Joint Strategic Needs Assessment
advertisement

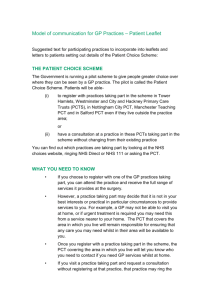
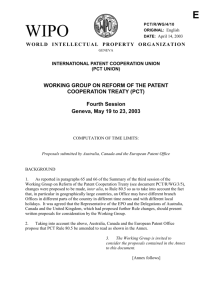
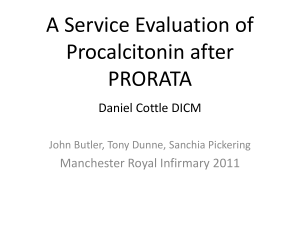
PUBLIC HEALTH Walsall Joint Strategic Needs Assessment: Briefing Paper Public Health Report No: PH0004-SL0802 Author: Dr Sue Laverty and Rachel Robinson Issued: 1st February 2006 Public Health Directorate Walsall Teaching Primary Care Trust Jubilee House Bloxwich Lane Walsall WS2 7JL Telephone: 01922 618388 Facsimile: 01922 618360 www.walsall.nhs.uk 1 Walsall Joint Strategic Needs Assessment Briefing Paper 1. Purpose This briefing paper discusses the new duty conferred on local authorities and PCTs to develop Joint Strategic Needs Assessments (JSNA), the implications for commissioning and service planning in Walsall and suggests how this important area of work may be progressed locally. It has been produced for the Director of Public Health, Director of Social Care and Inclusion, Associate Director for Adults Services and the Director of Children’s Services. 2. Background The Local Public Involvement in Health Act (October 2007) signals a new direction for local government. In the context of developing further effective, accountable local government it seeks to: Strengthen strategic leadership and partnership approaches Empower local citizens and communities Focus commissioning on outcomes Simplify the performance framework and move to a light touch approach in terms of inspection At the same time the NHS is in the midst of significant reform. There is a synergy between the approach outlined above and the NHS systems reform agenda. JSNA is seen as a crucial part of this agenda. There is increasing recognition that commissioning has focused on volume and price, rather than outcomes. There is an over emphasis on providing care in institutional and acute settings. Our focus has been on treating illness rather than preventing them and progress in tackling health inequalities has been slow. Whilst, the challenge of providing choice, placing patients at the centre and importantly giving them a real say in service development remains. Proposed in a Commissioning Framework for Health and Well-being (2007) and Creating Strong, Safe and Prosperous Communities (2007), the JSNA is seen as an important tool in addressing some of these issues. 2. What is a JSNA? A JSNA aims to inform commissioning strategies designed to improve health and wellbeing and reduce inequalities. It should inform health and social service planning decisions and delivery of priorities through the Local Area Agreement, in both the medium and longer term. In addition the JSNA should be used to inform and link to a range of other plans and strategies including, Sustainable Community Strategy, PCT local delivery plans, PBC business plans, Children and Young People’s plan to name but a few. JSNA is a continuous process underpinned by three key principles: Partnership working Community engagement Evidence of effectiveness It is a core element in the commissioning cycle (see diagram 1) and it is envisaged that a range of outputs might derive from this process (see diagram 2). The findings from the assessment will need to be shared with a range of stakeholders in order to inform commissioning decision across the health and local authority sector. 2 Diagram 1: The commissioning cycle Needs Priorities Review Outcomes (what are the gaps and how do we fill the gaps) Deliver plan Decide action Get resources This part of the cycle is where the outcomes are measured Diagram 2: JSNA 3 3. Why do a JSNA? Undertaking a JSNA is a statutory requirement but the real value of the JSNA process is in providing a framework for enhanced partnership working and community involvement around the commissioning agenda. JSNAs provide the opportunity to look ahead 3-15 years and support and direct change so that local services: Are shaped by the views of local people Reduce health inequalities Increase social inclusion Are delivered effectively and efficiently. A good JSNA will: Define achievable improvements in health and social care outcomes for local people Inform commissioning cycles Aid better decision making Underpin the Local Area