Examining the trends in costs of
medicines for drug-susceptible and
drug-resistant tuberculosis from 2010 –
2013; an analysis of Global Fund PQR
data
By: Ambrose Agweyu, Frank Wafula, Brian Mwangi, Cleopatra
Mugyenyi, Kate Macintyre and Bernard Langat
14 January 2015
P.O. Box 66869–00800, Nairobi, Kenya
TEL
+254 (0) 774 135 984 EMAIL info@aidspan.org
www.aidspan.org
Table of Contents
ABBREVIATIONS ................................................................................................................................... 3
PREFACE ............................................................................................................................................... 3
LIST OF TABLES .................................................................................................................................... 4
LIST OF FIGURES .................................................................................................................................. 4
EXECUTIVE SUMMARY ........................................................................................................................ 5
BACKGROUND ...................................................................................................................................... 6
METHODOLOGY .................................................................................................................................... 6
RESULTS ................................................................................................................................................ 8
Costs of TB medicines (High burden countries vs other countries) ..................................................................... 8
Analysis of trends ..................................................................................................................................................................... 11
DISCUSSION ........................................................................................................................................ 18
CONCLUSION ...................................................................................................................................... 20
REFERENCES ...................................................................................................................................... 21
APPENDIX 1: BOX PLOTS SHOWING EXTREME VALUES EXCLUDED FROM ANALYSES OF
TRENDS................................................................................................................................................ 22
APPENDIX 2: ANTI-TB MEDICINE ENTRIES IN PQR DATABASE (JANUARY 2010 – DECEMBER
2013) ..................................................................................................................................................... 25
Copyright © January 2015 by Aidspan. All rights reserved.
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 2
Abbreviations
FDC
GDF
GF
HBC
LBC
NTP
PAS
PQR
RHZ
RHZE
TB
WHO
Fixed Dose Combination
Global Drug Facility
Global Fund
High burden countries
Low burden countries
National Tuberculosis Program
Para-Aminosalicylate
Price and Quality Reporting
Rifampicin, Isoniazid, Pyrazinamide
Rifampicin, Isoniazid, Pyrazinamide, Ethambutol
Tuberculosis
World Health Organization
Preface
Aidspan (www.aidspan.org) is an international non profit organization based in Kenya,
whose mission is to reinforce the effectiveness of the Global Fund. Aidspan performs this
mission by serving as an independent observer of the Fund and by providing services that can
benefit all countries wishing to obtain and make effective use of Global Fund financing.
This paper is one of several Aidspan research reports available at
www.aidspan.org/page/research. Reports published over the past year by Aidspan include:
The New Funding Model Allocations: An Aidspan Analysis (November 2014)
Expenditure reported by national Tuberculosis programs in 22 high-burden countries
between 2010 – 2012: what is the Global Fund’s contribution? (Oct 2014)
Options for reforming the Global Fund Board (April 2014)
Conflict of Interest in Country Coordination Mechanisms: An Aidspan Survey (May
2014)
Procurement Cost Trends for Global Fund Commodities: Analysis of Trends for
Selected Commodities 2005–2012 (April 2013)
Global Fund Principal Recipient Survey: An Assessment of Opinions and Experiences
of Principal Recipients (April 2013)
Aidspan also publishes news, analysis and commentary articles about the Global Fund in its
Global Fund Observer (GFO)newsletter and on GFO Live. To receive GFO Newsletter, send
an email to receive-gfo-newsletter@aidspan.org.
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 3
Aidspan finances its work primarily through grants from governments and foundations.
Aidspan does not accept funding of any kind from the Global Fund. Aidspan and the Global
Fund maintain a positive working relationship, but have no formal connection. Aidspan does
not allow its strategic, programmatic or editorial decision-making to be influenced by the
Global Fund or by relationships with Aidspan’s funders.
Acknowledgements
Aidspan thanks the following donors whoall contributed to supporting Aidspan in 2014, and
thus supporting the production of this paper: the UK Department for International
Development (DFID), the Ford Foundation, GIZ Backup Initiative, Irish Aid, the
Government of the Netherlands, NORAD and Hivos.
