Multiple Myeloma - University of Arkansas for Medical Sciences
advertisement

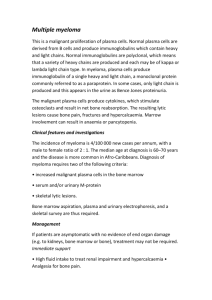
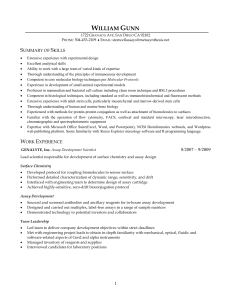
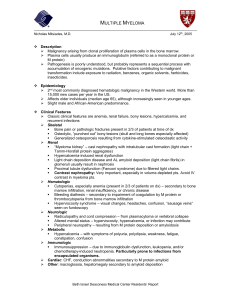
Radiology Review Edgardo J. C. Angtuaco, MD Athanasios B. T. Fassas, MD Ronald Walker, MD Rajesh Sethi, MD Bart Barlogie, MD Index terms: Bone marrow, diseases, 48.3452 Bones, CT, 48.12111 Bones, MR, 48.121411, 48.121412, 48.121413, 48.121415 Myeloma, 48.3452 Review Published online before print 10.1148/radiol.2311020452 Radiology 2004; 231:11–23 Abbreviations: FDG ⫽ fluorodeoxyglucose Ig ⫽ immunoglobulin MM ⫽ multiple myeloma STIR ⫽ short tau inversion recovery 1 From the Department of Radiology (E.J.C.A., R.W., R.S.) and the Myeloma Institute (A.B.T.F., B.B.), University of Arkansas for Medical Sciences, 4301 W Markham, Slot 596, Little Rock, AR 72205. Received April 22, 2002; revision requested June 19; revision received March 4, 2003; accepted March 17. Address correspondence to E.J.C.A. (e-mail: angtuacoedgardoj @uams.edu). © RSNA, 2004 Multiple Myeloma: Clinical Review and Diagnostic Imaging1 Multiple myeloma (MM) is a malignant clonal neoplasm of plasma cells of Blymphocyte origin that commonly results in overproduction of large amounts of monoclonal immunoglobulins. Important advances in the therapeutic management of this disease in the past decade have resulted in higher rates of durable complete remission, prolonged event-free survival, and improved overall survival. Clearer understanding of the effects of abnormal plasma cells on bone has led to therapeutic approaches that help prevent vertebral body fractures. Current imaging technologies and, in particular, survey marrow studies with magnetic resonance (MR) imaging have improved detection of the extent and location of disease in MM patients. In newly diagnosed cases, MR surveys of the axial skeleton accurately demonstrate the extent of disease— diffuse or focal involvement—and the presence of associated compression fractures and cord compression. After treatment, MR images show the effects of treatment and the presence of residual disease. Multiple sites of focal bone lesions detected on MR studies allow a more appropriate choice of biopsy site than the usual random iliac marrow biopsy. Use of MR to determine biopsy sites and computed tomographic guidance for biopsy performance have increased the safety and accuracy of sampling. These biopsies have resulted in increased identification of cytogenetic abnormalities, particularly the presence of chromosome 13 deletion, which is a grave prognostic indicator in MM. © RSNA, 2004 Multiple myeloma (MM) is a clonal B-lymphocyte neoplasm of terminally differentiated plasma cells. It accounts for approximately 1% of all malignant diseases and represents about 10% of hematologic malignancies. The annual incidence of newly diagnosed cases in the United States is three to four per 100,000 population per year, with an estimated 14,000 new cases each year. The median age at diagnosis is 65 years, and about 3% of patients are younger than 40 years (1). The disease has a higher incidence in men and African Americans. The cause of MM is unknown. Radiation exposure increases the risk, as evidenced by a higher than expected rate of disease in atomic bomb survivors, radiation workers, and postirradiated patients with ankylosing spondylitis. The origin of the malignant plasma cell remains a mystery. Data from cloning and gene-sequencing studies strongly imply that the malignant clone in MM arises from a late cell in B-cell development (2,3). CLINICAL PRESENTATION The clinical findings vary from totally asymptomatic in patients whose disease is discovered incidentally to life-threatening symptoms. The common clinical presentations are fatigue and bone pain (back or ribs) with or without associated fractures or infection. In 15%–30% of patients (4), the finding at presentation is hypercalcemia with concomitant renal insufficiency caused by precipitation of monoclonal light chains in the collecting tubules (5). Ten percent of patients present with other symptoms, including hyperviscosity syndrome, compression of the spinal cord (Fig 1), radicular pain, soft-tissue deposits, or bleeding problems. In patients who are asymptomatic, the disease is incidentally discovered because of laboratory findings of anemia or hyperproteinemia. The hallmark of MM is the detection in blood and/or urine of a monoclonal protein, M protein, produced by the abnormal plasma cells. Serum protein electrophoresis reveals a 11 Radiology localized band in the globulin part of the ␣ (immunoglobulin [Ig] A) or ␥ (IgG) region in 80% of patients. The remaining 20% of patients will have either hypogammaglobulinemia or a normal-appearing pattern (nonsecretory type). By using the more sensitive techniques of immunofixation and immunoelectrophoresis, M protein (in serum or/and urine) will be detected in 99% of patients (6). The IgG isotype is seen in 60% of MM patients; the IgA isotype, in 25%; the IgD isotype, in 1%; the IgM isotype in 1%; and light chain disease, in 20%. Once the diagnosis is suspected, a radiographic skeletal survey and bone marrow aspiration and biopsy are performed. Samples are sent for plasma cell labeling index and cytogenetic analyses. Minimal criteria for establishment of a diagnosis of MM should be the detection of at least 10% abnormal plasma cells in a random bone marrow biopsy specimen and M protein in either the serum (usually ⬎3 g/dL) and/or urine (usually ⬎1 g/24-hour collection). Osteolytic lesions on a skeletal survey may be found (7). In most patients, the diagnosis of MM is established without difficulty. CLINICAL STAGING AND PROGNOSIS In patients known to have MM, clinical stage is based on the Durie-Salmon system (8) (Table 1). Staging criteria are simple and help estimate suspected tumor burden. This system is based on a combination of clinical factors: amount of M protein, serum hemoglobin level, serum calcium level, number of lytic bone lesions on a skeletal radiographic survey, and renal function. The staging system is used as a predictor of patient outcome and is currently used as a standard for ongoing clinical trials. Prognosis for the disease is highly variable, with survival ranging from a few months to more than 10 years (9). In recent years, advances in the treatment of the disease have resulted in substantially improved clinical outcomes, with improved overall survival and better response to chemotherapeutic regimens, particularly high-dose therapy. Other prognostic factors have been developed that help better identify the subgroups of patients with different outcomes and tailor treatment intensity to disease risk. Serum 2-M level is one of the most important prognostic factors in MM. The level is a measure of tumor burden and renal function (10). C-reactive protein level is another important predictive factor. C12 䡠 Radiology 䡠 April 2004 Figure 1. Multiple plasmacytomas with cord compression. (a) Sagittal T1-weighted spin-echo (repetition time msec/echo time msec, 400/15) (left) and short tau inversion-recovery (STIR; repetition time msec/echo time msec/inversion time msec, 2,000/150/20) (right) magnetic resonance (MR) images of thoracic spine show scattered focal lesions involving vertebral bodies and posterior elements of thoracic spine. Both (b) transverse (600/15) and sagittal (a, left) T1-weighted spinecho MR images show cord compression by a focal expansile mass (arrow) at the T10 spinous process. reactive protein is a surrogate marker of interleukin 6, which is an osteoclast-activating factor. The combination of high levels of C-reactive protein and 2-M indicates a poor prognosis in MM patients who were treated with conventional chemotherapy (11). The plasma cell labeling index reflects the proliferative capacity of plasma cells. The index typically increases