Agreement and the PCT’s prospectus Send signals to existing and potential providers of services about potential service change 4. Implementing JSNA in Walsall Whilst health needs assessment are not new the JSNA offers the opportunity to systematise our approach and undertake assessments jointly across health and local government sectors. This approach does raise important issues which are now discussed in turn 4.1 JSNA – local vision Considerable latitude has been given to how localities define and utilise JSNAs. JSNA is not an end in itself. The value of this approach depends on local agreement re its value and the role it will play in informing local commissioning cycles across the health economy. There needs to be local ownership and agreement about what success looks like. How will we know if JSNA has been worthwhile? How close are we in Walsall to agreeing this vision and the criterion for success? What do we need to do next to achieve it? (see section 4) 4.2 Refining the question There is no dearth of data to collate nor of information to present and herein lies a danger. Whilst it might seem appealing to want to collect data on every conceivable determinant of health and wellbeing, the reality is that without focus a needs assessment can easily loose its way. Data collation becomes an end in itself. It is more useful for a needs assessment to be question-led and allow this to refine your approach. What are the specific questions that commissioners want answers to? How prepared are they to act on a plausible range of answers? What is their commitment? Focusing the line of enquiry is more likely to result in an effective JSNA which informs change. To this end implementing JSNA locally will require engaging with key commissioning and planning groups across the health and partnership sector. Initial discussions regarding the focus of JSNA in Walsall have suggested that tackling health inequalities offers a good option. Given that it has been prioritised in Walsall tPCT’s strategy and a prime focus of Walsall MBC as a spearhead authority. Focusing the JSNA on this issue would tie in with the development of a local Health Inequalities Strategy and also build on existing needs assessments filling any gaps from an inequalities perspective. 4 4.3 Data collation It is clear that a good JSNA relies on sound data. A national minimum core dataset is being developed, which takes into account the DOH’s key outcomes and the Local Government National Indicator set. There is an expectation that locally relevant data sets will be added. See appendix 1 for the dataset as it currently stands with comments about availability and collation of the information across Walsall. In addition, work has begun in Walsall assembling other relevant documents and data. Agreeing, populating and maintaining this dataset poses challenges and begs the question of whether Walsall has the infrastructure, in terms of information databases, analyst’s ands resources to support this work and the additional work proposed locally. Currently, both within and between organisations different information systems and teams collect information and produce intelligence derived from the data. These systems are not necessarily compatible and interpretation of the data requires a good working knowledge and experience of the organisation/sector. There are resource implications for implementing this process which need to be considered. In terms of capacity analyst support will be required for the collation, verification and interpretation of the data. This may require a dedicated officer/team across organisations to co-ordinate the work. An attempt was made to develop a pooled intelligence resource across Walsall. The Shared Partnership Information Resource (SPIR) had a vision to be pro-active, action driven by shared strategies and pooled intelligence resource. The resource was to inform local decision making and the development of strategies to reflect common objectives. A data warehouse was developed and hosted at Black Country Observatory (BCO) containing shared socioeconomic information. Whilst the features and the benefits of the SPIR were recognised across the Borough sustaining the system proved difficult for a number of reasons. The JSNA may provide an opportunity to revisit this principle. 