which are dependent on both K-RAS
and Akt, displayed significantly enhanced levels of cell death when
these proteins were down-regulated together (Figure 5 left). This
effect was also very prominent when K-RAS knockdown was
complemented with pharmacologic inhibition of Akt (Figure
5 middle). Contrarily, the viability of RAS wild-type AMO-1 cells,
which neither depend on RAS nor display constitutive activity of
Akt, was unaffected by combined knockdown of K-RAS and Akt1
(Figure 5 right).
Inhibition of MEK/MAPK alone does not recapitulate the effects
of RAS knockdown
The observation that knockdown of oncogenic RAS in MM.1S and
JJN-3 cells strongly decreased the levels of phospho-ERK1/2 led
us to examine to what extent oncogenic RAS might exert its
prosurvival effect via the MAPK pathway. Treatment of MM cells
with 10M of the MEK inhibitor PD184352 did not lead to
significant decreases in viability, even though at this concentration
the phosphorylation of the MEK substrates ERK1 and ERK2 is
completely and permanently blocked (supplemental Figure 5). The
prosurvival effect of constitutively active RAS in MM cells is
therefore not primarily mediated via the MEK/ERK module, again
underpinning that RAS represents a potentially useful therapeutic
target in its own right.
Discussion
Both the RAS/MAPK and the PI3K/Akt pathway have garnered
considerable attention for their presumed role in the pathogenesis
and potential suitability for therapeutic intervention in MM.36-38 We
have recently shown that Akt contributes to tumor cell survival in
approximately 50% of primary MM cases and that sensitivity to
Akt inhibition is predicted by the presence of constitutive Akt
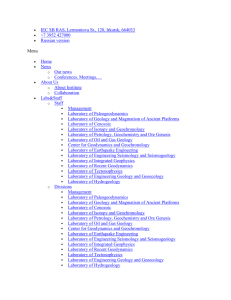
Figure 4. Western analysis of oncogenic RAS signaling. Knockdown of K-RAS in MM.1S cells (harboring an
activating G12A K-RAS mutation) or N-RAS in JJN-3
cells (harboring a Q61K N-RAS mutation) led to strongly
decreased levels of phosphorylated ERK1/2, indicative
of involvement of the RAS/MAPK pathway in oncogenic
RAS signaling. Phosphorylation levels of Akt and of its
substrates FOXO1/3a and GSK-3 were not significantly affected (shown for MM.1S cells only). Cells were
transfected with shRNA expression vectors (20 g/mL)
designed against either the mutant K-RAS allele (but
which also leads to knockdown of the wild-type protein),
or against both N-RAS alleles (the targeted sequence
does not match the position of the mutation at codon 61),
purified and harvested for Western analysis 2 days after
transfection. -actin served as loading control.
From www.bloodjournal.org by guest on March 4, 2016. For personal use only.
BLOOD, 10 FEBRUARY 2011 䡠 VOLUME 117, NUMBER 6
ONCOGENIC RAS AND Akt IN MULTIPLE MYELOMA
2003
Figure 5. Combined knockdown of oncogenic RAS and Akt enhances cell death in MM.1S cells. Simultaneous depletion of oncogenic
K-RAS and attenuation of Akt activity, either by shRNA-mediated knockdown (left) or by pharmacologic inhibition of Akt1 and 2 with Akti-1,2
(middle), significantly enhanced cell death in K-RAS mutated MM.1S
cells. The concentrations chosen for the expression vectors for K-RAS
shRNA (15 g/mL) and Akt1 shRNA (10 g/mL) and for Akti-1,2 (2.5M)
were such that an approximately medium size effect on the viability after
5 days in culture could be expected. RAS wild-type AMO-1 cells, which
are insensitive to Akt inhibition, were not significantly affected by either
single or combined knockdown of K-RAS and Akt1 (right).
phosphorylation.7 Because genetic lesions within the Akt pathway
are relatively rare in MM, we decided to investigate whether
oncogenic RAS is a main driver of intrinsic Akt activity and to
analyze its role for MM cell viability. Oncogenic RAS is a potential
upstream activator of the Akt pathway,26-29 and activating mutations in the K-and N-RAS genes are generally found in up to 50% of
MM cases.12-17 Our study, based on the correlation of the RAS
mutation status of primary MM samples with sensitivity to
pharmacologic Akt inhibition and with the phosphorylation status
of Akt in corresponding bone marrow biopsies, again denoted the
presence of phosphorylated Akt as indicator for Akt dependency.