during disease progression (12). The median survival of patients with a low plasma cell labeling index and low -2 M level who are treated with conventional chemotherapy is 71 months, compared with 17 months when both parameters are elevated (13). Elevated lactate dehydrogenase levels are predictive of short survival, as they are frequently associated with plasmablastic morphology, extramedullary sites of disease, and adverse-risk cytogenetic abnormalities (14). The presence of cytogenetic abnormalities has recently emerged as the most important prognostic factor in MM. Abnormal karyotypes are observed in 30%–50% of MM patients (15)—more frequently in patients with relapse (35%– 63%) than in those with newly diagnosed disease (20%–30%). Karyotypic abnormalities are complex, involving more than three chromosomes in 80% of the patients (16). Multiple trisomies and transAngtuaco et al TABLE 1 Durie-Salmon Staging System for MM Radiology Stage and Criteria burden† I: Low tumor Hemoglobin level Serum calcium level Radiograph Low paraprotein level Serum IgG Serum IgA Urine light chain II: Intermediate tumor burden All criteria III: High tumor burden‡ Hemoglobin level Serum calcium level Radiograph High paraprotein level Serum IgG Serum IgA Urine light chain Associated renal involvement A: serum creatinine level B: serum creatinine level Value* ⬎10 g/dL (100 g/L) ⬍12 mg/dL (3 mmol/L) No bone destruction, or solitary plasmacytoma ⬍5 g/dL (0.05 g/L) ⬍3 g/dL (0.03 g/L) ⬍4 g/24 h Between values for stage I and values for stage III ⬍8.5 g/dL (85 g/L) ⬎12 mg/dL (3 mmol/L) More than two advanced lytic lesions ⬎7 g/dL (0.07 g/L) ⬎5 g/dL (0.05 g/L) ⬎12 g/24 h ⬍2 mg/dL (177 mol/L) ⬎2 mg/dL * Value in parentheses is in SI unit. † All criteria must be satisfied. ‡ Any criterion must be satisfied. locations are the most common abnormalities. In patients treated with high-dose chemotherapy and autologous stem cell transplantation, a particularly poor outcome was observed in the presence of any translocation or abnormality involving 11q and partial or complete deletion of chromosome 13 (17). MYELOMA BONE DISEASE Before a discussion of imaging findings in MM, it is important to understand myeloma bone disease. The effects of abnormal plasma cells on bone lead to severe bone pain and skeletal fractures, especially spinal compression fractures. Histologic studies of bone have revealed excessive bone resorption in the vicinity of the myeloma cells, with severe inhibition of bone formation (18). Once myeloma cells invade the bone marrow, they adhere to the stromal cells and induce secretion of osteoclast-activating factors, including interleukins 6 and 1 and tumor necrosis factor–. These factors prompt the stromal cells and osteoblasts to secrete tumor necrosis factor–related induced cytokine, or TRANCE, a member of the tumor necrosis factor family (19), which induces differentiation and maturation of osteoclast progenitors (20). The activity of TRANCE can be blocked by osteoprotegerin. The delicate balance between TRANCE and osteoprotegerin, which normally regulates the osteoclastic activity in healthy individuals, Volume 231 䡠 Number 1 is totally disrupted in patients with MM. This disruption is due to overproduction of TRANCE and inactivation of osteoprotegerin by elevated amounts of syndecan-1, a molecule actively shed from the plasma cell surface. Furthermore, unchecked osteoclastic activity promotes the production and release from stromal cells of various cytokines, which lead, directly or indirectly, to further MM clone proliferation. A vicious cycle, with bone destruction “feeding” tumor growth and MM cells promoting bone destruction, is therefore set in motion (21). This set of factors leads to the common findings in MM: severe osteopenia and multiple spinal compression fractures. This vicious cycle can be broken by the use of bisphosphonates. These agents (used in conjunction with cytotoxic chemotherapy) have been found to be superior to chemotherapy alone in decreasing skeletalrelated events in MM patients, such as need for radiation therapy, pathologic fractures, and bone pain (22). Besides their skeletal effects (achieved through direct osteoclast inhibition), bisphosphonates may have an antimyeloma effect (23), and their use may lead to prolonged survival in myeloma patients (24). IMAGING STUDIES The role of imaging in the work-up of patients with MM consists of studies that allow recognition of the effects of my- eloma cells on the skeletal system. In the past, these studies included radiographic skeletal surveys, computed tomography (CT), and nuclear medicine bone scanning (7). Recently, MR imaging of bone marrow has allowed a direct look at the actual tumor burden within the bone marrow (25–30). Direct visualization of marrow disease allows assessment of the extent of disease in newly diagnosed cases and of the effects of therapy. More recently, positron emission tomography (PET) with fluorodeoxyglucose (FDG) has been used to study relapsing patients in whom recurrent disease is not easily detectable with routine imaging. PET, in this instance, has been found to aid in detection of unsuspected sites of medullary and extramedullary disease (31). SKELETAL RADIOGRAPHY AND CT Skeletal radiography continues to be the primary diagnostic study to aid in detection of destructive bone changes in MM. Estimates suggest that approximately 50% of bone destruction must occur before there is radiographic demonstration of the abnormality and that 75% of patients with MM will have positive radiographic findings (28). Four distinct forms of involvement have been described: the solitary lesion (plasmacytoma), diffuse skeletal involvement (myelomatosis), diffuse skeletal osteopenia, and sclerosing myeloma (32). Plasmacytomas typically are lytic lesions that primarily affect the spine, pelvis, skull, ribs, sternum, and proximal appendages (28). The skeletal radiographic survey continues to have an important role in the Durie-Salmon clinical staging criteria for newly diagnosed MM. The presence of two clearly defined lytic lesions indicates high tumor burden and stage III disease (8). In addition, the skeletal survey is used to judge progression of disease and has a complementary role to MR imaging in following the course of disease in patients with MM (33). Diffuse myelomatosis classically manifests as osteolytic lesions with discrete margins and uniform size. These lesions are often subcortical and elliptic and may coalesce into large segments of destruction. Diffuse skeletal osteopenia without well-defined lytic lesions predominantly involves the spine. Multiple compression fractures may be seen with this condition. Bone sclerotic lesions are seen in MM and are associated with the polyneuropathy, organomegaly, endocrinopaMultiple Myeloma 䡠 13 Radiology thy, monoclonal gammopathy, and skin changes, or POEMS, syndrome (34,35). CT is a sensitive tool for detection of the bone-destructive effects in MM (Fig 2). CT findings consist of punched-out lytic lesions, expansile lesions with softtissue masses, diffuse osteopenia, fractures, and, rarely, osteosclerosis (28,36) (Fig 3). Recently, Mahnken et al (36) compared multi– detector row CT with conventional radiography and MR imaging in 18 patients with newly diagnosed MM. Multi– detector row CT was superior to conventional radiography for defining lytic lesions and, in combination with MR imaging, aided in staging the extent of disease. Multi– detector row CT allowed a better evaluation of areas at risk for fracture than did MR imaging. Our experience with the role of CT in MM has been with its adjunctive role in defining possible lytic or sclerotic lesions and in guidance for spinal and pelvic biopsy of MR imaging– defined focal lesions (37). NUCLEAR MEDICINE STUDIES Utilization of the various nuclear medicine radiopharmaceuticals in MM relate to