List of Tables
Table 1: Commodities included in the analysis ......................................................................... 7
Table 2: Comparison of Median Unit Costs of Selected Anti-TB Medications Purchased by
High and Low Burden Countries ............................................................................................. 10
List of Figures
Figure 1: Trends in Costs of Adult RHZE FDC from 2010 to 2013 (High versus Low Burden
Countries)................................................................................................................................. 11
Figure 2: Trends in Costs of Adult TB Cat I+III Patient Kit A from 2010 to 2013 (High
versus Low Burden Countries) ................................................................................................ 12
Figure 3: Trends in Costs of Pediatric RHZ from 2010 to 2013 (High versus Low Burden
Countries)................................................................................................................................. 13
Figure 4: Trends in Costs of Adult RHZE versus Pediatric RHZ from 2010 to 2013 ............. 14
Figure 5: Trends in Costs of Capreomycin from 2010 to 2013 (High versus Low Burden
Countries)................................................................................................................................. 15
Figure 6: Trends in Costs of Cycloserine from 2010 to 2013 (High versus Low Burden
Countries)................................................................................................................................. 16
Figure 7: Trends in Costs of Levofloxacin from 2010 to 2013 (High versus Low Burden
Countries)................................................................................................................................. 17
Figure 8: Trends in Costs of PAS Sodium from 2010 to 2013 (High versus Low Burden
Countries)................................................................................................................................. 18
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 4
Executive Summary
Tuberculosis (TB) is a major public health challenge affecting up to one third of the world’s
population. Despite the availability of effective treatments, TB continues to claim 1.5 million
lives annually. Substantial reductions in incidence and mortality can be achieved through
improved access to effective anti-TB medications. This strategy is heavily supported by the
Global Fund against AIDS, Tuberculosis and Malaria (GF) through grants disbursed to national
TB programs, which are estimated to support up to three quarters of funding for programs in
high burden countries. This report describes the trends in costs for selected TB medications
purchased through grants from the GF from 2010 – 2013 in the 22 high burden countries (HBC)
and low burden countries (LBC).
The median cost of all first line anti-TB medications was significantly lower in HBC compared
to LBC with pediatric formulations costing approximately half the value of adult alternatives. In
contrast, the costs of second line treatments showed no variation across high and low burden
countries. Further, the unit costs of second line treatments were up to 100 times higher than those
of first line formulations. A rising trend was observed for first line treatments over the four year
period while the costs of second line treatments, with the exception of capreomycin, reduced
over time.
Trends in the costs of second line treatments and first line treatments in low burden countries
may be attributed to the role of the Global Drug Facility (GDF) in obtaining competitive prices
through pooled procurement. Conversely, the costs of first line treatments in high burden
countries show characteristics of a mature market. Differences in costs for pediatric and adult
first line medications coincide with the disbursement of grants by UNITAID to subsidize the cost
of pediatric anti-TB drugs. This analysis illustrates important differences in costs of anti-TB
medications and highlights potential areas of intervention for initiatives aimed at accelerating
progress towards achieving global TB targets through increasing access to affordable anti-TB
medications.
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 5
Background
Tuberculosis continues to rank among the leading causes of death accounting for an estimated 9
million new annual infections and 1.5 million deaths globally (1). Along with HIV and malaria,
tuberculosis was acknowledged as a global public health challenge by world leaders in the
Millennium Declaration and articulated under Millennium Development Goal 6 (2). Efforts
towards achieving this goal have been rewarded with variable degrees of success with 8 out of 22
of the high burden countries (HBC) 1 having met all of the 2015 targets for reductions in TB
cases and deaths and a further two on track to do so (1). However, the average global decline in
TB incidence between 2000 and 2013 remains modest at 1.5% per year.
Increasing access to effective anti-TB medicines is a major strategy in the effort to reduce the
burden of TB. Although financing for anti-TB medicines from both domestic sources has
increased steadily over recent years, donor funding remains a major source of funding for antiTB medicines, accounting for up to 70% of the national tuberculosis program (NTP) budgets in
some high burden countries (3). In a recent report describing the expenditure of national TB
programs (NTPs) of the 22 HBC between 2010 – 2012, the Global Fund against AIDS,
Tuberculosis and Malaria (GFATM) was reported to have contributed up to 76% of total national
expenditure of the programs of the countries studied (4). Despite its central role in financing TB
care, literature on the trends in costs for anti-TB medicines purchased through the Global Fund is
surprisingly scarce.