5. Next steps in Walsall It has been shown that JSNAs will allow us to build on existing expertise and knowledge in needs analysis and further strengthen partnership approaches locally. The change required to deliver effective JSNAs is in degree rather than kind. It will require: Agreeing a vision for JSNA, defining criterion for success and ensuring ownership across the partnership Stronger partnership working across the commissioning agenda and rationalisation of the process and structures which support it Shared data collation and analysis and consideration of the infrastructure required to ensure timely delivery An explicit reporting pathway, a clearly identifiable line of accountability and performance monitoring framework A suggested way forward is to: Agree an overall steering group comprising the Directors of Public Health, Adults Social Services, Director of Children’s services and the Director of Walsall Borough Strategic partnership. Establish a working group to address the key issues outlined above with initial priorities to include, agreeing a vision and local ownership of JSNA, developing the minimum data set and framework for collation and completing an initial draft by October 2008. It has to be acknowledged that this is an interitive process which will be refined over the next 12-14 months. 5 Appendix 1 – Data Required for JSNA Local Availability v7a Domain Table 1: PRIMARY DATA NEEDED FOR A STRATEGIC NEEDS ASSESSMENT Sub-domain Population numbers Sub-subdomain Data/Indicator Available Source Estimates 5 year age bands and gender Y ONS Projections Population 3-5 years ahead Y ONS Current Current births Y ONS or PCT Lead Agency/ Officer LA or PCT LA or PCT PCT Frequency Reported Lowest Geography Covered Annual Borough Annual Borough Quarterly Postcode Demography Births Projections Projected births Y PCT PCT Annual Borough Estimates Numbers and percentages by age band Y ONS LA or PCT Annual Borough Projections 3-5 years ahead N Limiting Long-Term Illness Y ONS, Census Y ONS Y Y Ethnicity Disability Social & Environmental Context Migration Misc proxy indicators Deprivation Living arrangements Housing Bold red = National Indicators Italic grey = optional indicators See www.auditcommission.gov.uk/migrantworkers/d ata for available indicators Index of Multiple Deprivation (IMD) Proportion of children in poverty (NI 116) 1. Housing tenure 2. Overcrowding Older People 1. Living alone 2. Central heating LA or PCT Borough LA or PCT Every 10 yrs SOA ODPM LA or PCT Every 3 years SOA ONS, Census LA or PCT Every 10 yrs SOA Comments Not currently available but could be estimated from historic data and local intelligence A joint working group led by Tim Ferguson, could look at developing/scrutinising local demographic estimates and projections More detailed description of data is available Work in progress. Indicators are liable to be added, removed or amended. Appendix 1 – Data Required for JSNA Local Availability Domain v7a Sub-domain Sub-subdomain Data/Indicator Available Source Adults with learning disabilities in settled accommodation (NI 145) Adults in contact with secondary mental health services in settled accommodation (NI 149) Economic Environment Transport Access to car or van, etc Employmen t 1. Overall employment rate (NI 151) 2. Working age people on out-ofwork benefits (NI 152) 3. Working age people claiming out-of-work benefits in the worst performing neighbourhoods (NI 153) Vulnerable People 1. Adults with learning disabilities in employment (NI 146) 2. Adults in contact with secondary mental health services in employment (NI 150) Other Employment Indicators– e.g.: Unemployment rate, Claimant count, etc Other Average incomes Isolation Rural or urban location Access to services (e.g. from Indices of Deprivation) Voice Bold red = National Indicators Italic grey = optional indicators Satisfaction of people over 65 with home and neighbourhood (NI 138) Lead Agency/ Officer Frequency Reported Lowest Geography Covered Every 10 yrs SOA Comments LA Y ONS, Census LA or PCT LA Y ONS PCT or LA Annual Borough