either a direct association with tumor biology (ie, imaging of tumor cells) or an indirect effect (eg, imaging of compression fractures, dystrophic calcifications). MM is primarily an osteolytic neoplasm. However, detection of bone involvement with the usual technetium 99-m (99mTc)based bone scanning agents relies on an osteoblastic response of the skeletal system for uptake. Bone scans obtained with 99m Tc have therefore resulted in underappreciation of the extent of disease (34,35, 38 – 40). In a report (34) comparing the skeletal radiographic survey with bone scans, uptake of the radioisotope in radiographically abnormal regions occurred in 44% of cases, normal findings were seen in 48%, and diminished uptake was seen in 8%. Lesions that are well defined on bone scans are the result of complications in MM: namely, osteoblastic response to a compression fracture of a vertebral body or pelvic insufficiency fracture, soft-tissue calcifications within a plasmacytoma (41), or tumor-associated amyloidosis (42). In recent efforts to image MM, investigators have turned to radiopharmaceuticals that allow direct imaging of tumor physiology. Agents known to accumulate in tumor tissue, such as gallium 67 (67Ga) citrate, thallium 201 (201Tl) chloride, 99m Tc sestamibi, or FDG PET have all met with greater success in imaging MM than have typical bone scanning agents. 14 䡠 Radiology 䡠 April 2004 Figure 2. Multiple compression fractures on CT and MR images. Comparative images from sagittal reformatted CT data set (left) and sagittal STIR MR image (2,000/150/20) (right) of thoracic spine show multiple compression fractures of thoracic vertebral bodies, with severe thoracic kyphosis and marked osteolysis of the T1 vertebral body (arrow). 67 Ga citrate localizes in areas of active tumor either through primary localization within the tumor or through the secondary “inflammatory response” induced by the tumor. This inflammatory response is evidenced by the associated presence of mononuclear cell and lymphocytic infiltrates observed with the plasma cells. Whether these mechanisms act singly or in combination remains unknown (43– 46). 67Ga is not likely to be used in tumor detection in MM owing to its expense, lack of advantage over sestamibi or PET imaging, and possible need for multiday scanning. In instances where infection is suspected in MM patients, 67Ga citrate may be used and uptake by the tumor may be observed. 201 Tl chloride has also been used in the detection of MM. The mechanism of uptake is either increased metabolic demands of the tumor or secondary inflammatory response induced in the marrow (47). A recent study comparing 201Tl and 99mTc bone scans in MM found 201Tl to be promising in detection of disease owing to its complementary detection rates (48). The role of this agent in MM is, however, currently supplanted by 99mTc sestamibi, which shows similar localization on images of higher quality and lower cost. 99m Tc sestamibi is thought to accumulate preferentially in malignant cells, ow- Figure 3. Lytic expansile mass of C5. Transverse CT image at level of C5 shows expansile soft-tissue mass along right side of C5 vertebral body, with associated bone destruction. ing to a higher transmembrane electric potential that results from a higher metabolic rate in MM cells (49–52). The primary site of localization is in the mitochondria (52,53). Pace et al (50) classified the activity patterns of 99mTc sestamibi as focal, diffuse, a combination of focal and diffuse, or normal in 39 patients with MM. Activity was correlated with active disease, and norAngtuaco et al Radiology Figure 4. One-month comparative FDG PET images show good response to therapy. Left: Initial image shows increased metabolic activity in spine and pelvis. Note separate focal mass (arrow) in left iliac region. Right: Posttreatment (1-month follow-up) study shows decrease in overall metabolic activity in spine and pelvis, with resolution of left iliac mass and residual disease (arrowhead) in left sacrum. Decrease in metabolic activity indicates good response to chemotherapeutic agents. gested in 75% of patients overall and in 100% of patients with mixed focal and diffuse disease (Fig 4). An additional use for FDG PET in patients with solitary plasmacytoma is to aid in detection of other unsuspected sites. El Shirbiny et al (59) reported a case of combined use of 99m Tc sestamibi and FDG PET, where the former seemed to correlate better with overall extent of disease and the latter with areas of active disease. One final use of nuclear medicine in MM is in the evaluation of patients for the treatment of painful bone metastases. Isotopes such as strontium 89 (89Sr) have been used to palliate the pain in MM (60). Because response is dependent on osteoblastic activity, a purely osteolytic process might not be effectively treated. A routine bone scan can help document the presence of osteoblastic response in these patients and is therefore helpful to predict response to 89Sr treatment. MR IMAGING Figure 5. Skull involvement of MM. (a) Craniovertebral junction disease. Unenhanced sagittal T1-weighted spin-echo MR images (450/15) of the head in two patients. Left: Clivus shows diffuse hypointensity with nonexpansile distal mass (arrow). Right: Focal expansile mass of dens (arrowhead) causes compression of cervicomedullary junction. (b) Multiple calvarial diploic lesions. Coronal fat-suppressed contrast-enhanced T1-weighted spin-echo MR image (550/15) of the head shows multiple focal areas of enhancement (arrowheads) of the diploë with an expansile mass (arrow) in left lateral frontal diploë. mal scans were related to remission. Unfortunately, the value of follow-up studies is limited because of the known development of multidrug resistance by myeloma cells, which causes blockade of the accumulation of the sestamibi (54 –57). Fluorine 18 FDG PET has been reported Volume 231 䡠 Number 1 in MM (58,59). In a series of 43 patients with MM and solitary plasmacytoma, Shirrmeister et al (31) reported focal tracer uptake on FDG PET scans of 38 of 41 lesions (sensitivity, 93%) with known osteolytic pattern. FDG PET depicted 71 additional lesions missed on radiographs in 14 patients. Some of these additional lesions were confirmed by other means in 10 of these patients, which resulted in a change of disease management in 14% of the patients. Diffuse disease was sug- MR imaging findings in MM closely reflect the broad spectrum of pathologic tumoral spread (25–30). The distribution of malignant plasma cells in MM includes sites that show normal areas of active hematopoiesis in adults. These are in the bone marrow of the axial skeleton. The combination of the diagnostic accuracy afforded by current MR units and the extensive coverage by phased-array spine coils allow the acquisition of survey studies of long segments of the axial skeleton within a reasonable time period. MR images can then be used to determine the exact location, size, and local compressive effects of the focal plasmacytomas and possible associated fractures. MR images can help precisely define radiation therapy ports used in the primary treatment of patients with solitary bone plasmacytoma (61). Posttreatment MR images help define response to treatment (62– 64). An additional use of MR imaging is the delineation of the effects and complications of the highly involved therapeutic protocols, to help explain whether observed clinical findings are the result of complications of the disease or of a failure to respond to therapy. MR Imaging Parameters The type of MR sequence applied greatly affects the MR image. Multiple sequences have been proposed for use in identifying focal or diffuse disease of the bone marrow. These sequences include spin-echo (T1-weighted and T2-weighted), Multiple Myeloma 䡠 15 Radiology Figure 6. MR imaging patterns in MM. Multiple midline