However, it also showed that even if RAS-mutated MM samples
tended to express phosphorylated Akt more frequently, no correlation between Akt dependency and the presence of oncogenic RAS
existed. Accordingly, knockdown of oncogenic RAS in cell lines
MM.1S and JJN-3 failed to attenuate the intrinsic phosphorylation
of Akt or of Akt substrates, such as GSK-3 or FOXO1/3a, also
indicating that the presence of oncogenic RAS is not required to
sustain endogenous Akt activity. This is in contrast to studies in
RAS wild-type ANBL-6 MM cells, where stable overexpression of
oncogenic RAS entailed increased levels of Akt phosphorylation.26
However, our results are in agreement with loss-of-function
analyses in solid tumor entities where oncogenic RAS was not
found to be a primary driver for constitutive Akt activation.39,40
Notwithstanding its statistical lack of significance, a larger number
of RAS mutant primary MM samples did also show constitutive
activation of Akt. We would therefore, not rule out that oncogenic
RAS may well support Akt activity in a subset of MM cases. It is
nowadays known that neither the preclinical efficacy nor the
clinical failure of farnesyltransferase inhibitors was attributable to
effects on oncogenic RAS,20-23 and currently no selective pharmacologic RAS inhibitors are available. Whereas extensive knowledge has been acquired on the incidence and prevalence of RAS
mutations in MM and their clinical context, functional information
on the actual relevance of oncogenic RAS in this disease is less
prevalent. Insight into RAS function has mainly been gained
through overexpression studies of either K- or N-RAS in ANBL-6
cells,24-26 but depletion of endogenous oncogenic RAS has not yet
been performed. Because the high frequency of RAS mutation
renders it a convenient genetic marker for classification of potential
therapeutic subgroups, we decided to perform an isoform-specific
loss-of-function analysis in MM cell lines to investigate whether
oncogenic RAS still maintains a role for survival in these late-stage
representations of MM. Specific K- or N-RAS knockdown did
indeed lead to strong decreases in viability if MM cells harbored
the respective oncogenic isoform, whereas little or no effects were
observed if only the wild-type isoform was present. These experiments therefore are the first to directly demonstrate that MM cells
actually display a particular dependence on oncogenic RAS for
their survival.
Our study suggests that in MM oncogenic RAS mutation and
Akt dependency are not 2 sides of the same medal: neither does
oncogenic RAS necessarily activate Akt nor does constitutive
activation of Akt depend on the presence of oncogenic RAS. This
indicates that intrinsically active RAS and Akt may delineate
distinct oncogenic pathways, which independently contribute to
MM cell survival. Such a notion is supported by our observation
that depletion of K-RAS, when combined with Akt blockade (via
knockdown of Akt1 or via pharmacologic inhibition of Akt), led to
enhanced cell death in the K-RAS mutant/Akt-dependent cell line
MM.1S but was without effect in RAS wild-type/Akt-independent
AMO-1 cells.
Oncogenic RAS is known to sustain activity of the RAS/MAPK
pathway,26,41,42 and in our hands, too, knockdown of oncogenic
RAS led to a strong decrease in the level of phosphorylated
ERK1/2 in MM.1S and JJN-3 cells. Nevertheless, although sustained blockade of this pathway with suitable concentrations of
MEK inhibitor PD184352 abrogated ERK1/2 phosphorylation, it
had little or no effect on the survival of MM cells regardless of their
RAS mutation status. To that end, we have previously shown that
knockdown of ERK1&2 did not impair survival of N-RAS mutated
INA-6 cells.31 This indicates that the prosurvival effects of
oncogenic RAS in MM are unlikely to be exclusively transmitted
via the MEK/ERK module. Pharmacologic intervention at the level
of MEK is thus not a substitute for direct RAS blockade.
