BME 1450 Term Paper.doc
advertisement

1
A Systems Biology Approach to understanding
Osteoporosis
Tayyab S. Khan, M.A.Sc. Candidate
Abstract– Osteoporosis is a silent, multifactorial
disease characterized by low bone mass and an
increased risk of fracture. A variety of risk factors
have been associated with the disease and include
menopause, aging, oxidative stress, genetics and
lifestyle. The multifactorial nature of the disease
combined with complex molecular mechanistic
interactions underlying its pathology, necessitate
development of a system level understanding of the
disease. Although current models for osteoporosis
take into account roles of only a fraction of the
many risk factors associated with the disease, they
provide the framework for developing integrated,
holistic models which can help us design high
efficacy preventative and therapeutic strategies
against the disease.
Index Terms– bone remodeling, menopause,
osteoblasts, osteoclasts, osteoporosis, oxidative
stress, systems biology.
I. INTRODUCTION
O
STEOPOROSIS is a multifactorial,
systemic skeletal disease characterized by
low bone mass and microarchitectural
deterioration of bone tissue, with a consequent
increase in bone fragility and susceptibility to
fracture [1]. It is often referred to as the ‘silent
thief’ as it remains asymptomatic until the
incidence of fracture. Principally affecting old
men and women, it has emerged as a serious
health hazard in recent times and accounts for
1.3 million fractures annually in the United
States, treatment costs of which are in excess of
20 billion dollars annually [2]. As our aging
population is expected to increase from its
current strength of 323 million people to 553
million by 2050 [3], this cost is expected to rise
if effective therapeutic strategies are not
developed against the disease.
Bone is a dynamic mix of three main
types of cells, namely osteoblasts, osteoclasts
and osteocytes, and the extracellular matrix
whose
non-mineralized
(osteoid)
and
mineralized components comprise its structure
[4]. Bone is continually formed and resorbed by
the activities of the mononucleated osteoblasts
and the multinucleated osteoclast cells
respectively. The function of the third, and the
most numerous of all cell types found in bone
tissue, the osteocytes, is less clear. They are
terminally divided osteoblasts, have a high
nucleus to cytoplasm ratio and are known to
communicate with each other and other cells
lining the bone surface to detect bone in need of
repair as well as transmit signals to osteoblast
and osteoclast precursors in bone marrow to
stimulate their differentiation [5]. The coordinated physiology of these cells is responsible
for the process of bone remodeling, which
involves maintenance of a dynamic equilibrium
between bone formation and resorption.
Disturbances in this process that shift the balance
of equilibrium towards bone resorption may
cause decreases in bone mass, as measured by
bone mineral density (BMD) and once the BMD
of a patient falls 2.5 standard deviations below
the mean normal young adult reference range,
they are diagnosed with osteoporosis [6].
A number of risk factors have been
associated with osteoporosis and include
menopause, aging, oxidative stress, genetics, and
lifestyle. This multifactorial nature of the disease
necessitates a comprehensive understanding of
the diverse roles played by each factor in order to
design high efficacy therapeutic strategies
against it. Although models predicting effects of
one of the risk factors on bone health have been
generated, we lack holistic, integrated models
accounting for the relative contributions of
multiple risk factors in increasing an individual’s
risk for osteoporosis. Systems biology provides
us with the tools and framework for development
of an all-inclusive, holistic model for
osteoporosis which accounts for the relative roles
played by multiple risk factors in its pathology of
osteoporosis. This model can help us increase
our understanding of the disease etiology and aid
our quest to develop effective preventative and
therapeutic strategies against osteoporosis.
2
II. RISK FACTORS FOR OSTEOPOROSIS
1. MENOPAUSE
The fact that the one of the two primary
types of osteoporosis (type 1) is known as
postmenopausal osteoporosis underscores the
importance of menopause in increasing the risk
for the disease. Menopause is accompanied by a
deficiency in secretion of estrogen, a group of
hormones principally known for its role in
development and maintenance of female sexual
characteristics. However, it is also important in
the process of bone remodeling and is known to
suppress bone resorption by osteoclasts. Thus
estrogen
deficiency
at
menopause
is
accompanied by what is known as a high bone
turnover state, an i.e. increase in bone resorption
and a corresponding, but insufficient, increase in
bone formation. This imbalance causes loss of
bone mass and leads to an increased risk for
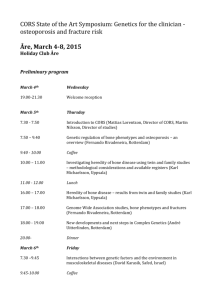
osteoporosis (Figure 1) [7]. This is evident in the
10-fold increase in bone loss after menopause [8],
which translates in as many as 44 million
postmenopausal
women
suffering
from
osteoporosis today in the United States [9].
