Technical note
advertisement

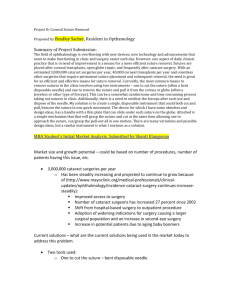
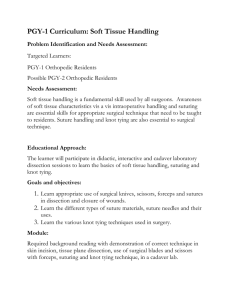
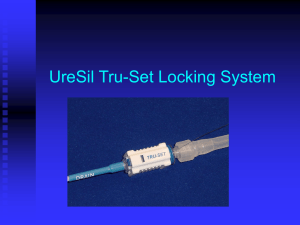
Technical note An investigation of leakage tracts along stressed suture lines in phantom tissue G.A. Thomson a , a, Mechanical Engineering & Mechatronics, University of Dundee, Dundee DD1 4HN, UK Received 25 July 2006; revised 3 October 2006; accepted 10 October 2006. Available online 29 November 2006. Abstract Suturing is still one of the most important procedures used in trauma and surgery environments. It does however rely on piercing other wise healthy tissue. In doing so channels are opened which may act as conduits for bacteria to enter the body or to allow material such as blood or intestinal bacteria to leak from vessels. This work shows by means of finite element analysis and physical modelling through the use of a phantom that the tension in the suture has a direct bearing on the opening of these channels. It was found that for the phantom the channel cross-sectional area was approximately proportional to the applied tension and suture thread deflection. Leakage channels of up to 0.1 mm2 cross-section were achieved with suture tensions of 120 grammes force. Channels of this size are significantly larger than the bacteria suggesting transmission is theoretically possible. Keywords: Suturing; Leakage; Finite element modelling; Colon Article Outline 1. Introduction 2. Methods and models 3. Results and discussion 4. Conclusion Acknowledgements References 1. Introduction Suturing is a very well established technique for connecting sections of tissue following trauma or surgical procedures, with the basic concept reported in Indian texts dating as far back as 1000 B.C. [1], [2] and [3]. Suturing offers relative speed, security and the ability to approximate open tissue. As a result, despite recent developments involving the likes of stapling or adhesive strips, suturing is likely to remain a feature of surgical practice for some time to come. An aspect of suturing that is perhaps less desirable is that, by definition, the suturing needle and the trailing suture must pass through healthy and undamaged tissue proximal to the wound being secured. An implication of this is that this tissue becomes perforated by a series of holes. Creation of the suturing holes is achieved by the suturing needle and these needles are available in a wide variety of lengths, curvatures, suture attachment methods and needle cross-sectional profiles. It is the cross-sectional profiles which largely help define how the needle will penetrate the tissue and broadly speaking these fall into two general types—cutting and tapered (Fig. 1). (17K) Fig. 1. Cutting and tapered suture needles. Cutting needles generally have tapered, triangular cross-sections with the vertices of these forming sharp edges to help shear the tissue. This is designed to make suturing easier particularly when dealing with tougher tissue types such as skin or tendon. Purely tapered needles have a circular cross-section and tend to push between tissue fibres separating rather than cutting through them. In doing so the intention is that the natural elasticity of the tissue should help to close the hole back around the suture following the passage of the needle. This should minimise tissue damage and help to ensure a certain degree of sealing around the suture thread. As a result these needles are particularly favoured for leak critical applications. Leakage around the suture is often an important issue. For surface wounds in the skin or eyes, the suture hole can act as a tract for bacteria to travel deep into the tissue leading to possible infection [4]. For internal surgery the consequences can be potentially even more serious. A very common type of internal surgery is a procedure known as anastomosis which can be applied to a number of conditions. This involves the reconnection of internal plumbing following transplantation, implantation or after the removal of diseased or damaged tissue. This procedure is commonly applied to the vascular system to reconnect veins or arteries following surgery. Leakage here can cause either haemorrhaging of blood out of the vessel or ingress of undesirable material into the blood supply. As a result surgeons will generally have to use a fibrin sealant around the join to help reduce the possibility of leakage [5] and [6]. A further common form of anastomosis relates to the digestive tract, in particular the colon [7], [8], [9] and [10]. Colon cancer is extremely common and generally requires surgical treatment in which the diseased tissue is removed and the resulting free ends of the remaining healthy sections of colon are then joined together. The colon is very rich in bacteria which aid in the digestive process, however if these leak out into abdominal lumen they can cause serious infection in the potentially fatal form of peritonitis [11], [12], [13], [14], [15] and [16]. Leakage of material through suture holes, whether internal or external can therefore have very serious clinical consequences which impact patient health and with the resulting complications, add to health provider demands. This work made use of phantom tissue material and finite element modelling to assess the extent of leakage around the suture lines and will focus on the application of round tapered