Methodology
We sought to describe the trends in procurement cost for selected TB commodities using
information collected through the Global Fund’s Price Quality Reporting (PQR) system from
2010-2013. The PQR is a Global Fund provided online reporting facility that tracks commodity
prices as reported by countries as they buy commodities using their grant money. We
1
The 22 countries that accounted for approximately 80% of all estimated cases of TB worldwide based on WHO
statistics. Listed alphabetically: Afghanistan, Bangladesh, Brazil, Cambodia, China, DR Congo, Ethiopia, India,
Indonesia, Kenya, Mozambique, Myanmar, Nigeria, Pakistan, Philippines, Russian Federation, South Africa,
Thailand, Tanzania, Uganda, Viet Nam, Zimbabwe. (Global Tuberculosis Control: WHO Report
2000. WHO/CDS/TB/2000.275 (World Health Organization, Geneva, 2000), p. 10.)
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 6
specifically sought to analyze the trends of first line and second line TB medicines procured by
both the 22 high burden and all other countries that received grants from the Global Fund
between 2010 and 2013.
Data from the PQR were obtained from the Global Fund, and inspected for among other things,
completeness, presence of outliers and distribution. Extreme values (after inspection) were
assumed to be data entry errors, and were excluded from the analyses of trends. Details of the
outliers excluded are provided in Appendix 1.The scope of the analysis was defined a priori by
restricting the comparisons to those of the costs reported for first line anti-TB fixed dose
combinations (adult and pediatric) and frequently purchased single medications for drug resistant
TB in high burden and low burden countries (table 1). The complete list of anti-TB medications
contained in the database is provided in Appendix 2.
Table 1: Commodities included in the analysis
Commodity
Number of entries in PQR database
High burden countries
Other countries
Total
82
143
225
31
22
53
22
40
62
Cycloserine
103
285
388
Levofloxacin
113
277
390
Capreomycin
53
165
218
PAS Sodium
66
212
278
First line
Adult RHZE1 FDC2
TB Cat. I+III Patient Kit A
Pediatric RHZ4 FDC
3
Second line
1
RHZE - Rifampicin 150mg + Isoniazid 75mg + Pyrazinamide 400mg + Ethambutol 275mg
FDC – Fixed Dose Combination
3
Four-drug FDC 6x28tabs (R 150mg / H 75mg / Z 400mg / E 275mg) plus Two-drug FDC 12x28tabs (R 150mg / H
75mg)
4
Pediatric RHZ - Rifampicin 60mg + Isoniazid 30mg+ Pyrazinamide 150mg
2
Unit costs were derived from the quantities of medications purchased and total costs paid for
respective items purchased. Median costs for the selected medicines procured from 2010 to 2013
were calculated with interquartile ranges. Comparisons between high burden countries and other
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 7
countries were made using the Mann-Whitney U test and corresponding p-values reported.
Trends over the period of interest were illustrated using scatter plots. Unit costs were regressed
against time and represented as lines of best fit superimposed on the scatter plots. We conducted
hypothesis tests to compare the regression coefficients of costs for the selected commodities in
high and low burden countries. All analyses were conducted using STATA version 13 (Stata
Corp, Texas, USA).
Results
At the time of analysis, the PQR database contained 27,748 entries from 128 countries. Of these,
5,280 (19.0%) were categorized as TB-related medications. All high burden countries were
represented, with the exception of South Africa and Brazil, both of whom did not procure TB
medicines through the Fund’s facility during the period covered in the analysis.
Costs of TB medicines (High burden countries vs other countries)
Table 2 summarizes a comparison of costs for selected first and second line TB medicines
procured through the Global Fund from between 2010 and December 2013.
Median costs for RHZE, the first line adult fixed dose combination (FDC) showed minimal
variation ranging from USD .05 to .06 per tablet. A comparison of overall costs between high
and low burden countries revealed significantly lower median costs in the former category
(P.001). Similar differences were observed for TB Category I+III Patient Kit A (a kit combining
first line medicines for the intensive and continuation phases of treatment - see table 1). The
median cost for the other first line treatment analyzed - pediatric RHZ FDC was also lower
within the high burden countries, although the association was relatively weaker (P=.07).