sagittal MR images of thoracic or lumbar spine. (a– c) Left: T1-weighted spinecho images (400/15). Middle: STIR images (2,000/150/20). Right: Gadolinium-enhanced fat-suppressed T1-weighted spin-echo images (500/15). (a) Normal MR pattern in lumbar spine. Note primarily fatty marrow (normal MR pattern) with diffuse hyperintensity on T1-weighted spin-echo image, diffuse hypointensity on STIR image, and no marrow enhancement on gadolinium-enhanced image. Note homogeneity of marrow signal intensity for all imaging sequences. (b) Diffuse marrow involvement in lumbar spine. Note primarily cellular marrow demonstrating reversal of normal MR pattern, with diffuse hypointensity on T1-weighted spin-echo image, diffuse hyperintensity on STIR image, and marked enhancement on gadolinium-enhanced image. There is associated fracture of the T12 vertebral body. (c) Diffuse heterogeneous marrow involvement in lumbar spine. Note heterogeneity of marrow signal intensity through all observed vertebral bodies, with mixed areas of hypointensity and hyperintensity on T1-weighted spin-echo, STIR, and gadolinium-enhanced images. Note reversal of signal intensity on T1-weighted and STIR images (Fig 6 continues). gradient-echo (T2*-weighted), STIR, and contrast material–enhanced spin-echo (with and without fat suppression) sequences (26,29,65–67). T1-weighted spin-echo images generally depict a focal plasmacytoma as a hypointense area within a generally hyperintense marrow background. On the other hand, diffuse involvement is identified as generalized hypointensity of the overall marrow, compared with the intensity of the disk interspace or adjacent skeletal muscles. On T2-weighted spin-echo, gradientecho, and STIR images, focal lesions are hyperintense relative to the hypointense marrow background. Diffuse involvement is identified as a generalized hyperintensity of the marrow background relative to the intensity of skeletal muscles. With these sequences, we believe that inclusion of a fat-suppression technique (in our experience, STIR imaging) is important, as it allows better assessment of marrow involvement (diffuse, focal, speckled) and characterization of involvement (uniform or homogeneous, nonuniform or inhomogeneous) (65– 68). Contrast-enhanced studies with fat suppression can supplement these other studies with demonstration of enhancement in focal or diffuse disease. At initial evaluation and follow-up in MM patients, we obtain survey MR images of the entire axial skeleton. These consist of T1-weighted spin-echo and STIR spinecho sequences (sagittal projection of 16 䡠 Radiology 䡠 April 2004 Angtuaco et al MR Imaging of Normal Marrow Radiology In MR imaging evaluation of the marrow, the patient’s age must be taken into consideration. In the young patient, most of the marrow in both the axial and appendicular skeletons is cellular, primarily inhabited by hematopoietic cells (red marrow). In adolescence, the red marrow of the appendicular skeleton changes to yellow marrow, with change occurring initially in the diaphysis and epiphyses and later in the metaphyses. By the age of 20 years, the appendicular skeleton is mostly made of fatty elements, while the axial skeleton—the spine, pelvis, ribs, skull, and proximal metaphyses of the femur and humerus— is largely hematopoietic (69). In the 4th decade of life, the axial skeleton changes in cellular makeup to fatty marrow; by the 6th decade, the marrow is mainly fatty. On T1-weighted images, fatty marrow is hyperintense and cellular marrow is hypointense, relative to the intensity of skeletal muscles. Ricci et al (70) described four normal marrow patterns in various age groups (Table 2). In the age population where MM is most often found, one should be cautious in identifying diffuse nonuniform or bandlike areas of hypointensity on T1weighted images as abnormal, because these findings can be normal in this age group. MR Imaging of MM Figure 6 (continued). MR imaging patterns in MM. (d, e) Left: T1-weighted spin-echo images (400/15). Middle: STIR images (2,000/150/20). Right: Gadolinium-enhanced fat-suppressed T1weighted spin-echo images (500/15). (d) Diffuse speckled marrow involvement in thoracic spine. Note nodular abnormalities in entire spine are better seen on STIR and gadolinium-enhanced images. Speckled, or salt-and-pepper, appearance is better appreciated on STIR and gadoliniumenhanced images, again with posterior-element lesions better seen on these images. (e) Focal disease in thoracic spine. Note several focal lesions at T3 and T4 spinous processes and T12 vertebral body. The smaller spinous process lesions at T4 (arrows) can be seen only on STIR and gadolinium-enhanced images. spine and coronal projection of pelvis). These studies are complementary in the analysis and detection of focal and diffuse disease in MM (65– 68). Gadolinium-enhanced fat-suppressed T1-weighted images are added to studies of the thoracic and lumbar spine. This allows better differentiation of smaller focal lesions and characterization of diffuse disease. Transverse T1Volume 231 䡠 Number 1 and/or T2-weighted images are obtained to characterize the effects of focal expansile lesions. MR imaging of the brain is performed to examine diploic involvement of the calvarium and skull base (Fig 5). This is accomplished with sagittal T1-weighted and coronal and transverse gadolinium-enhanced fat-suppressed T1-weighted sequences. In MM, localization of tumor spread by using MR imaging closely mimics the findings in patients with spinal marrow metastasis. In general, abnormalities are identified as hypointensities on T1weighted images, hyperintensities on STIR images, and enhancement on gadolinium-enhanced images. These imaging features are not pathognomonic for MM and may also be seen in other diseases that affect the marrow. In general, however, MM is suspected whenever MR images depict an expansile focal mass; multiple focal masses in the axial skeleton; diffuse marrow involvement, particularly at known sites of normal hematopoiesis; or multiple compression fractures in a patient with no known primary malignancy. In patients with newly diagnosed MM, several MR patterns have been described that define tumor burden (25,28,30, 71,72) (Fig 6). Low tumor burden is normally associated with a normal MR pattern. On the other hand, high tumor burden is suspected when marrow is diffusely hypointense on T1-weighted imMultiple Myeloma 䡠 17 Radiology ages, hyperintense on STIR images, and enhancing on gadolinium-enhanced images. Overall marrow signal intensity may be homogeneous or heterogeneous. Findings of diffuse marrow involvement may also be appreciated in a setting of increased hematopoiesis in patients with severe anemia or in states of marrow repopulation, which are usually drug induced (stimulation with growth factors). Moulopoulos and Dimopoulos (26) described a variegated marrow appearance on T1-weighted images, suggestive of scattered focal nodular deposits of plasma cells. Plasmacytomas are usually multiple and highly variable in distribution, with the majority located in the thoracic and lumbar spine and the pelvis. They range from small to large expansile focal masses. Focal lesions with diffuse marrow involvement may coexist (25) (Fig 7). In patients with stage I MM, who are usually asymptomatic, MR images commonly show a normal MR pattern (no evidence of diffuse or focal disease). A defined group of patients were, however, identified who had abnormal MR studies. This group showed a more progressive disease pattern with a shorter latency period before the need for systemic chemotherapy (73–76). In newly diagnosed stage III disease, various MR patterns have been demonstrated (25,29,34,77). Lecouvet et al (77) found that 24% of patients had a normal MR pattern. This group of patients responded better to therapy and achieved complete remission more often than did