Antoine Lutz, Larry Greischar , Richard J
advertisement

BOLD signal in insula is differentially related to cardiac function
during compassion meditation in experts vs. novices.
Antoine Lutz1, Larry Greischar, David Perlman, Richard J. Davidson
University of Wisconsin, Madison, WI.,
1
To whom correspondence should be addressed: W. M. Keck Laboratory for Functional
Brain Imaging and Behavior, Waisman Center, University of Wisconsin, 1500 Highland
Avenue, Madison, WI 53705. E-mail: alutz@wisc.edu
Abstract:
The brain and the cardiovascular system influence each other during the processing of
emotion. The study of the interactions of these systems during emotion regulation has
been limited in human functional neuroimaging, despite its potential importance for
physical health. We have previously reported that trained expertise in cultivation of
compassion alters the activation of circuits linked with empathy and theory of mind in
response to emotional stimuli. Guided by the finding that heart rate increases more during
blocks of compassion meditation than neutral states, especially for experts, we examined
the interaction between State (compassion vs. neutral) and Group (novice, expert) on the
relation between heart rate and BOLD signal during presentation of emotional sounds.
Our findings revealed that BOLD signal in the right middle insula showed a significantly
stronger association with heart rate (HR) across state and group. This association was
stronger in the left middle/posterior insula when experts were compared to novices. The
positive coupling of HR and BOLD was higher within the compassion state than within
the neutral state in the dorsal anterior cingulate cortex for both groups, underlining the
role of this region in the modulation of bodily arousal states. This state effect was
stronger for experts than novices in somato-sensory cortices and the right inferior parietal
lobule (group by state interaction). These data confirm that compassion enhances the
emotional and somatosensory brain representations of others’ emotions, and that this
effect is modulated by expertise. Future studies are needed to further investigate the
impact of compassion training on these circuits.
Empathy can broadly be referred to as the capacity to understand and share another
person’s emotional experience. Recent functional magnetic resonance imaging (fMRI)
studies have demonstrated that observing another person’s emotional state activates parts
of the network involved in processing that same state in oneself, whether it is disgust,
touch, or pain (for reviews see {{64 de Vignemont,F. 2006; 67 Sommerville,J.A. 2006;
}}). For instance, the ‘pain matrix’, including the anterior insula (AI) and anterior
cingulate cortex (ACC), was activated when participants experienced pain themselves as
well as when they saw an arrow cue indicating that their partner had experienced pain
({{66 Singer,T. 2004; }}; for review {{64 de Vignemont,F. 2006; }}). These data are
consistent with perception-action models of empathy {{68 Preston,S.D. 2002; }}, in
which observing and imagining another person in a particular state is thought to activate a
similar state in the observer (simulation theory, {{69 Rizzolatti,G. 2001; }}). They also
fit with a similar framework that proposes that the observed and executed actions are
‘coded in a common cognitive and neural framework,’ enabling individuals to construct
‘shared representations of self and others’ ({{67 Sommerville,J.A. 2006; }}).
Recent studies have started to assess both state and trait factors modulating empathic
brain responses{{64 de Vignemont,F. 2006; }}. As state factors, top-down processes
such as cognitive appraisal or attention were found to influence empathy. For instance,
empathic brain responses were diminished when participants believed that the other
participant received pain as therapeutic treatment {{70 Lamm,C. 2007; }}. As a trait
factor, characteristics of the empathizer were found to modulate the magnitude of
empathic brain responses. For instance, Cheng et al. (put the date in parens here for the
ref) compared physicians who practice acupuncture to naive participants while observing
animated visual stimuli depicting needles being inserted into different body parts {{71
Cheng,Y. 2007; }}. The results indicated less empathy-related pain activity in AI and
ACC for the expert group as compared with the control group, suggesting a reduction of
empathic brain responses if the participants are familiar with such stimuli. Similarly,
inter-individual differences in neural empathy responses were found to correlate with
self-reported measures of empathy: the higher participants scored on these empathy
questionnaires, the higher their activation was in insula and ACC (e.g. {{66 Singer,T.
2004; 86 Jabbi,M. 2007; }}).