In contrast, there was no relationship between costs and disease burden for the four second line
treatments included in this analysis. With the exception of levofloxacin (a broad spectrum
antibiotic), costs of second line treatments were substantially higher than first line treatments.
The cost of Capreomycin, a second line anti-TB, was nearly 100 times higher than that for the
adult four-drug FDC.
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 8
Notable variations were observed in the costs reported for pediatric RHZ FDC and capreomycin
(IQR .03 to .07 and 4.3 to 8.0 respectively). In comparison, the costs of treatments within high
burden countries showed only minimal variation, reflected by narrow interquartile ranges of
median unit costs.
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 9
Table 2: Comparison of Median Unit Costs of Selected Anti-TB Medications Purchased by High and Low Burden Countries
Category
First line medications
Adult RHZE
TB Cat. I+III
Pediatric
FDC
Patient Kit A
RHZ FDC
.06 (83)*
18.2 (31)
.03 (22)
High burden
(.05 – .06)**
(17.1 – 20.2)
(.03 – .03)
countries
.06 (149)
20.2 (22)
.04 (41)
Other
(.06 – .06)
(19.1 – 20.2)
(.03 – .07)
countries
.001
.05
.07
P value†
* Total number of entries
** Interquartile range
Second line medications
Capreomycin
Cycloserine
Levofloxacin
PAS Sodium
5.5 (53)
(4.3 – 5.7)
5.5 (165)
(4.3 – 8.0)
.55
.06(117)
(.05– .07)
.06 (278)
(.05– .06)
.67
.39 (79)
(.38 – .43)
.38 (253)
(.38 – .41)
.30
.59 (105)
(.59 – .59 )
.59 (293)
(.59 – .59)
.90
†Mann-Whitney U test
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 10
Analysis of trends
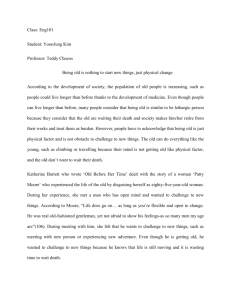
First line Adult RHZE FDC
Significant ascending linear trends were observed for the cost of first line adult RHZE FDC
from 2010 to 2013 in both HBC (P<.001) and other countries (P<.001). The change in price
over time did not vary between the two groups (P=.53) (figure 1).
Figure 1: Trends in Costs of Adult RHZE FDC from 2010 to 2013 (High versus Low Burden
Countries)
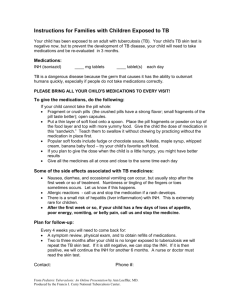
First line TB Cat. I+II Patient Kit A
Although the number of entries for the adult TB Category I+II Patient Kit A was
considerably lower than that recorded for the RHZE FDC, a similar trend of progressively
rising costs was observed for purchases in both HBC and other countries (P< .001 in both
groups) (figure 2). The change in price over time also did not vary between the two groups
for this commodity.
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 11
Figure 2: Trends in Costs of Adult TB Cat I+III Patient Kit A from 2010 to 2013 (High versus
Low Burden Countries)
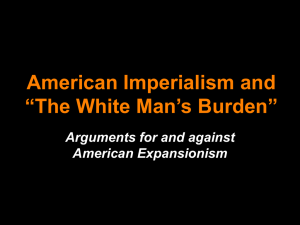
First line Pediatric RHZ FDC
The costs of the pediatric RHZ FDC increased over time in both high and low burden
countries. This trend, although statistically significant (P=.03 and P=.02 for high and low
burden countries respectively), was less pronounced than that observed for costs of other first
line medications (figures 2 and 3). The change in costs over time in HBC versus other
countries was almost identical (P=.91) (figure 3).