Oncogenic K-RAS has recently been shown to be associated with
the presence of activated nuclear factor-B signaling in various
human carcinoma cell lines.43 However, comparison of the RAS
mutation status of the MM cell lines represented here with their
ranking for nuclear factor-B activity (nuclear factor-B transcriptional signature index) recently published by Demchenko et al,44
does not suggest a clear pattern. RAS mutant cell lines appear
equally well represented among those ranking highest (eg, MM.1
and JJN-3) or lowest (eg INA-6, NCI-H929) in the index.
In conclusion, our study shows, for the first time, that oncogenic
RAS isoforms sustain the survival of MM cells and that this effect
is unlikely to be mediated via either the Akt or the MAPK pathway.
The oncogenic RAS isoforms therefore constitute potential therapeutic targets in their own right. Although RAS is currently not
drugable, the development of strategies to block oncogenic RAS
function is warranted and highly desirable for novel treatment
approaches, which would be of immediate relevance for a welldefined patient subgroup.
Acknowledgments
This work was supported by the Deutsche Forschungsgemeinschaft
(SFB-TR17 and KFO 216) and by the MD/PhD program of the
From www.bloodjournal.org by guest on March 4, 2016. For personal use only.
2004
BLOOD, 10 FEBRUARY 2011 䡠 VOLUME 117, NUMBER 6
STEINBRUNN et al
Interdisciplinary Center for Clinical Research of the University of
Würzburg (Würzburg, Germany).
Authorship
Contribution: T. Steinbrunn designed, performed, and analyzed
experiments and wrote the paper; T. Stühmer designed and
analyzed experiments and wrote the paper; S.G., A.R., and A.M.
provided biopsies and conducted and analyzed the immunohistochemical experiments; C.U. and H.E. provided patient samples;
M.C. provided patient samples and wrote the paper; and R.C.B.
initiated and designed experiments and wrote the paper.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Torsten Steinbrunn, Medizinische Klinik und
Poliklinik II, Josef-Schneider-Straße 2, 97080 Würzburg, Germany; e-mail: steinbrunn_t@medizin.uni-wuerzburg.de.
References
1. Kyle RA, Rajkumar SV. Multiple myeloma. Blood.
2008;111(6):2962-2972.
2. Chng WJ, Glebov O, Bergsagel PL, Kuehl WM.
Genetic events in the pathogenesis of multiple
myeloma. Best Pract Res Clin Haematol. 2007;
20(4):571-596.
3. Hideshima T, Mitsiades C, Tonon G, Richardson PG,
Anderson KC. Understanding multiple myeloma
pathogenesis in the bone marrow to identify new
therapeutic targets. Nat Rev Cancer. 2007;7(8):
585-598.
4. Magrangeas F, Lodé L, Wuilleme S, Minvielle S,
Avet-Loiseau H. Genetic heterogeneity in multiple
myeloma. Leukemia. 2005;19(2):191-194.
5. Tiedemann RE, Gonzalez-Paz N, Kyle RA, et al.
Genetic aberrations and survival in plasma cell
leukemia. Leukemia. 2008;22(5):1044-1052.
6. Hsu J, Shi Y, Krajewski S, et al. The AKT kinase is
activated in multiple myeloma tumor cells. Blood.
2001;98(9):2853-2855.
7. Zöllinger A, Stühmer T, Chatterjee M, et al. Combined functional and molecular analysis of tumor
cell signaling defines 2 distinct myeloma subgroups: Akt-dependent and Akt-independent multiple myeloma. Blood. 2008;112(8):3403-3411.
8. Hyun T, Yam A, Pece S, et al. Loss of PTEN expression leading to high Akt activation in human
multiple myelomas. Blood. 2000;96(10):35603568.
9. Chang H, Qi XY, Claudio J, Zhuang L, Patterson B,
Stewart AK. Analysis of PTEN deletions and mutations in multiple myeloma. Leuk Res. 2006;30(3):
262-265.