Data accumulated from different studies
on postmenopausal osteoporosis is now being
used to generate computer-based simulation
models to predict bone mass in years following
menopause. These include computer simulation
studies showing bone remodeling in trabecular
(cancellous) bone [10], studies analyzing the
effect of age at menopause in development of
osteoporosis [11], and simulation models
predicting effects of antiresorptive treatments on
bone volume after menopause [12]. We are, thus,
beginning to see the application of a systems
biology approach to study postmenopausal
osteoporosis.
In contrast with postmenopausal
osteoporosis, age-related osteoporosis is not
accompanied by increased bone turnover. Instead,
it is proposed that following attainement of peak
bone mass at 25-30 years of age (Fig 1), there is
a decrease in proliferative capacity of
osteoprogenitors that give rise to the bone
forming, osteoblast cells. Thus in advancing age,
enough osteoblasts are not present to balance
bone resorption by osteoclast cells, leading to a
decrease in bone mass and eventually an
increased risk for osteoporosis [13].
Like postmenopausal osteoporosis, we
are beginning to generate simulation models for
age-related bone loss. These include models
predicting effects of lead exposure to accelerate
normal bone loss due to aging [13], effect of age
on BMD in Chinese population [14], and models
analyzing the effects of multiple factors, peak
BMD, advancing age, and age at menopause on
the risk for osteoporosis [11]. Thus we are
beginning to see a trend towards integrating
multiple risk factors in creating models for the
disease condition. With accumulation of more
data, it is hoped that we can accommodate other
risk factors in these models so as to improve our
understanding of osteoporosis.
2. AGING
Like menopause, age plays an important
role in the pathophysiology of osteoporosis. It is
due to this reason that the second type of primary
osteoporosis (type II) is also known as agerelated osteoporosis. The National Osteoporosis
Foundation estimate that 1 in 2 white females
and 1 in 4 white males over fifty years of age
will sustain at least one osteoporosis-related
fracture in their lifetime attests to the important
role growing age can have in the development of
osteoporosis [9].
Figure 1: Variation in BMD of women. In
elderly women, low BMD can arise owing to the
attainment of low peak bone mass (purple),
increased bone loss due to early menopause (blue)
or greater than average rate of post-menopausal
bone loss ('fast loser', in green). [21]
3
3. OXIDATIVE STRESS
Oxidative stress is defined as an
increase in free radicals and reactive oxygen
species (ROS) and a corresponding decrease in
the antioxidant defences in the body. ROS
include free radicals, hydrogen peroxide,
hydroxyl radical and superoxide anion which
may be produced in response to environmental
agents, e.g. radiation, as well as endogenous
oxygen metabolism. Owing to the presence of
singlet oxygen containing an unpaired electron,
ROS are extremely reactive in nature, and can
react with DNA, proteins, and lipids to cause
structural and functional changes in them. In so
doing, they can contribute to the pathogenesis of
a variety of disease conditions such as
atherosclerosis, carcinogenesis, male infertility,
and osteoporosis [15-16].
Research interest towards understanding
the role of oxidative stress in the pathology of
osteoporosis emerged from studies finding
decreased
endogenous
and
exogenous
antioxidants, vitamins C, E and A, activities of
enzymes involved in inhibiting ROS, superoxide
dismutase, glutathione peroxidase, etc. in plasma
samples of osteoporotic women [17]. Since then,
studies have shown that oxidative stress induced
by hydrogen peroxide stimulates bone loss both
by suppressing differentiation of osteoblasts as
shown by a decrease in osteoblast differentiation
markers alkaline phosphatase (ALP), type 1
collagen,
and
colony
forming
unitosteoprogenitor (CFU-O) formation [18], as well
as by increasing bone resorption by osteoclasts
in a dose dependent manner [19]. These studies,
in addition to the ones showing that treatment
with antioxidants such as lycopene can increase
mineralized bone nodule formation by
osteoblasts, and can inhibit both cell
differentiation and bone resorption of osteoclasts
give credence to the view that oxidative stress
can increase risk for osteoporosis (Tayyab Khan,
unpublished results).