needles as applied to colon suturing. To date most finite element work carried out on skin suturing has focussed on how the bulk tissue is brought together and the implications this has on healing [17], [18] and [19]. Modelling work on the detail interaction of how the suture passes through tissue appears limited. This work was conducted as part of a larger programme aiming to develop a device to allow surgeons to test intraoperatively for possible suture leakage, both from the suture holes and the tissue join. Clinical data on the exact nature of leakage is very limited as these cases tend to come to light a day or so after a prior surgery and are by definition emergency procedures necessitating rapid clean resection rather than detailed investigation and repair. By physically and numerically modelling the suture hole it is the intention to begin to understand the nature of leakage and so help to identify key criteria which can be used by the surgeon to reduce the likelihood of leakage. 2. Methods and models For the physical trials a sample of phantom tissue was placed on a microscope slide. This phantom material was made from a section of cast Gelflex (Alex Tiranti Ltd., Berkshire, UK), 15 mm2 and 3.5 mm thick. This material has a measured elastic modulus of 150 kPa. Through the centre of this material a suture was passed using its attached needle and the ends of the suture joined together. The suture type chosen was Ethicon W9136 (Ethicon, Livingston, UK) which features a round tapered needle, and a measured thread diameter of 0.35 mm. This is typical of the type used in colon surgery. This thread was then tensioned with varying loads and a microscope used to examine the distortion of the suture hole. An illustration of this can be seen in Fig. 2. Images of the hole distortion were then captured via a camera attached to the microscope and the area of separation was evaluated using standard imaging software. (90K) Fig. 2. Schematic (a) and actual (b) suture tensioning system. The equivalent finite element model was limited to a two-dimensional plane stress structure. This is a simplification of the true situation, however as mechanical property data for the colon, in particular with regard to the third (through thickness) dimension is limited a three-dimensional approach would have generated further simplifications. Fig. 3 shows a schematic of the model. This replicates the phantom sample in taking the form of a square of side length 15 mm and a thickness of 3.5 mm. (33K) Fig. 3. Finite element model of suture passing through tissue. The thread passing through the hole was given a nominal diameter of 0.35 mm commensurate with the actual suture. Compressive radial interference with the surrounding material of 0.025 mm was applied to simulate the elastic reaction from the displaced tissue. The material was fully restrained along its left hand edge to simulate the clamping of this edge in the phantom. Incremental displacements of 0.05 mm of the suture centre were then applied, pulling the suture to the right while the degree of separation of the tissue from the left hand edge of the suture was monitored. This incremental loading allows both for data recording and dealing with non-linearities associated with large displacements. While shown in full form in the diagrams, symmetry of the model about the horizontal axis was used for processing efficiency. 3. Results and discussion Fig. 4 shows the distortion of the hole for a variety of loading conditions as represented by the finite element model and by imagery from the physical trials. In both cases it can clearly be seen that the tissue separates from the suture and the resulting gap would allow transmission of fluids or bacteria between the internal and external sides of the join. (163K) Fig. 4. Tissue separation from suture thread by imagery from the physical trials (a) and by the finite element model (b). Fig. 5 and Fig. 6 quantify the separation generated for a range of suture pull deflections as expressed by the finite element model. The suture pull deflection is defined as the movement of the suture centre as it passes through the phantom or model relative to its original position. Fig. 5 illustrates the separation values for a range of suture pull deflections. Fig. 6 shows the separation area generated and indicates that the separation area has a degree of proportionality to the applied deflection of the thread. For both the physical and analytical model, separation areas of up to 0.1 mm2 were found for higher suture tensions. With gut bacteria such as E. coli and Bacteroides fragilis having diameters of less than 1 μm [20] a gap of 0.1 mm2 could clearly allow for the possibility of the passage of bacteria clusters. (17K) Fig. 5. The separation of the phantom tissue from the left hand edge of the suture for a variety of rightward suture deflections. (23K) Fig. 6. Separation areas vs. suture thread pull. The relationship between the force exerted by the suture thread on the tissue was also explored in the physical model and the results of this can be seen in Fig. 7. A series of identical trials were carried out with the load on the suture being increased as the suture and tissue separation was captured. (9K) Fig. 7. Empirical results for suture pull force vs. separation area. Again this shows approximate proportionality between the applied force