those with diffuse disease. On the other hand, MR images revealing diffuse involvement were shown to correlate with increased marrow cellularity, increased plasmacytosis, anemia, and overall poorer survival when compared with images in patients with a normal MR pattern (25,27,28,30,71,77). MR images accurately reflect response to treatment by showing a decrease or resolution of focal lesions seen on initial studies. Resolution of diffuse disease can also be identified (78 – 80). In a group of 90 patients studied at our institution with survey MR imaging of the axial skeleton before and after high-dose therapy and tandem bone marrow transplantation, the posttreatment MR images showed improvement in successfully treated patients. Complete resolution of MR findings to a normal MR pattern without focal lesions, which was achieved in 40 patients, was associated with an improved patient survival of 65 months or longer versus 46 months in those without 18 䡠 Radiology 䡠 April 2004 TABLE 2 Patterns of Normal Signal Intensity on T1-weighted MR Images of Spine in Different Age Groups Pattern and Site Age Distribution 1: Hypointense Cervical Thoracic Lumbar 2: Hypointense with bandlike and triangular hyperintensity at endplates Cervical Thoracic Lumbar 3: Hyperintense* Cervical Thoracic Lumbar 92% ⬍40 y 70% ⬍30 y 99% ⬍30 y 87% ⬎40 y 88% ⬎50 y 86% ⬎40 y 75% ⬎50 y Uniform 76% ⬎40 y * Pattern 3a is homogeneous; pattern 3b is heterogeneous. Figure 7. Diffuse disease with multifocal lesions. Noncontiguous coronal STIR MR images (2,000/150/20) demonstrate diffuse overall hyperintensity of marrow as compared with signal intensity of adjacent muscles. Focal lesions involving right posterior ilium (curved arrow), right and left ischium (arrowheads), and L4 and L5 vertebral bodies with extraosseous mass at right side of L5 (straight arrows) are noted against background of hyperintense marrow. complete resolution of MR findings (81) (Fig 8). FRACTURE IN MM Spinal compression fractures occur in 55%–70% of patients with MM (82) (Figs 2, 9). These fractures may be due to bone destruction by a focal mass or to increased osteolysis. MR imaging provides an opportunity to detect the offending cause (83,84). Lecouvet et al (82) classified spinal fractures into benign or malignant, primarily on the basis of the presence of an associated focal mass. Sixtyseven percent of 224 total fractures in 37 patients were identified as benign. In our review of MR imaging surveys of the entire spine in 264 patients with newly diagnosed MM (84), fractures were present in 117 (44.3%). A single fracture was seen in 50 (42%) of 117 patients, and a focal lesion causing the fracture was seen in 40 (80%) of those 50 patients. In patients with multiple fractures, 273 sites of fracture were seen in 67 (58%) patients; of the 273 fractures, 126 (46%) had an associated mass. These results indicate that spinal fractures in MM do not require the presence of a focal mass and can occur in a setting of marrow that appears benign on MR images (82– 84). Tricot (21) proved this point in laboratory studies that showed that the presence of myAngtuaco et al Radiology Figure 9. Plasmacytoma with associated compression fracture of C7. Sagittal T1-weighted (left; 600/15) and STIR (right; 2,000/150/20) MR images of cervical spine show focal lesion (arrows) involving C7 vertebral body, with associated fracture. There is protrusion of the plasmacytoma into adjacent spinal canal. Figure 8. Complete resolution of diffuse and focal lesions. Left: Pretreatment sagittal (top) and coronal (bottom) STIR MR images (2,000/150/20) of lumbar spine and pelvis show diffuse disease with focal lesions (straight arrows) in pelvis. Right: Follow-up sagittal (top) and coronal (bottom) STIR MR images (2,000/150/20) of lumbar spine and pelvis show complete resolution of both diffuse and focal lesions. Note normal MR appearance of diffuse hypointensity without focal lesions. Superior end-plate fracture at L4 (curved arrow) has developed. eloma cells in bone marrow stroma increases the formation of osteoclast-activating factors, leading to increased bone resorption and subsequent fractures. Spinal fractures also occur following treatment. Moulopoulos et al (79) reported 35 new sites of fracture in 29 successfully treated MM patients. In patients with relapse, fractures were also noted. In another study, Lecouvet et al (85) showed 131 new fractures in 37 patients undergoing therapy. They found that the group of patients with an initial MR study showing diffuse disease or more than 10 focal lesions had a shorter fracture-free interval than did the patients who did not have diffuse disease shown on MR images. They suggested that the initial MR study may help identify patients at increased risk for subsequent fracture of the spine. Currently, bisphosphonates are standard drugs administered to MM patients undergoing therapy, because these drugs are known to decrease the incidence of compression fractures. Bisphosphonates disrupt the vicious cycle of increased osteolysis and myeloma cell production. Volume 231 䡠 Number 1 New treatment methods for spinal fractures related to MM include percutaneous vertebroplasty and kyphoplasty. Percutaneous vertebroplasty is now accepted as a method of alleviating the bone pain associated with a spinal fracture (86). The procedure also has the secondary aim of preservation of the remaining height of the vertebral body. Kyphoplasty, on the other hand, aims at restoration of the original vertebral height and elimination of spinal deformity (87). MR findings of abnormal signal intensity in spinal fractures aid the interventionalist in determining the treatment level in cases of multiple spinal fractures. Parallel zones of hypointensity on T1-weighted images and hyperintensity on STIR or T2weighted images in the fractured vertebra correlated with localized pain during percussion at the site of fracture. COMPLICATIONS AND PROGRESSION OF DISEASE The multiple drug therapies currently utilized in the treatment of MM result in com- plications that are identifiable on MR images. High doses of corticosteroids, a frontline drug in treatment of MM, may cause spinal fracture and avascular necrosis of the femoral heads. Immunosuppression caused by cytotoxic drugs results in a higher incidence of infections in the spine (eg, discitis) and the brain (eg, cerebritis, cerebral abscess). Cyclosporine used in marrow transplantation regimens may result in neurologic changes of posterior reversible cerebral encephalopathy. A rare progression in MM is leptomeningeal spread within the central nervous system. In a recent review of 1,856 treated patients at our institution, Fassas et al (88) showed this complication in 18 patients. MR findings of leptomeningeal enhancement in the brain or spine were seen and helped establish the diagnosis (Fig 10). The definitive diagnosis was made with results from cytologic analysis of cerebrospinal fluid. This complication was associated with unfavorable cytogenetic results such as chromosome 13 deletion, histologic findings of plasmablastic cells, other extramedullary sites of disease, and plasma cell leukemia. Myelofibrosis and amyloidosis can develop as a consequence of treatment in patients with MM. Myelofibrosis can be suggested on MR studies as a conversion of the entire bone marrow to diffuse hypointensity on both T1-weighted and STIR images. Amyloidosis can be seen as focal areas of hypointensity on both T1weighted and STIR images. Relapse and poor response to treatment are well evaluated with MR imaging. In patients with clinical relapse, new focal lesions or an increase in the size of previously identified focal lesions in Multiple Myeloma 䡠 19 Radiology medullary or extramedullary sites are seen (Fig 11). In severe relapse, conversion of a normal pattern to one of diffuse involvement may also be seen. Poor response