Owing to the relative recent association
between oxidative stress and osteoporosis,
simulation models predicting effects of oxidative
stress on bone mass have not been developed.
From personal experience, however, the author
has participated in at least one such attempt
underway at St. Michael’s Hospital, Toronto,
through a clinical study employing 200
postmenopausal women who are risk for
developing osteoporosis. It is envisaged that
their oxidative stress markers, DNA oxidation
measured by levels of 8-hydroxydeoxyguanosine
(8OHdG), protein oxidation using loss of
reduced thiol groups, and lipid peroxidation
using malondialdehyde levels be measured.
These levels would then be correlated with their
endogenous and exogenous antioxidant defences,
DNA polymorphisms in antioxidant genes
superoxide dismutase, glutathione peroxidase,
catalase etc., and levels of antioxidants,
carotenoids, lycopene, vitamins A and E,
polyphenols in plasma to find their total
antioxidant
potential.
Measurements
of
oxidative stress and antioxidant potential of an
individual would be compared with their bone
turnover markers and BMD. The data obtained
would then be used to construct a model showing
any possible association between oxidative stress
and osteoporosis among postmenopausal women.
Once completed, this would be the first
application of a systems biology approach in
understanding the role of oxidative stress in the
etiology of osteoporosis.
4. GENETICS
In a post genomic era, identification of
a genetic basis for osteoporosis has inspired
many researchers. Twin studies showing high
heritability estimates for bone mass, size and
structure provided important clues to the genetic
basis of osteoporosis [20]. Researchers have
employed candidate gene approaches, linkage
studies, genome scans in sibling pairs, etc. to
discover a number of genes, and their
interactions, playing a role in the pathogenesis of
osteoporosis [20]. While the heritability of bone
formation has been well established, the same
link between genes and bone loss has only begun
to be identified [21]. Studies have identified a
number of genes associated with osteoporosis,
most studied of which are genes for Collagen
type 1 I (COL1A1), estrogen receptors (ER),
and vitamin D receptors (VDR) (Table 1).
Although the association between osteoporosis
and polymorphisms in both VDR, involved in
calcium absorption in small intestine, and ER,
the estrogen receptor, have been less convincing,
and at times contradictory. Polymorphisms in
COL1A1 gene have been consistently and
convincingly correlated with low bone mineral
density and increased fracture risk. COL1A1,
along with Collagen type 1 II (COL1A2) is a
major component of collagen, the main structural
protein in the skeleton. This explains why
polymorphisms in the gene have been correlated
4
with low bone mineral density (BMD) and a
greater risk of fracture [21].
The
advent
of
cDNA
and
oligonucleotide microarrays have provided us
with high-throughput tools to study the genetic
basis of a multifactorial, multigenic disease such
as osteoporosis. We are beginning to see studies
showing differential expression of as many as
184 genes in the early osteoblast differentiation
[22]. This information, although gained from a
mouse cell line is bound to contain variations
from human models, does provide us with a
good starting point in our search for candidate
genes for osteoporosis. Comparison of data
gained from this model with models employing
other cell lines, or data for polymorphisms found
in osteoporotic patients can help us determine the
relative roles played by these genes in increasing
risk for osteoporosis. It may eventually pave the
way for developing models for osteoporosis on
the basis of a genetic predisposition for the
disease.
Table 1 – Candidate genes associated with
BMDa
Candidate
Genes
COL1A1
Protein
Collagen,
type 1 1
ESR1
Estrogen
Receptor 1()
VDR
Vitamin D
Receptor
a
Adapted from [20].
Chromosomal
Location
17q21.3-q22.1
6q25.1
12q12-q14.
5. LIFESTYLE FACTORS
A number of lifestyle factors have also
been associated with osteoporosis, two of which
are presented as follows.
(a) DIET
A variety of dietary components have
been studied for their possible association with
osteoporosis. These include intakes of calcium,
vitamin D, alcohol, caffeine, and antioxidants, to
name a few. Since calcium is the most important
mineral present in our bones, it is important to
maintain adequate calcium intakes in accordance
with the recommended daily allowances (RDA)
for specific age groups to maintain bone mass.