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 12
Figure 3: Trends in Costs of Pediatric RHZ from 2010 to 2013 (High versus Low Burden
Countries)
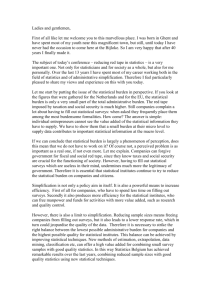
Pediatric versus Adult First line FDCs
A comparison between pediatric and adult first line FDCs similarly revealed a rising trend in
costs over time. Although the average costs of both the adult medications was noticeably
higher than the pediatric alternative, the increase in price over time was very similar between
the two groups (P=.54) (figure 4).
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 13
Figure 4: Trends in Costs of Adult RHZE versus Pediatric RHZ from 2010 to 2013
Second line medications: Capreomycin
Costs of capreomycin increased in both high and low burden countries over time. Although
statistically significant upward linear trend was observed (P=.01 and <.001 for high and low
burden countries respectively), a sudden rise in the cost of individual purchases was apparent
in 2011 with a reduction in subsequent years (figure 5).
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 14
Figure 5: Trends in Costs of Capreomycin from 2010 to 2013 (High versus Low Burden
Countries)
Second line medications: Cycloserine
The cost of cycloserine reduced steadily over the four year period in both high and low
burden countries (P<.001). Although the direction of change in cost was consistent in the two
groups, the rate of decline appeared to be more pronounced in low burden countries (P=.05)
(figure 6).
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 15
Figure 6: Trends in Costs of Cycloserine from 2010 to 2013 (High versus Low Burden
Countries)
Second line medications: Levofloxacin
A significant decline in the cost of levofloxacin was observed within HBC over the four years
(P=.002). Within low burden countries the cost of levofloxacin remained unchanged over
time (P=.36). This difference in trend between the two groups of countries was statistically
significant (P=.02) (figure 7).
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 16
Figure 7: Trends in Costs of Levofloxacin from 2010 to 2013 (High versus Low Burden
Countries)
Second line medications: PAS Sodium
Consistent with trends in costs of other second line anti-TB medications, the costs of PAS
Sodium also showed substantial reductions over time (P<0.01 in both the high burden and the
other countries). A comparison of the fitted trends revealed that the difference in the rate of
decline did not vary significantly between the two categories of countries (P=.18) (figure 8).
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 17
Figure 8: Trends in Costs of PAS Sodium from 2010 to 2013 (High versus Low Burden
Countries)
Discussion
We used price information reported through the Global Fund’s PQR system to study trends in
costs of TB medicines between January 2010 and December 2013. We believe this is the first
time such an analysis has been done. Previous analyses have looked at the trends for HIV and
malaria commodities (5, 6).
The Global Drug Facility (GDF), a section under the WHO-supported STOP TB initiative (7)
has contributed significantly towards ensuring access to high quality affordable anti-TB
medicines since its inception in 2001 (8). This facility, which functions through pooled
procurement of competitively sourced commodities, aims to ensure uniform costs across
countries for supported commodities which include first and second line anti-TB medications
(including pediatric drugs). This analysis reveals important differences between costs across
commodities purchased in the 22 high burden countries and low burden countries. Our
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 18
findings suggest the existence of external channels of procurement not supported by the
GDF. Indeed a recently published report estimated that the GDF supplied first line treatments
for only a third of reported TB cases in 2011 (9). This same report states that the market share
of GDF-supplied first line treatments has been shrinking over time while that for second line
treatments appears to be growing. This trend may be attributed to a vibrant market for first
line anti-TB medications purchased directly from suppliers at competitive costs – a situation
that supports the continued need for rigorous quality assurance mechanisms such as the WHO
prequalification system for suppliers. The GDF however maintains an important role in the
procurement of second line TB medicines with a limited number of manufacturers and for
first line medicines in low burden countries.