Y ODPM LA or PCT Every 3 years SOA More detailed description of data is available LA Work in progress. Indicators are liable to be added, removed or amended. Appendix 1 – Data Required for JSNA Local Availability Lifestyle/Risk factors Domain v7a Sub-domain Burde n of illhealth an disabili ty Frequency Reported PCT PCT Jo Robinson Annual Quarterly Annual Borough PCT PHIT and Caroline Mansell Annual Postcode Manor PCT PHIT Annual Postcode Smoking 1. Modelled and/or recorded prevalence 2. Quit rates 3. Deaths due to smoking Y Y N Eating habits Modelled and/or recorded eating behaviour Prevalence of breast-feeding at 6-8 weeks from birth (NI 53) N Y PCT Y Alcohol Alcohol-harm related hospital admission rates (NI 39) Modelled and/or recorded drinking behaviour Lowest Geography Covered E.g. from Active People Survey Y Sports England PCT Paul Wicker Every 2 years Ward? Sexual Behaviour Under 18 conceptions (NI 112) Under 16 conceptions Y ONS PCT Diane Osborne Annual Some ward data is available Hypertension Modelled and/or recorded prevalence Y Doncaster Model PCT PHIT Annual Practice N Obesity Modelled and/or recorded prevalence : adults Obesity among primary school age children in Reception Year (NI 55) Obesity among primary school age children in Year 6 (NI 56) Y NCMP PCT PHIT Annual Postcode Y NCHOD ONS PCT PHIT Annual Borough (some LE calculations at ward) All Causes Bold red = National Indicators Italic grey = optional indicators All-Age All-Cause Mortality (NI 120) Life Expectancy Comments Some data is available routinely, data on deaths would need to be estimated fro evidence and death extracts Data on feeding at 6-8 weeks is available, but coverage is around 80%. Coverage for Initiation rates are higher N Physical Activity Other Misc Lead Agency/ Officer Data/Indicator Behaviours Available Source Sub-subdomain A separate local report and action plan was produced by Paul This data is always 2 years out of date, local proxy measures are being developed by the PCT See comment below Work in progress. Indicators are liable to be added, removed or amended. Appendix 1 – Data Required for JSNA Local Availability Domain v7a Sub-domain Sub-subdomain Frequency Reported Lowest Geography Covered Annual Ward Annual Ward PCT PHIT Annual Borough ONS PCT PHIT Annual Borough PBS Diabetes Population Prevalence Model PCT PHIT Annual Practice Data/Indicator Available Source Infant Mortality Y ONS Main causes of death Y ONS Y Manor Dr Foster or NHS Comparator Y Y Hospital admissions – top 10 causes Lead Agency/ Officer PCT PHIT PCT PHIT Comments Self-reported measure of overall health and wellbeing (NI 119) Healthy life expectancy at age 65 (NI 137) Causes considered amenable to healthcare Mortality Modelled v. recorded prevalence Diabetes General General Circulatory Implications – e.g. Life Expectancy/Quality-Adjusted Life Expectancy/Costs from UKPDS Mortality rate from all circulatory diseases under 75 (NI 121) N Y NCHOD Annual Borough Mortality Y NCHOD PCT PHIT Annual Generally, Borough but Postcode from PHMF via PHIT Modelled v. recorded prevalence Y Doncaster Model PCT PHIT Annual Practice CHD Bold red = National Indicators Italic grey = optional indicators PCT PHIT Diabetes, hypertension, cancer, respiratory disease, and circulatory disease are also reported in the recent Public Health Report on Long Term Conditions Work in progress. Indicators are liable to be added, removed or amended. Appendix 1 – Data Required for JSNA Local Availability Domain v7a Sub-domain Sub-subdomain Data/Indicator Hospital admission rate for MI (proxy for incidence) Stroke Available Source Lead Agency/ Officer Frequency Reported Lowest Geography Covered Y Dr Foster or NHS Comparator PCT PHIT Annual Borough Quarterly Trust Annual Postcode Annual Trust Admissions for cardiac revascularisation Y WMSHA Mortality Y NCHOD Y Dr Foster, NHS Comparato r Hospital admission rate for Stroke (proxy for incidence) General Mortality rate from all cancers under age 75 (NI 122) By site Cancer registrations WMSHA Andrea Price or PCT, PHIT PCT PHIT PCT PHIT NCHOD PCT PHIT Annual Generally, Borough but Postcode from PHMF via PHIT WMCIU, CIU or NCHOD PCT PHIT Annual Ward Annual Generally, Borough