to treatment protocols also can be demonstrated on follow-up MR studies, where they appear as no change or deterioration in the previously identified areas of involvement. MGUS AND SOLITARY BONE PLASMACYTOMA Monoclonal gammopathy of uncertain significance (MGUS) is the most common cause of laboratory-discovered monoclonal gammopathy. MGUS is usually an incidental finding, and its incidence in patients over the age of 70 years is 3% (89). The serum M protein component is typically low, Bence-Jones proteinuria is rare, and there is less than 10% plasmacytosis in the marrow. M protein levels remain relatively stable over time. Although most patients die of comorbid conditions, MGUS can “evolve” to MM, Waldenström macroglobulinemia, chronic lymphocytic leukemia, plasmacytoma, amyloidosis, or lymphoma. The longer the follow-up, the higher the percentage of patients whose condition eventually progresses to malignant disease. In a recent study of almost 1,400 patients with MGUS and with 11,000 person-years of follow-up, the cumulative probability of progression was 12% at 10 years, 25% at 20 years, and 30% at 25 years (90). Initial monoclonal protein (M protein) concentration was a significant predictor of progression at 20 years. Vande Berg et al (91) performed MR imaging in 35 patients with MGUS and found MR abnormalities in seven. Of the patients with no MR abnormalities, none required treatment after a follow-up of 30 months. On the other hand, four of seven patients with abnormal MR findings required treatment within 5 years of diagnosis. MR imaging provides important information concerning prognosis in patients with MGUS, and an abnormal MR study warrants closer follow-up for signs of progressive disease. Solitary bone plasmacytoma is uncommon (representing 2%–3% of plasma cell dyscrasias) and usually manifests with bone pain. The diagnosis is based on histologic evidence of tumor consisting of monoclonal plasma cells. Associated laboratory findings include normal blood levels of hemoglobin, creatinine, and calcium, with negative bone marrow biopsy results and skeletal radiographic survey findings. 20 䡠 Radiology 䡠 April 2004 Figure 10. Leptomeningeal spread in MM. Contrast-enhanced sagittal (left) and transverse (right) T1-weighted spin-echo (450/15) MR images of lumbar spine show abnormal enhancement of nerve roots (arrowhead) and surface of conus medullaris (arrow). Transverse image shows distinct nodular enhancement of the cauda equina, indicative of leptomeningeal spread of tumor. Figure 11. Extramedullary spread in MM. Left: Transverse T2weighted spin-echo MR image (2,000/80) in a patient with clinical findings of relapse show a mass (curved arrow) in the left pararenal space. A separate mass (straight arrow) is in the right pararenal space. Right: On transverse T2-weighted (2,000/80) section obtained at a lower level, right pararenal mass is shown extending into adjacent right neural foramen and epidural space (arrowhead). Associated dural sac compression is noted. Biopsy of both masses revealed malignant plasma cells. A small, if any, M protein component should decrease with treatment (definitive local radiation therapy) (92). The rate of reduction of M protein level may be slow (93), and in many patients the M protein persists for years despite adequate radiation therapy, implying the presence of tumor cells beyond the radiation field. The median overall survival after radiation therapy in patients with solitary bone plasmacytoma is 10 years. The median time to progression to MM is 2–3 years. In some studies, the size of the lesion, osteopenia, and low levels of uninvolved immunoglobulins were predictive of progression to overt MM (94). Results of several studies indicated that screening of patients with solitary bone plasmacytoma by using MR imaging or in combination with a skeletal radiographic survey revealed a high prevalence of other plasmacytomas. This group of patients also showed a shorter latency of progression to MM (95–97). Angtuaco et al CONCLUSION Radiology In the past decade, important advances in the understanding of MM and the therapeutic options available to patients with the disease have resulted in improved patient survival. This has gone hand in hand with the advanced capabilities of modern imaging methods, particularly MR. MR imaging bone marrow surveys in patients with MM demonstrate the broad spectrum of involvement, the results of treatment, the areas of potential complications, and the sites of focal disease for safe bone biopsies. Figure 12. MR-directed CT-assisted biopsy. Left: Sagittal contrastenhanced fat-suppressed T1-weighted spin-echo (600/15) MR image shows two enhancing lesions at T3 (arrow) and T9 (arrowhead). Right: Transverse CT image obtained with patient in prone position during CT-assisted biopsy of the T9 lesion shows biopsy needle (arrow) entering the lytic lesion of T9 vertebral body by using a transpedicular approach. MR-DIRECTED CT-ASSISTED SKELETAL BIOPSY PERSPECTIVES IN THE TREATMENT OF MM Cytogenetic abnormalities (in particular, chromosome 13 deletion) in the plasma cells in patients with MM is an important negative predictor of durable clinical response and overall survival (17). Obtaining proper biopsy specimens of the tumor that can lead to this discovery has become a necessary clinical tool. MR survey studies that depict unsuspected sites of focal lesions help direct this process of specimen collection (Fig 12). Bone biopsies with largebore needles (generally 12–14-gauge bone biopsy needles) are difficult to perform in the MR setting. CT guidance of these MR-depicted focal lesions has aided the safe performance of these procedures, especially in spinal bone biopsies. Our experience with biopsies of the spine and pelvis of MR-depicted focal lesions has led to a 20% increase in the yield of positive cytologic and cytogenetic information from biopsies at these sites, compared with results in samples obtained from random iliac crest biopsies (37). This had led to a more aggressive clinical approach once cytogenetic abnormalities are detected. The treatment of patients with MM continues to evolve. In a recent review of current treatment options in patients with MM, one of the authors (B.B.) indicated the superiority of high-dose therapy over conventional therapy in terms of event-free survival and overall survival (98). The rate of complete remission improved from 5% to 50%, with event-free survival extending beyond 3 years and overall survival beyond 6 years. The author stressed the importance of the detection of cytogenetic abnormalities, particularly chromosome 13 deletion, in cytologic specimens as indicative of a poor outcome. His review showed favorable outcomes in patients without the cytogenetic abnormality and with low -2 microglobulin and C-reactive protein levels. Improved outcomes were achieved with the addition of thalidomide, owing to the antiangiogenic activity of that drug. Finally, good outcomes were seen in the group of patients who achieved complete clinical remission shown on follow-up MR studies with a normal MR pattern without focal lesions (81). These patients had a better overall survival rate and prolonged event-free survival than did those with persistent lesions on MR images. Volume 231 䡠 Number 1 References 1. Blade J, Kyle RA, Greipp PR. Multiple myeloma in patients younger than 30 years: report of 10 cases and review of the literature. Arch Intern Med 1996; 156:1463– 1468. 2. Hallek M, Bergsagel PF. Anderson KC. Multiple myeloma: increasing evidence for a multistep transformation process. Blood 1998; 91:3–21. 3. Klein B, Bataille R. Cytokine network in human multiple myeloma. Hematol Oncol Clin North Am 1992; 6:273–284. 4. Niesvizky R, Warrell RP. Pathophysiology and management of bone disease in multiple myeloma. Cancer Invest 1997; 15: 85–90. 