However, it should be noted that vitamin D
intake should also be maintained within the
recommended level of 200-400 International
Units/day since in its active form, 1,25–
dihydroxyvitamin D3 (1,25-(OH)2D3), helps in
absorption of calcium in the small intestine,
duodenum, by increasing gene expression of
calbindin, a translocator of calcium [23].
Research
also
correlates
small/moderate
consumption of alcohol positively with BMD,
while both smoking and caffeine intake showed a
negative association with BMD at a number of
sites in the skeleton [24]. This information can
help us adopt healthy dietary practices to
maintain bone mass.
(b) PHYSICAL ACTIVITY
Physical activity is another lifestyle
factor known to exert effects on bone health.
Studies have negatively correlated exercise and
bone turnover markers (which are high in
postmenopausal osteoporosis) among postmenopausal women, revealing the role of
physical activity in the management of the
disease condition [25]. This information is
supplemented by studies showing higher BMD
in 15-42 years old males and females following
an exercise regimen in comparison to those
having low levels of physical activity [26].
However, there are other studies correlating
intense physical activity, as undertaken by
dancers, gymnasts and professional athletes with
amenorrhea, absence or cessation of menstrual
periods. As this is often accompanied by low
estrogen levels, it leads to increased bone loss
through mechanisms similar to postmenopausal
osteoporosis, and results in an increased risk for
osteoporosis later in life [27]. Thus it appears
that there are some threshold levels until which
physical activity can be beneficial and exceeding
them have negative effects on bone mass. A
systems biology approach can help us identify
those levels so as to help us maintain bone mass
and reduce the risk for osteoporosis.
CONCLUSION
The above discussion presents an
analysis of the various factors associated with
osteoporosis and entails some approaches to
model the disease condition based on specific
risk factors. As we proceed further in our quest
to understand the pathology underlying
osteoporosis, it is important to integrate the new
information with that gathered from earlier
studies. Thus we can begin to generate
multifactorial,
multigenic
models
for
5
osteoporosis and test them for accuracy in those
at risk for developing it. Such a holistic approach
can not only help us increase our understanding
of the disease condition, but may also pave the
way for developing successful treatment
strategies against the leading cause of morbidity
and mortality in our elderly population.
REFERENCES
[1]
Consensus Development Conference, “Diagnosis,
prophylaxis and treatment of osteoporosis,” Am. J. Med., vol.
94, pp. 646-650, 1993.
[2]
M. A. Moyad, “Osteoporosis: A rapid review of risk
factors and screening methods,” Urol. Oncol., vol. 21, pp.
375-379, 2003.
[3]
A. J. Shepherd, “An overview of osteoporosis,” Alt.
Ther., vol. 10, pp. 26-33, 2004.
[4] C. M. Bono and T. A. Einhorn, “Overview of
osteoporosis:pathology and determinants of bone strength,”
Eur. Spine. J., vol 12. suppl. 2, pp. S90-96, 2003.
[5]
R.L. Jilka, “Biology of the basic multicellular unit and
the pathophysiology of osteoporosis,” Med. Pediatr. Oncol.,
vol. 41, pp. 182-185, 2003.
[6]
T. V. Nguyen, J. R. Center and J.A. Eisman,
“Osteoporosis:
underrated,
underdiagnosed
and
undertreated,” Bone and Joint Disorders: Prevention and
Control, vol. 180, pp. S18-S24, 2004.
[7]
B. R. Troen, “Molecular mechanisms underlying
osteoclast formation and activation,” Exp. Gerontol., vol. 38,
pp. 605-614, 2003.
[8]
S. C. Manolagas and R .L. Jilka, “Emerging insights
into the pathophysiology of osteoporosis,” N. Eng. J. Med.,
vol. 332, pp. 305-311, 1995.
[9]
Disease
Statistics.
National
Osteoporosis
Foundation.http://www.nof.org/advocacy/prevalence/index.ht
m (Accessed October 15, 2004).
[10] S. Tayyar, P. S. Weinhold, R. A. Butler, J. C.
Woodward, L. D. Zardiackas, K. R. St. John, J. M. Bledsoe,
and J. A. Gilbert, “Computee simulation of trabecular
remodeling using a simplified structural model,” Bone, vol.
25, pp. 733-739, 1999.