The treatment of drug resistant tuberculosis is a growing global challenge. This analysis
revealed an encouraging general downward trend in the costs of medications for drug
resistant tuberculosis. This finding is consistent with the 2013 annual report of the Stop TB
Partnership which attributes the declining cost to the GDF (10). In spite of the declining costs
of second line treatments, the cost of treating multi-drug resistant TB remains over 100 times
that of treating drug sensitive tuberculosis (11). A significant proportion of this amount is
spent on injectable medications. The analysis showed, for instance, that the cost of
capreomycin increased over the period of analysis. This rise was attributed to a global
shortage in 2011 that followed an acute shortage of the active pharmaceutical ingredient from
the sole quality assured manufacturer (12). High costs of this and other second line drug
illustrate the immediate need for expansion of the pool of quality assured manufacturers for
second line treatments which currently consumes a disproportionate amount of national
budgets for TB and threatens to reverse the gains made in lowering the burden of drug
susceptible TB over recent years. The relatively low cost of levofloxacin, a second line
fluoroquinolone, is reflective of its availability from at least three suppliers (13), and use
beyond TB treatment as a broad spectrum antibiotic with several other clinical indications.
Average costs of adult first line anti-TB medications showed a steady increase over time.
This trend may be reflective of a mature market in the face of global economic crisis. The
sizable mature nature of the market for this group of drugs has been previously
acknowledged in a report published by UNITAID in 2012 (14).
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 19
Global estimates indicate that childhood TB accounts for 6 - 21% of all cases (1, 15).
Through grants from UNITAID, the costs of anti-TB medications for this population are
reported to have reduced by up to 30% (16). Our analysis showed a lower overall cost of first
line medications for children compared to adult FDCs despite reports of high production
costs and low demand from national programs (14). However, we observed no difference in
the trends in costs over time for the two groups of medications.
Strength of our study was the application of statistical techniques to compare groups and
analyze trends that allowed for objective comparisons to be made. We were therefore able to
examine small variations in costs that would otherwise be difficult to detect by visual
inspection but may have significant implications for commodities costing millions of dollars.
One limitation in our study was that our analysis could not account for different
manufacturers of the commodities analyzed as these data are not currently collected in the
PQR database. Other analyses of PQR data have shown variations in the packaging quantities
of TB medicines across manufacturers (13). In an attempt to account for such differences we
considered individual tablets (except for TB Cat. I+III Patient Kit A) as our units of analysis.
We propose the inclusion of details of manufacturers in the PQR system to facilitate
comparison of costs and further enhance the transparency of procurement for commodities
purchased through grants from the Fund.
Conclusion
This analysis provides important insights to the variation in costs of a range of TB treatments.
The results may be used to evaluate ongoing initiatives to increase access to anti-TB
medications and highlight priority areas for intervention. Notable differences were observed
in trends of first and second line TB medications. While costs of second line medications
have shown a decline over time, average prices remain several times higher than those of first
line treatments. The Global Fund through initiatives such as the GDF are expected to
continue to play an important role in ensuring access to affordable quality anti-TB medicines.
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 20
References
1.
World Health Organization. Global tuberculosis report 2014. Geneva: World Health
Organization, 2014.
2.
UN General Assembly (55th sess. : 2000-2001). United Nations Millennium Declaration,
Resolution Adopted by the General Assembly. New York: United Nations, 2000.
3.
Floyd K, Fitzpatrick C, Pantoja A, Raviglione M. Domestic and donor financing for
tuberculosis care and control in low-income and middle-income countries: an analysis of trends,
2002-11, and requirements to meet 2015 targets. The Lancet Global health. 2013;1(2):e105-15.
4.
Macintyre K, Mwangi B. Expenditure reported by national Tuberculosis programs in 22 high
burden countries between 2010 – 2012: what is the Global Fund’s contribution? Nairobi, Kenya:
AIDSPAN, 2014.
5.
Wafula F, Agweyu A, Macintyre K. Regional and temporal trends in malaria commodity
costs: an analysis of Global Fund data for 79 countries. Malar J. 2013;12:466.
6.
Wafula F, Agweyu A, Macintyre K. Trends in procurement costs for HIV commodities: a 7year retrospective analysis of global fund data across 125 countries. J Acquir Immune Defic Syndr.
2013;65(4):e134-9.
7.
Stop TB Partnership. The Global Plan to Stop TB 2011–2015: Transforming the fight towards
elimination of tuberculosis. Geneva: World Health Organization, 2010.
8.
Matiru R, Ryan T. The Global Drug Facility: a unique, holistic and pioneering approach to
drug procurement and management. Bulletin of the World Health Organization. 2007;85(5):348-53.
9.