Along these lines, we recently studied the impact of a state of compassion (short for
“compassion and loving-kindness meditation state”) on this empathy-related network
(insula and ACC) in both expert and novice meditation practitioners {{4 Lutz,A. 2008;
}}. We studied compassion as both state and trait (experts vs. novices) factors influencing
empathy. Loving-kindness, the wish of happiness for others, and compassion, the wish to
relieve others’ suffering, are empathic responses which are motivated by an altruistic
concern for others. In many traditions, these qualities are cultivated through specific
meditation practices designed to prime behaviors compatible with these wishes in
response to actual interpersonal encounters {{73 Gethin, R. 1998; 37 Gyatso, Tenzin (the
XIV Dalai Lama) 1995; }}. Despite the potential social and clinical importance of these
affective processes, the possibility that they can be trained in a manner comparable to
attentional {{13 Slagter,H.A. 2007; }} or sensory-motor skills {{75 Maguire,E.A. 2006;
}} has received very limited scientific attention even though our recent study supports
this hypothesis. To cultivate these affective qualities, practitioners in a number of
traditions have developed meditative practices, which are thought to be essential to
counteract self-centered tendencies {{73 Gethin, R. 1998; 37 Gyatso, Tenzin (the XIV
Dalai Lama) 1995; }}. To investigate these questions, we previously assessed brain
activity using fMRI while novice and expert meditation practitioners generated a lovingkindness-compassion meditation state. To probe affective reactivity, we presented
emotional and neutral sounds during the meditation and comparison periods.
The
presentation of the emotional sounds was associated with increased pupil diameter and
activation of limbic regions (insular and cingulate cortices) during meditation (versus
rest). During meditation, activation in the insula was greater during the presentation of
negative sounds than positive or neutral sounds in expert versus novice meditators
(Group by State by Valence interaction). The strength of activation in the insula was also
associated with self-reported intensity of the meditation for both groups. Together these
data indicate that compassion and loving-kindness, along with the mental expertise to
cultivate these qualities, alter the activation of circuits previously linked to empathy in
response to emotional stimuli.
Because practitioners reported that a task would disrupt their ongoing meditation,
our previous study did not include a behavioral measure of the compassion state.
However, classical descriptions of this practice indicate that the generation of intense
compassionate feelings during meditation can produce specific bodily changes including
increased heart rate, goose bumps, or even tears {{37 Gyatso, Tenzin (the XIV Dalai
Lama) 1995; }}. Guided by these descriptions, in this report we analyze cardiac changes
during this meditation practice and examine the relation between heart rate (HR) changes
and simultaneously acquired (with fMRI) measures of brain function in experts and
novices. In particular, we use variations in HR during the task as a peripheral marker of
the visceral alterations that occur during the generation of compassion.
Voxelwise
correlations of this marker to the blood-oxygen-level dependent (BOLD) signal allow us
to identify the neural processes that accompany the autonomic changes during the
voluntary generation of compassion and to examine how the neurovisceral coupling
during meditation might differ between experts and novices.
Previous neuroimaging studies have addressed the question of central control of heart rate
in emotions by collecting parallel measurement of heart rate changes and changes in
activation as indexed by fMRI ({{78 Critchley,H.D. 2003; 77 Critchley,H.D. 2005; 76
Yang,T.T. 2007; }}{{87 Lane,R.D. 2009; }}). In one study where brain activity and heart
rate were simultaneously measured, the authors reported that the level of activity in
emotion-related regions (amygdala, insula, anterior cingulate) predicted subjects’ heart
rate responses to the presentation of emotional facial expressions {{76 Yang,T.T. 2007;
}}. Of importance for this study, Critchley et al. measured simultaneous
electrocardiography and brain activity during performance of cognitive and motor tasks.
Activity in the dorsal anterior cingulate cortex (ACC) was found to mediate the
modulation of bodily arousal states (sympathetic activity) during these tasks {{78
Critchley,H.D. 2003; }}. In a study from our laboratory where functional MRI of the
heart and brain were acquired nearly simultaneously, we found that greater activation in
the amygdala, anterior cingulate and the right middle frontal gyrus predicted greater
cardiac contractility during a stimulus paired with threat versus safety {{88 Dalton,K.M.
2005; }}.
Based on the findings reviewed above, our main hypothesis was that changes in heart rate
during compassion would be positively correlated with BOLD signal, as a function of
compassion meditation versus neutral state (State) and as a function of expertise (Group),
in regions important for feelings and emotions (e.g., insular cortex) and autonomic
control (e.g, dorsal ACC). In a first analysis, we investigated whether changes in HR
across both states were associated with changes in the brain. In this first analysis, the
HR/BOLD coupling parameters across states were influenced both by the main effect of
state and by changes in the degree of HR/BOLD couplings within each state. We then
specifically investigated the changes in the HR/BOLD couplings within each state. We
used a voxel-wise analysis performed on the HR/BOLD coupling parameter within each
state using a 2 × 2 factorial design with the first factor representing “Group” (10 experts
vs. 12 novices) and the second factor being the “State” (compassion meditation vs.
neutral state). This analysis provided a way to identify the brain regions which
specifically correlated with the fluctuations in emotional arousal during compassion
meditation. In addition, we tested whether these associations differed as a function of
expertise (“Group”, expert vs. novice practitioners).