[11]
C. J. Hernandez, G.S. Beaupre and D.R. Carter, “A
theoretical analysis of the relative influences of peak BMD,
age-related bone loss and menopause on the development of
osteoporosis,” Osteoporos. Int. vol. 10, pp. 843-847.
[12] J.C. van der Linden, J.A.N. Verhaar, H.A.P. Pols, and
H. Weinans, “A simulation model at trabecular level to
predict effects of antiresorptive treatment after menopause,”
Calcif. Tissue Int, vol. 73, pp. 537-544, 2003.
[13]
E.J. O’Flaherty, “Modeling normal aging bone loss
withconsideration of bone loss in osteoporosis,” Toxicol. Sci.,
vol., 55, pp. 171-188, 2000.
[14] S.Z. Xu, W.M. Huang, and J.Y. Ren, “The new model
of age-dependent changes in bone mineral density,” Growth
Dev. Aging, vol. 61, pp.19-26. 1997.
[15] S.S. Varanasi, R.M. Francis, C.E.M. Berger, S.S.
Papiha, and H.K.Datta, “Mitochondrial DNA deletion
associated oxidative stress and severe male osteoporosis,”
Osteoporos Int., vol. 10, pp. 143-149. 1999
[16] H. Isomura, et al., “Bone metabolism and oxidative
stress in postmenopausal rats with iron overload,” Toxicology,
vol. 197, pp. 93-100, 2004.
[17] D. Maggio, et al., “Marked decrease in plasma
antioxidants in aged osteoporotic women: results of a crosssectional study,” J. Clin. Endocrinol. Metab. vol. 88, pp.
1523-7, 2003.
[18] X.C. Bai, D. Lu, J. Bai, H. Zheng, Z.Y. Ke, X.M. Li,
and S.Q. Luo, “Oxidative stress inhibits osteoblastic
differentiation of bone cells by ERKand NF-kappaB,”
Biochem Biophys Res Commun. vol. 314, pp. 197-207, 2004.
[19] J.H. Fraser, M.H. Helfrich, H.M. Wallace, and S.H.
Ralston, “Hydrogen peroxide, but not superoxide stimulates
bone resorption in mouse calvariae,” Bone, vol. 19, pp. 223-6,
1996.
[20] M. Peacock, C.H. Turner, M.J.Econs, and T. Faroud,
“Genetics of osteoporosis,” Endoc. Rev., vol. 23, pp. 303-326,
2002.
[21] M.A. Brown, and E.L Duncan, “Genetic studies of
osteoporosis,” Expert Rev. Mol. Med., vol. 1(14), pp1-18,
1999.
[22] D. S. deJong, B.L. Vaes, K.J. Dechering, A. Feijan,
J.M. Hendriks, R. Wehrens, C.L. Mummery, E.J. van Zoelen,
W. Olijwe, and W.T. Steegenga, “Identification of novel
regulators associated with early phase osteoblast
differentiation,” J Bone Miner Res. vol. 19., pp. 947-58, 2004.
[23] B.W.Hollis, and C.L.Wagner, “Assessment of dietary
vitamin D requirements during pregnancy and lactation,” Am.
J. Clin. Nutr. vol. 79, pp. 717-726, 2004.
[24]
M. J. Grainge, C.A. Coupland, S.J. Cliffe, C.E.
Chilvers, and D.J. Hosking, “Cigarette smoking, alcohol and
caffeine consumption and bone mineral density in
postmenopausal women. The Nottingham EPIC study group”
Osteoporos Int. vol. 8, pp. 355-63, 1998.
[25] S. Yamazaki, S. Ichimura, J. Iwamoto, T. Takeda, and
Y. Toyama, “Effect of walking exercise on bone metabolism
in postmenopausal women with osteopenia/osteoporosis,” J.
Bone. Miner. Metab., vol. 22, pp. 500-508, 2004.
[26] H. Dupe, P. Gardsell, O. Johnell, B.E. Nilsson, and K.
Ringsberg, “Bone mineral density, muscle strength and
physical activity. A population based study of 332 subjects
aged 15-42 years,” Acta. Orthop. Scand., vol. 68, pp. 97-103,
1997.
[27] S. Bass, G. Pearce, N. Young, and E. Seeman, “Bone
mass during growth: the effects of exercise. Exercise and
mineral accrual,” Acta. Univ. Carol., vol. 40, pp3-6, 1994.