but Postcode from PHMF via PHIT Annual Practice Annual Borough Annual Borough Cancer Respiratory Infectious STIs Bold red = National Indicators Italic grey = optional indicators Y COPD Mortality Y NCHOD or ONS data PCT PHIT COPD modelled v. recorded prevalence Y Doncaster Model TB notifications Y HPA KC60 GUM STI data, particularly gonorrhoea Y HPA or GUM PCT PHIT Regional Surveillan ce Unit RSU or Manor Work in progress. Indicators are liable to be added, removed or amended. Comments Appendix 1 – Data Required for JSNA Local Availability Domain v7a Sub-domain Sub-subdomain Source Lead Agency/ Officer Frequency Reported Lowest Geography Covered New diagnoses of HIV/Aids Chlamydia in under-25s Late diagnosis of HIV Y HPA or GUM RSU or Manor Annual Borough Annual Borough PCT PHIT PCT Sue Laverty Dental Decay % DMFT in 5-year olds Y NCHOD Mental Dementia e.g. Predictions from POPPI Y? PCT Falls Hospital admissions for Fractured Neck of Femur (proxy for incidence) Y NCHOD PCT PHIT Annual Borough Y? ONS PCT PHIT Annual Borough Y? ONS PCT PHIT Annual Borough Borough Trauma Road accidents Injuries Services Available Data/Indicator People killed or seriously injured on roads Children killed or seriously injured on roads (NI 48) Hospital admissions caused by unintentional and deliberate injuries to children and young people (NI 70) Borough Musculoskeletal Arthritis Admissions for hip and knee replacement Y NCHOD PCT PHIT Annual Disability General Long-term limiting illness Y ONS, Census PCT or LA Every 10 yrs Numbers Physical disability, frailty and sensory impairment Older and Vulnerable People 1. Number of clients 2. Number receiving services in community Social Services Bold red = National Indicators Italic grey = optional indicators Work in progress. Indicators are liable to be added, removed or amended. Comments Appendix 1 – Data Required for JSNA Local Availability Domain v7a Sub-domain Sub-subdomain Data/Indicator Available Source Lead Agency/ Officer Frequency Reported Lowest Geography Covered Y PCT PCT PHIT Annual Practice, Ward Learning disability Older and Vulnerable People 1. Number of clients 2. Number receiving services in community Mental health and Older and Vulnerable People 1. Number of clients 2. Number receiving services in community Substance misuse Older and Vulnerable People 1. Number of clients 2. Number receiving services in community Other vulnerable people 1. Number of clients Number receiving services in community Timeliness of social care assessment (NI 132) Standard of Service Preventative Bold red = National Indicators Italic grey = optional indicators People supported to live independently through social services (NI 136) Carers receiving needs assessment or review and a specific carer’s service, or advice and information (NI 135) Uptake rates for Flu jab, etc Uptake rates for MMR, etc Work in progress. Indicators are liable to be added, removed or amended. Comments Appendix 1 – Data Required for JSNA Local Availability Domain v7a Sub-domain Sub-subdomain Data/Indicator Offer of an appointment at a GUM service within 48 hours Long acting reversible contraception methods as a percentage of all contraception Sexual Health Services Access to NHS funded abortions before 10 weeks gestation Access to NHS funded abortions before 10 weeks gestation (CYP) User perspective on social care Voice User perspective on health care Bold red = National Indicators Italic grey = optional indicators Available Source Lead Agency/ Officer Frequency Reported Lowest Geography Covered Y UNFIY and WMSHA PCT PHIT Monthly Borough Y? PCT PCT Barat Patel ? Practice PCT PHIT Annual and some quarterly Borough (PCT data Postcoded) Y ONS and PCT Comments Annually from ONS but locally PCT has developed a system to monitor trends more frequently The extent to which older people receive the support they need to live independently at home (NI 139) Self-reported experience of social care users (NI 127) National Patients Survey Programme findings for local institutions. Available from http://www.healthcarecommission.org. uk/healthcareproviders/yourlocalhealt hservices.cfm Work in progress. Indicators are liable to be added, removed or amended.