5. Buxbaum J. Mechanisms of disease: monoclonal immunoglobulin deposition—amyloidosis, light chain deposition disease, and light and heavy chain deposition disease. Hematol Oncol Clin North Am 1992; 6:323–346. 6. Kyle RA. Multiple myeloma and other plasma cell disorders. In: Hoffman R, ed. Hematology: basic principles and practice. 2nd ed. New York: Churchill Livingstone, 1995; 1354. 7. Kyle R. Diagnostic criteria of multiple myeloma. Hematol Oncol Clin North Am 1992; 6:347–358. 8. Durie BG, Salmon SE. A clinical staging system for multiple myeloma: correlation of measured myeloma cell mass with presenting clinical features, response to treatment and survival. Cancer 1975; 36:842– 854. 9. Barlogie B, Epstein J, Selvanayagam P, Alexanian R. Plasma cell myeloma: new biological insights and advances in therapy. Blood 1989; 73:865– 879. 10. Durie BG, Stock-Novack D, Salmon SE, et al. Prognostic value of pretreatment serum beta 2 microglobulin in myeloma: a Southwest Oncology Group study. Blood 1990; 75:823– 830. 11. Bataille R, Boccadora M, Klein B, et al. C-reactive protein and beta 2 microglobulin produce a simple and powerful myeloma staging system. Blood 1992; 80: 733–737. 12. Drewinko B, Alexanian R, Boyer H, et al. The growth factor of human myeloma cells. Blood 1981; 57:333–338. 13. Greipp PR, Lust JA, O’Fallon WM, et al. Plasma cell labeling index and beta 2 microglobulin predict survival independent of thymidine kinase and C-reactive protein in multiple myeloma. Blood 1993; 81:3382–3387. Multiple Myeloma 䡠 21 14. Dimopoulos MA, Barlogie B, Smith TL, Alexanian R. High serum lactate dehydrogenase level as a marker for drug resistance and short survival in multiple myeloma. Ann Intern Med 1991; 115:931–935. Sawyer JR, Waldron JA, Jagannath S, Barlogie B. Cytogenetic findings in 200 patients with multiple myeloma. Cancer Genet Cytogenet 1995; 82:41– 49. Tricot G, Sawyer JR, Jagannath S, et al. Unique role of cytogenetics in the prognosis of patients with myeloma receiving high-dose therapy and auto-transplants. J Clin Oncol 1997; 15:2659 –2666. Tricot G, Barlogie B, Jagannath S, et al. Poor prognosis in multiple myeloma is associated only with partial or complete deletions of chromosome 13 or abnormalities involving 11q and not with other karyotype abnormalities. Blood 1995; 86:4250 – 4256. Jantunen E, Laakso M. Biophosphonates in multiple myeloma: current status; future perspectives. Br J Haematol 1996; 93: 501–506. Roodman GD. Cell biology of the osteoclast. Exp Hematol 1999; 27:1229 –1241. Lacey DL, Timms E, Tan HL, et al. Osteoprotegerin ligand is a cytokine that regulates osteoclast differentiation and activation. Cell 1998; 93:165–176. Tricot G. New insights into role of microenviroment in multiple myeloma. Lancet 2000; 355:248 –249. Berenson JR, Lichtenstein A, Porter L, et al. Efficacy of pamidronate in reducing skeletal events in patients with advanced multiple myeloma. Myeloma Aredia Group. N Engl J Med 1996; 334:488 – 493. Aparicio A, Gardner A, Tu Y, Savage A, et al. In vitro cytoreductive effects on multiple myeloma cells induced by bisphosphonates. Leukemia 1998; 12:220 –229. Berenson JR, Lichtenstein A, Porter L, et al. Long-term pamidronate treatment of advanced multiple myeloma patients reduces skeletal events. Myeloma Aredia Study Group. J Clin Oncol 1998; 16:593– 602. Angtuaco EJ, Moulopoulos LA, Hronas T, Avva R. Imaging studies. In: Mehta J, Singhal S, eds. Myeloma. London, England: Dunitz, 2002; 297–309. Moulopoulos L, Dimopoulos M. Magnetic resonance imaging of the bone marrow in hematologic malignancies. Blood 1997; 90:2127–2147. Dimopoulos M, Moulopoulos L, Datseris I, et al. Imaging of myeloma bone disease. Acta Oncol 2000; 39:823– 827. Lecouvet F, Vande Berg B, Malghem J, Maldague B. Magnetic resonance imaging in multiple myeloma. Semin Musculoskelet Radiol 2001; 5:43–55. Vande Berg B, Lecouvet F, Michaux L, et al. Magnetic resonance imaging of the bone marrow in hematological malignancies. Eur Radiol 1998; 8:1335–1344. Kusumoto S, Jinnai I, Itoh K, et al. Magnetic resonance imaging patterns in patients with multiple myeloma. Br J Haematol 1997; 99:649 – 655. Schirrmeister H, Bommer M, Buck AK, et al. Initial results in the assessment of multiple myeloma using F-18 FDG PET. Eur J Nucl Med Mol Imaging 2002; 29: 361–366. Greenspan A. Malignant bone tumors II. Radiology 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 22 䡠 Radiology 䡠 April 2004 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. In: Greenspan A, ed. Orthopedic radiology: a practical approach. 3rd ed. Philadelphia, Pa: Lippincott Williams & Wilkins, 2000; 697–700. Lecouvet FE, Malghem J, Michaux L, et al. Skeletal survey in advanced multiple myeloma: radiographic versus magnetic resonance imaging survey. Br J Haematol 1999; 106:35–39. Hubner KF, Andrews GA, Hayes RL, Poggenburg JK, Solomon A. The use of rare-earth radionuclides and other boneseekers in the evaluation of bone lesions in patients with multiple myeloma or solitary plasmacytoma. Radiology 1977; 125:171–176. Wahner HW, Kyle RA, Beabout JW. Scintigraphic evaluation of the skeleton in multiple myeloma. Mayo Clin Proc 1980; 55:739 –746. Mahnken AH, Wildberger JE, Gehbauer G, et al. Multidetector CT of the spine in multiple myeloma: comparison with MR imaging and radiography. AJR Am J Roentgenol 2002; 178:1429 –1436. Avva R, Vanhemert R, Barlogie B, et al. CT-guided biopsy of focal lesions in patients with multiple myeloma may reveal new and more aggressive cytogenetic abnormalities. AJNR Am J Neuroradiol 2001; 22:781–785. Scutellari PN, Spanedda R, Feggi LM, Cervi PM. The value and limitations of total body scan in the diagnosis of multiple myeloma: a comparison with conventional skeletal radiography. Haematologica 1985; 70:136 –142. Woolfenden JM, Pitt MJ, Durie BGM, Moon TE. Comparison of bone scintigraphy and radiology in multiple myeloma. Radiology 1980; 134:723–728. Ampil FL, Mills GM. Bone scintigraphy in plasma cell myeloma. Eur J Orthop Surg Traumatol 1999; 9:59 – 60. Shuke N, Okizaki A, Yamamoto W, Usui K, Aburano T. Accumulation of Tc-99m HMDP in extramedullary plasmacytoma of the stomach. Clin Nucl Med 2001; 26: 354 –355. VanAntwerp JD, O’Mara R, Pitt M, Walsh S. Technetium-99m-diphosphonate accumulation in amyloid. J Nucl Med 1975; 16:238 –240. Kanoh T, Ohno T, Uehino H, Amamoto I, Torizuka K. Avid uptake of 67-Ga in multiple myeloma. An additional indicator of the aggressive phase. Clin Nucl Med 1987; 12:482– 484. Roach PJ, Arthur CK. Comparison of thallium-201 and gallium-67 scintigraphy in soft tissue and bone marrow multiple myeloma: a case report. Australas Radiol 1997; 41:67– 69. De Rosa G, Pezzulo L, Del Vecchio S. Avid (67)Ga uptake in multiple myeloma relapsing after bone marrow transplant. Haematologica 2000; 85:764. Lin WY, Wang SJ. Ga-67 scan findings in bone marrow involvement with plasmablastic myeloma and corresponding Tc99m MIBI images. Clin Nucl Med 2001; 26:963. Ishibashi M, Nonoshita M, Uchida M, et al. Bone marrow uptake of thallium-201 before and after therapy in multiple myeloma. J Nucl Med 1998; 39:473– 475. Watanabe N, Shimizu M, Kageyama M, et al. Multiple myeloma evaluated with 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 201Tl scintigraphy compared with bone scintigraphy. J Nucl Med 1999; 40:1138 – 1142. Tirovola EB, Biassoni L, Britton KE, Kaleva N, Kouykin V, Malpas JS. The use of 99m-Tc-MIBI scanning in multiple myeloma. Br J Cancer 1996; 74:1815–1820. Pace L, Catalano L, Pinto A, et al. Different patterns of technetium-99m sestamibi uptake in multiple myeloma. Eur J Nucl Med 1998; 25:714 –720. Fonti R, Del Vecchio S, Zannetti A, et al. Bone marrow uptake of 99m-Tc-MIBI in patients with multiple myeloma. Eur J Nucl Med 2001; 28:214 –220. Piwnica-Worms D, Holman L. Noncardiac applications of hexakis(alkylisonitril) 99m-Tc complexes. J Nucl Med 1990; 31:1166 –1167. Chiu ML, Kronauge