10. Ismail SI, Mahmoud IS, Msallam MM, Sughayer MA.
Hotspot mutations of PIK3CA and AKT1 genes
are absent in multiple myeloma. Leuk Res. 2009;
34(6):824-826.
11. Müller CI, Miller CW, Hofmann WK, et al. Rare
mutations of the PIK3CA gene in malignancies of
the hematopoietic system as well as endometrium, ovary, prostate and osteosarcomas, and
discovery of a PIK3CA pseudogene. Leuk Res.
2007;31(1):27-32.
12. Chng WJ, Gonzalez-Paz N, Price-Troska T, et al.
Clinical and biological significance of RAS mutations in multiple myeloma. Leukemia. 2008;
22(12):2280-2284.
13. Rasmussen T, Kuehl M, Lodahl M, Johnsen HE,
Dahl IM. Possible roles for activating RAS mutations in the MGUS to MM transition and in the intramedullary to extramedullary transition in some
plasma cell tumors. Blood. 2005;105(1):317-323.
14. Friday BB, Adjei AA. K-ras as a target for cancer
therapy. Biochim Biophys Acta. 2005;1756(2):
127-144.
15. Portier M, Molès JP, Mazars GR, et al. p53 and
RAS gene mutations in multiple myeloma. Oncogene. 1992;7(12):2539-2543.
16. Bezieau S, Devilder MC, Avet-Loiseau H, et al.
High incidence of N and K-Ras activating mutations in multiple myeloma and primary plasma cell
leukemia at diagnosis. Hum Mutat. 2001;18(3):
212-224.
17. Liu P, Leong T, Quam L, et al. Activating mutations of N- and K-ras in multiple myeloma show
different clinical associations: analysis of the
Eastern Cooperative Oncology Group Phase III
Trial. Blood. 1996;88(7):2699-2706.
18. Corradini P, Ladetto M, Voena C, et al. Mutational
activation of N- and K-ras oncogenes in plasma
cell dyscrasias. Blood. 1993;81(10):2708-2713.
19. Neri A, Murphy JP, Cro L, et al. Ras oncogene
mutation in multiple myeloma. J Exp Med. 1989;
170(5):1715-1725.
20. Brunner TB, Hahn SM, Gupta AK, Muschel RJ,
McKenna WG, Bernhard EJ. Farnesyltransferase
inhibitors: an overview of the results of preclinical
and clinical investigations. Cancer Res. 2003;
63(18):5656-5668.
21. Harousseau JL. Farnesyltransferase inihibitors in
hematologic malignancies. Blood Rev. 2007;21(4):
173-182.
22. Karnoub AE, Weinberg RA. Ras oncogenes: split
personalities. Nat Rev Mol Cell Biol. 2008;9(7):
517-531.
23. Martinelli G, Iacobucci I, Paolini S, Ottaviani E.
Farnesyltransferase inhibition in hematologic malignancies: the clinical experience with tipifarnib.
Clin Adv Hematol Oncol. 2008;6(4):303-310.
24. Billadeau D, Liu P, Jelinek D, Shah N, LeBien TW,
Van Ness B. Activating mutations in the N- and
K-ras oncogenes differentially affect the growth
properties of the IL-6-dependent myeloma cell
line ANBL6. Cancer Res. 1997;57(11):22682275.
25. Rowley M, Liu P, Van Ness B. Heterogeneity in
therapeutic response of genetically altered myeloma cell lines to interleukin 6, dexamethasone,
doxorubicin, and melphalan. Blood. 2000;96(9):
3175-3180.
26. Hu L, Shi Y, Hsu JH, Gera J, Van Ness B,
Lichtenstein A. Downstream effectors of oncogenic ras in multiple myeloma cells. Blood. 2003;
101(8):3126-3135.
27. Shaw RJ, Cantley LC. Ras, PI(3)K and mTOR
signalling controls tumour cell growth. Nature.
2006;441(7092):424-430.
28. Young A, Lyons J, Miller AL, Phan VT, Alarcon IR,
McCormick F. Ras signaling and therapies. Adv
Cancer Res. 2009;102:1-17.