Arinaminpathy N, Cordier-Lassalle T, Vijay A, Dye C. The Global Drug Facility and its role
in the market for tuberculosis drugs. Lancet. 2013;382(9901):1373-9.
10.
World Health Organization (WHO). Stop TB Partnership – Annual Report 2013. Geneva:
World Health Organization, 2013.
11.
Pooran A, Pieterson E, Davids M, Theron G, Dheda K. What is the cost of diagnosis and
management of drug resistant tuberculosis in South Africa? PLoS One. 2013;8(1):e54587.
12.
Grania Brigden. Capreomycin shortage – symptom of a bigger problem in multidrug-resistant
tuberculosis London: BMJ Publishing Group; 2011 [cited 2014 20th October]. Available from:
blogs.bmj.com/bmj/2011/07/21/grania-brigden-capreomycin-shortage-symptom-of-a-bigger-problemin-multidrug-resistant-tuberculosis/.
13.
Lisa Smith and Prashant Yadav. Analysis of the Global Fund Financed Market for TB
medicines: Competitive landscape, market shares, product volumes and product variety
Michigan2014 [cited 2014 20th October]. Available from:
http://wdi.umich.edu/research/healthcare/resources/GF_PQR_TB_Mrkt_Analysis%20Jan14_Update.p
df.
14.
UNITAID. HIV, Tuberculosis and Malaria Medicines Landscape: Progress Report on
Emerging Issues and Potential Opportunities to Improve Access. Geneva: World Health Organization,
2012.
15.
Dodd PJ, Gardiner E, Coghlan R, Seddon JA. Burden of childhood tuberculosis in 22 highburden countries: a mathematical modelling study. The Lancet Global health. 2014;2(8):e453-9.
16.
World Health Organization (WHO). UNITAID - Innovative financing to shape markets for
HIV/AIDS, malaria and tuberculosis: World Health Organization (WHO); 2014 [cited 2014 20th
October]. Available from: http://www.unitaid.eu/en/children-tb-treatment.
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 21
Appendix 1: Box Plots Showing Extreme Values Excluded from
Analyses of Trends
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 22
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 23
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 24
Appendix 2: Anti-TB Medicine Entries in PQR Database (January
2010 – December 2013)
Product Name
Amikacin
Amoxicillin
Amoxicillin+Clavulanate - FDC
Capreomycin
Clarithromycin
Clofazimine
Cycloserine
Ethambutol
Ethambutol+Isoniazid - FDC
Ethambutol+Isoniazid+Pyrazinamide+Rifampicin - FDC
Ethambutol+Isoniazid+Rifampicin - FDC
Ethionamide
Isoniazid
Isoniazid+Pyrazinamide+Rifampicin - FDC
Isoniazid+Rifampicin - FDC
Kanamycin
Levofloxacin
Linezolide
Moxifloxacin
Ofloxacin
PAS Sodium
Prothionamide
Pyrazinamide
Rifampicin
Streptomycin
TB Cat. I+III Patient Kit A
TB Cat. I+III Patient Kit B
TB Cat. I+III Patient Kit C
TB Cat. I+III Patient Kit C UNICEF (DPRK)
TB Cat. II Patient Kit A1
TB Cat. II Patient Kit A2
TB Cat. II Patient Kit B1 UNICEF (DPRK)
TB Cat. II Patient Kit B1 UNICEF (DPRK)
TB Cat. II Patient Kit B2
TB Cat. II Patient Kit C
TB India PC1 Cat-I Patient Kit
TB India PC10
TB India PC13 Ped PWBs 6-10kg
TB India PC14 Ped PWBs 11-17 kg
TB India PC15 Ped PPs 18-25 kg
TB India PC16 Ped PPs 18-25kg and 26-30kg
TB India PC2 Cat-II Patient Kit
TB India PC3
TB India PC4
TB India PC5
Terizidone
Water for injection
Total
Number of purchases
104
1
111
299
22
17
507
223
24
300
133
281
141
68
352
217
462
4
180
113
433
199
399
14
227
68
2
5
8
5
18
4
1
3
1
64
3
13
20
12
11
58
17
20
1
4
111
5,280
_________________________________________________________________________________
An analysis of Global Fund PQR data
An Aidspan Publication
14 Jan 2015
Page 25