JF, Piwnica-Worms D, et al. Effect of mitrochondrial and plasma membrane potentials on accumulation of hexakis(2-methoxyisobutylisonitril) technetium in cultured mouse fibroblast. J Nucl Med 1990; 31:1646 –1653. Piwnica-Worms D, Chiu ML, Budding M, Kronauge JF, Kramer RA, Croop JM. Functional imaging of multidrug resistant pglycoprotein with an organotechnetium complex. Cancer Res 1993; 53:977–984. Piwnica-Worms D, Rao VV, Kronauge JF, Croop JM. Characterization of multidrug resistance P-glycoprotein transport function with an organotechnetium cation. Biochemistry 1995; 34:12210 –12220. Moretti JL, Cordobes MD, Starzec A, et al. Involvement of glutathione in loss of technetium-99m-MIBI accumulation related to membrane MDR protein expression in tumor cells. J Nucl Med 1998; 39:1214 –1218. Vecchio SD, Ciarmiello A, Potena MI, et al. In vivo detection of multidrug-resistant (MDR1) phenotype by 99m-Tc-sestamibi scan in untreated breast cancer patients. Eur J Nucl Med 1997; 24:150 –159. Sasaki M, Ichiya Y, Kuwabara Y, et al. Fluorine-18-fluorodeoxyglucose positron emission tomography in technetium99m-hydroxymethylenediphosphate negative bone tumors. J Nucl Med 1993; 34:288 –290. El-Shirbiny AM, Yeung H, Imbriaco M, Michaeli J, Macapinlac H, Larson SM. Technetium-99m-MIBI versus fluorine18-FDG in diffuse multiple myeloma. J Nucl Med 1997; 38:1208 –1210. Edwards GK, Santoro J, Taylor A Jr. Use of bone scintigraphy to select patients with multiple myeloma for treatment with strontium-89. J Nucl Med 1994; 35:1992– 1993. Lecouvet F, Richard F, Vande Berg B, et al. Long term effects of localized spinal radiation therapy on vertebral fractures and focal lesions appearance in patients with multiple myeloma. Br J Haematol 1997; 96:743–745. Walker RE, Eustace SJ. Whole-body magnetic resonance imaging: techniques, clinical indications, and future applications. Semin Musculoskelet Radiol 2001; 5:5–19. Vogler JB, Murphy WA. Bone marrow imaging. Radiology 1988; 168:679 – 693. Weinreb JC. MR imaging of bone marrow. Radiology 1990; 177:23–24. Rahmouni A, Divine M, Mathieu D, et al. Angtuaco et al Radiology 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. Detection of multiple myeloma involving the spine: efficacy of fat-suppression and contrast-enhanced MR imaging. AJR Am J Roentgenol 1993; 160:1049 –1052. Golfieri R, Baddely H, Pringle J, et al. The role of the STIR sequence in magnetic resonance imaging examination of bone tumours. Br J Radiol 1990; 63:251–256. Mirowitz SA, Apicella P, Reims WR, et al. MR imaging of bone marrow lesions: relative conspicuousness on T1-weighted, fat-suppressed T2-weighted and STIR images. AJR Am J Roentgenol 1994; 162: 215–221. Angtuaco EJ, Robbins MB, Angtuaco EE, et al. Prospective analysis of STIR and fatsuppressed fast spin echo imaging in the evaluation of bone marrow disorders (abstr). Radiology 1992; 185(P):195. Moore SG, Dawson KL. Red and yellow marrow in the femur: age-related changes in appearance at MR imaging. Radiology 1990; 175:219 –223. Ricci C, Cova M, Kang Y, et al. Normal age-related patterns of cellular and fatty bone marrow distribution in the axial skeleton: MR imaging study. Radiology 1990; 177:83– 88. Moulopoulos LA, Varma DG, Dimopoulos MA. Multiple myeloma: spinal MR imaging in patients with untreated newly diagnosed disease. Radiology 1992; 185: 833– 840. Tertti R, Alanen A, Remes K. The value of magnetic resonance imaging in screening myeloma lesions of the lumbar spine. Br J Haematol 1995; 91:658 – 660. Dimopoulos MA, Moulopoulos LA, Smith TL, et al. Risk of disease progression in asymptomatic multiple myeloma. Am J Med 1993; 94:57– 61. Weber DM, Dimopoulos MA, Moulopoulos LA, et al. Prognostic features of asymptomatic multiple myeloma. Br J Haematol 1997; 97:810 – 814. Van de Berg BC, Lecouvet FE, Michaux L, et al. Stage I multiple myeloma: value of MR imaging of the bone marrow in the determination of prognosis. Radiology 1996; 201:243–246. Moulopoulos LA, Dimopoulos MA, Smith TL, et al. Prognostic significance of magnetic resonance imaging in patients with Volume 231 䡠 Number 1 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. asymptomatic multiple myeloma. J Clin Oncol 1995; 13:251–256. Lecouvet FE, Vande Berg B, Michaux L. Stage III myeloma: clinical and prognostic value of spinal bone marrow MR imaging. Radiology 1998; 209:653– 660. Rahmouni A, Divine M, Mathieu D, et al. MR appearance of multiple myeloma before and after treatment. AJR Am J Roentgenol 1993; 160:1053–1057. Moulopoulos LA, Dimopoulos MA, Alexanian R, et al. Multiple myeloma: MR patterns of response to treatment. Radiology 1994; 193:441– 446. Lecouvet FE, Dechambre S, Malghem J, et al. Bone marrow transplantation in patients with multiple myeloma: prognostic significance of MR imaging. AJR Am J Roentgenol 2001; 176:91–96. Angtuaco EJ, Avva R, Munshi CN, et al. MR skeletal survey of the axial skeleton: a predictor of patient survival in multiple myeloma? (abstr). Radiology 1999; 213(P):294. Lecouvet FE, Vande Berg BC, Maldague BE, et al. Vertebral compression fractures in multiple myeloma. I. Distribution and appearance at MR imaging. Radiology 1997; 204:195–199. Moulopoulos LA, Yoshimitsu K, Johnston DA, et al. MR prediction of benign and malignant vertebral compression fractures. J Magn Reson Imaging 1996; 6:667– 674. Angtuaco EJ, Justus M, Sethi R, et al. Analysis of compression fractures in patients with newly diagnosed multiple myeloma on comprehensive therapy (abstr). Radiology 2001; 221(P):138. Lecouvet FE, Malghem J, Michaux L, et al. Vertebral compression fractures in multiple myeloma. II. Assessment of fracture risk with MR imaging of spinal bone marrow. Radiology 1997; 204:201–205. Cotten A, Dewatre F, Cortet B, et al. Percutaneous vertebroplasty for osteolytic metastases and myeloma: effect of the percentage of lesion filling and the leakage of methacrylate at clinical follow-up. Radiology 1996; 200:525–530. Theodorou DJ, Theodorou SJ, Duncan TD, et al. Percutaneous kyphoplasty for the correction of spinal deformity in 88. 89. 90. 91. 92. 93. 94. 95. 96. 97. 98. painful vertebral body compression fractures. Clin Imaging 2002; 26:1–5. Fassas A, Muwalla F, Berryman T, et al. Myeloma of the central nervous system: association with high-risk chromosomal abnormalities, plasmablastic morphology and extramedullary manifestations. Br J Haematol 2002; 117:103–108. Kyle RA. Monoclonal gammopathy of undetermined significance and solitary plasmacytoma: implications for progression to overt multiple myeloma. Hematol Oncol Clin North Am 1997; 11:71– 87. Kyle RA, Therneau TM, Rajkumar SV, et al. A long term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med 2002; 346:564 –569. Vande Berg BC, Lecouvet FE, Michaux L, et al. Nonmyelomatous monoclonal gammopathy: correlation of bone marrow MR images with laboratory findings and spontaneous clinical outcome. Radiology 1997; 202:247–251. Dimopoulos MA, Moulopoulos LA, Maniatis A, Alexanian R. Solitary plasmacytoma of bone and asymptomatic multiple myeloma. Blood 2000; 96:2037–2044. Alexanian R. Localized and indolent myeloma. Blood 1980; 56:521–525. Jackson A, Scarffe JH. Prognostic significance of osteopenia and immunoparesis at presentation in patients with solitary myeloma of bone. Eur J Cancer 1990; 26: 363–371. Moulopoulos LA, Dimopoulos MA, Weber D, et al. Magnetic resonance imaging in the staging of solitary plasmacytoma of bone. J Clin Oncol 1993; 11:1311– 1315. Mathieu D, Rahmouni A, Divine M, et al. MR imaging of the spine in presumed solitary plasmacytoma (abstr). Radiology 1993; 189(P):119. Liebross RH, Ha CS, Cox JD, et al. Solitary bone plasmacytoma: outcome and prognostic factors following radiotherapy. Int J Radiat Oncol Biol Phys 1998; 41:1063–1067. Barlogie B. High-dose therapy and innovative approaches to treatment of multiple myeloma. Semin Hematol 2001; 38: 21–27. Multiple Myeloma 䡠 23