29. Khwaja A, Rodriguez-Viciana P, Wennstrom S,
Warne PH, Downward J. Matrix adhesion and
Ras transformation both activate a phosphoinositide 3-OH kinase and protein kinase B/Akt cellular
survival pathway. EMBO J. 1997;16(10):27832793.
30. Stühmer T, Arts J, Chatterjee M, et al. Preclinical
anti-myeloma activity of the novel HDAC-inhibitor
JNJ-26481585. Br J Haematol. 2010;149(4):529536.
31. Chatterjee M, Stühmer T, Herrmann P, Bommert
K, Dörken B, Bargou RC. Combined disruption of
both the MEK/ERK and the IL-6R/STAT3 pathways is required to induce apoptosis of multiple
myeloma cells in the presence of bone marrow
stromal cells. Blood. 2004;104(12):3712-3721.
32. Brummelkamp TR, Bernards R, Agami R. A system for stable expression of short interfering
RNAs in mammalian cells. Science. 2002;296
(5567):550-553.
33. Réjiba S, Wack S, Aprahamian M, Hajri A. K-ras
oncogene silencing strategy reduces tumor
growth and enhances gemcitabine chemotherapy
efficacy for pancreatic cancer treatment. Cancer
Sci. 2007;98(7):1128-1136.
34. Stühmer T, Anderson SA, Ekker M, Rubenstein JL.
Ectopic expression of the Dlx genes induces glutamic acid decarboxylase and Dlx expression. Development. 2002;129(1):245-252.
35. Stühmer T, Chatterjee M, Hildebrandt M, et al.
Nongenotoxic activation of the p53 pathway as a
therapeutic strategy for multiple myeloma. Blood.
2005;106(10):3609-3617.
36. Kuehl WM, Bergsagel PL. Multiple myeloma:
evolving genetic events and host interactions. Nat
Rev Cancer. 2002;2(3):175-187.
37. Raab MS, Podar K, Breitkreutz I, Richardson PG,
Anderson KC. Multiple myeloma. Lancet. 2009;
374(9686):324-339.
38. Podar K, Chauhan D, Anderson KC. Bone marrow microenvironment and the identification of
new targets for myeloma therapy. Leukemia.
2009;23(1):10-24.
39. Omerovic J, Hammond DE, Clague MJ, Prior IA.
Ras isoform abundance and signalling in human
cancer cell lines. Oncogene. 2008;27(19):27542762.
40. Singh A, Greninger P, Rhodes D, et al. A gene
expression signature associated with “K-Ras addiction” reveals regulators of EMT and tumor cell
survival. Cancer Cell. 2009;15(6):489-500.
41. Egan SE, Weinberg RA. The pathway to signal
achievement. Nature. 1993;365(6449):781-783.
42. Katz ME, McCormick F. Signal transduction from
multiple Ras effectors. Curr Opin Genet Dev.
1997;7(1):75-79.
43. Barbie DA, Tamayo P, Boehm JS, et al. Systematic RNA interference reveals that oncogenic
KRAS-driven cancers require TBK1. Nature.
2009;462(7269):108-112.
44. Demchenko YN, Glebov OK, Zingone A, Keats JJ,
Bergsagel PL, Kuehl WM. Classical and/or alternative NF-kappaB pathway activation in multiple
myeloma. Blood. 2010;115(17):3541-3552.
From www.bloodjournal.org by guest on March 4, 2016. For personal use only.
2011 117: 1998-2004
doi:10.1182/blood-2010-05-284422 originally published
online December 13, 2010
Mutated RAS and constitutively activated Akt delineate distinct
oncogenic pathways, which independently contribute to multiple
myeloma cell survival
Torsten Steinbrunn, Thorsten Stühmer, Stefan Gattenlöhner, Andreas Rosenwald, Anja Mottok,
Christian Unzicker, Hermann Einsele, Manik Chatterjee and Ralf C. Bargou
Updated information and services can be found at:
http://www.bloodjournal.org/content/117/6/1998.full.html
Articles on similar topics can be found in the following Blood collections
Lymphoid Neoplasia (2218 articles)
Multiple Myeloma (307 articles)
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society
of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.