and the resultant measured leak area. There is however quite a significant spread in the results as a result of inhomogenity in the material and the thread cross-section. Some slight bulging of the phantom material placed in compression by the suture was observed however there was no visible buckling or creasing of the material. This would have generated significant non-linearities and so rendered comparison with the finite element model invalid. It was observed that the phantom material would tear immediately in front of the suture when loads above 140 grammes were applied. For more modest loads no obvious damage or plasticity was noted. Unlike the phantom and the finite element model presented here, the colon is a complex organ with several layers of muscle and tissue, each of which has different physical properties. In addition an internal suture tract will be subject to both fluidic pressure on the tract and the action of mucous and clotting material which will impact the progression of bacteria into and through the suture tract. Nonetheless this work has shown that there is a realistic likelihood of suture tracts opening up under tension. 4. Conclusion It perhaps comes as little surprise that the tension of sutures acting against restrained tissue will cause leaks. This work however has attempted to quantify and model the situation and has shown both from modelling and empirical work a degree of proportionality between the applied tension and the resultant potential leak area. At present the model is relatively basic, using phantom tissue material rather than the more complex situations encountered with living tissue with its nonlinearity, stress relaxation and non-homogeneous nature. Nonetheless this work is proving useful in helping to understand the causes and issues around anastomotic leaks of the colon which forms part of the wider work of this group. Acknowledgement The author wishes to acknowledge the UK EPSRC for supporting this work through grant EP/D003040/1. References [1] Wound closure products, Ethicon products worldwide; 2002. [2] D.J. Leaper, Wound closure—basic techniques, EWMA J 2 (2001) (1), pp. 19–24. [3] P.S. Chari, Susruta and our heritage, Indian J Plas Surg 36 (2003) (1), pp. 4–13. [4] A. Sonavane, S. Sharma, N. Gangopadhyay and A.K. Bansal, Clinico-microbiological correlation of suture-related graft infection following penetrating keratoplasty, Am J Ophthalmol 135 (2003) (1), pp. 89–91. SummaryPlus | Full Text + Links | PDF (112 K) [5] Y. Ünlü, U. Vural, H. Koçak, M. Ceviz, N. Becit and O. Akbulut, Comparison of topical haemostatic agents for the prevention of suture hole bleeding. An experimental study, Eur J Endovasc Surg 23 (2002), pp. 441–444. Abstract | Abstract + References | PDF (97 K) [6] G. Dickneite, H. Metzner and U. Nicolay, Prevention of suture hole bleeding using fibrin sealant: benefits of factor XIII, J Surg Res 93 (2000), pp. 201–205. Abstract | Abstract + References | PDF (98 K) [7] D. Koročsec, A. Holobar, M. Divjak and D. Zazula, Building interactive virtual environments for simulated training in medicine using VRML and Java/JavaScript, Comput Meth Prog Biol 80 (2005) (Suppl. 1), pp. S61–S70. Abstract | PDF (1773 K) [8] National service framework assessments No. 1 – NHS cancer care in England and Wales – Supporting data: 1—Who gets cancer and their survival, commission for health improvement/audit commission; 2001. [9] Haward R. Improving outcomes in colorectal cancer, NHS Executive; 1997. [10] Guidelines for the management of colorectal cancer. The association of coloproctology of Great Britain and Ireland; 2001. [11] J.M. Gilbert and G.E. Trapnell, Intraoperative testing of the integrity of left-sided colorectal anastomoses, Ann R Coll Surg 70 (1988), pp. 158–160. [12] A.A. Memon and C.G. Marks, Stapled anastomoses in colorectal surgery: a prospective study, Eur J Surg 162 (1996), pp. 805–810. [13] J.M.D. Wheeler and J.M. Gilbert, Controlled intraoperative water testing of left-sided colorectal anastomoses: are illeostomies avoidable?, Ann R Coll Surg 81 (1999), pp. 105–108. [14] C.D.M. Griffith and J.D. Hardcastle, Intraoperative testing of anastomic integrity after stapled anterior resection for cancer, J R Coll Surg E 35 (1990), pp. 106–108. [15] J.G. Docherty, J.R. McGregor, A.M. Akvol, C.D. Murray and D.J. Galloway, Comparison of manually constructed and stapled anastomoses in colorectal surgery, Ann Surg 221 (1995) (2), pp. 176–184. [16] Annual report 1999—Scottish audit of surgical mortality, SASM; 1999. [17] H. Yoshida, S. Tsutsumi, M. Mizunuma and A. Yanai, Three-dimensional finite element modelling of skin suture part 1: spindle model and S-shaped modified model, Med Eng Phys 22 (2000), pp. 481–485. SummaryPlus | Full Text + Links | PDF (1027 K) [18] H.R. Chaudry, B. Bukiet, M. Siegel, T. Findley, A.B. Ritter and N. Guzsela, Optimal patterns for suturing wounds, J Biomech 31 (1998), pp. 653–662. [19] P.H. DeHoff and J.E. Key, Application of the finite element analysis to determine forces and stresses in wound closing, J Biomech 14 (1981) (8), pp. 549–554. Abstract | Full Text + Links | PDF (614 K) [20] B. Li and B.E. Logan, Bacterial adhesion to glass and metal-oxide surfaces, Colloids Surf B: Biointerf 36 (2004), pp. 81–90. SummaryPlus | Full Text + Links | PDF (357 K) | Full Text via CrossRef Tel.: +44 1382 384908; fax: +44 1382 385508.