Materials and methods
Participants.
We selected the participants from our previous studies{{6 Brefczynski-Lewis,J.A. 2007;
4 Lutz,A. 2008; }} on whom we also had clean electrocardiogram (ECG) data.
Participants from the current analysis included 10 long-term Buddhist practitioners whom
we classified as experts (mean age = 40.0 years, std = 9.6 years,) and 13 healthy
volunteers (mean age = 38.3 years, std = 9.1 years). The two groups did not differ in age
(t-test, t(1,21) = -0.3, p = 0.78) or gender (t-test, t(1,21) = -0.5, p = 0.65). All participants
were right-handed, except for one ambidextrous expert, as assessed by Edinburgh
Handedness Inventory {{89 Oldfield,R.C. 1971; }} and all but 4 were male (2 experts
and 2 age-matched novices). Buddhist practitioners, recognized as experts, were 5 of
Asian origin, 5 of Caucasian origin. To navigate the cultural differences among scientists
and long-term practitioners and for recruitment purposes, communication was facilitated
by Dr. Matthieu Ricard, an interpreter for the Dalai Lama who is a Western Buddhist
monk with scientific training and 35 years of meditative training in Nepal. Experts had
previously completed mental training in the similar Tibetan Nyingmapa and Kagyupa
traditions for 10,000 to 50,000 hours, which included a variety of meditation practices
including this compassion meditation. The length of their training was estimated based on
their daily practice and the time they spent in meditative retreats. Ten hours of meditation
per day of retreat was estimated as an average. The control participants were recruited via
advertisements in local newspapers and consisted of members of the UW Madison
community. The advertisement specifically recruited participants who had an interest in
meditation, but who had no prior meditative training. One week before the actual fMRI
scan session, novices were given written instructions on how to perform the meditation
practices, written by Dr. Ricard, and practiced this compassion meditation and two other
meditations for one hour a day for a week (20 minutes per meditation). Written informed
consent was obtained prior to scanning, in accordance with procedures and protocols
approved by the UW, Madison, Institutional Review Board.
A proficient Tibetan
speaking translator gave detailed procedural instructions and read the consent form to
three non-English speaking participants.
Meditative instruction
The state of loving-kindness and compassion is described as an "unconditional
readiness and availability to help living beings". This practice does not require
concentration on particular objects, memories or images, although in other meditations
that are also part of their long-term training, practitioners focus on particular persons or
groups of beings. Because “benevolence and compassion pervades the mind as a way of
being”, this state is called "pure compassion" or “non-referential compassion” (dmigs
med snying rje in Tibetan, pronounced “mig mey nying je” – literally: compassion (nying
je) without (mey) object (mig)). As described in Dr. Ricard’s instructions for the novices:
“During
the training session, the subject will think about someone he cares about, such as
his parents, sibling or beloved, and will let his mind be invaded by a feeling of altruistic
love (wishing well-being) or of compassion (wishing freedom from suffering) toward
these persons. After some training the subject will generate such feeling toward all beings
and without thinking specifically about someone. While in the scanner, the subject will
try to generate this state of loving kindness and compassion.” The Resting state (Tib.
“sem lung ma bstan”, pronounced “sem lung ma ten” – literally: neutral (lung ma ten)
mind (sem)) was a non-meditative state without specific cognitive content and with a lack
of awareness or clarity of the mind. Novice’s instructions were the following: “Neutral
here means that your emotional state is neither pleasant nor unpleasant and that you
remain relaxed. Try to be in the most ordinary state without being engaged in an active
mental state.” The controls’ ability to follow the instruction was assessed orally prior to
the data collection.
Protocol
Before the MRI scanning session, participants had a simulation session during
which they viewed an abbreviated version of the experimental paradigm while lying in a
mock MRI scanner (including head coil and digitized scanner sounds). This simulation
session served to acclimate all participants to the fMRI environment. We used a block
design, alternating ~3min of the state of meditation (4 cycles) with ~1.6 min of a resting,
neutral state (5 cycles), twice on separate days. There was an average per session of 643
seconds of meditation and 550 seconds of neutral state (264 seconds and 190 seconds
respectively for expert participant 2). A total of 25 2-second auditory sounds from the
International Affective Digitized Sounds (IADS) {{79 Bradley,M.M. 2000; }} for each
valence (positive, neutral and negative) were randomly presented across these two
sessions. These sounds were presented every 6-10 seconds after the first 40 seconds of
the meditative blocks and after 15 seconds of the resting blocks. Participants were
instructed to maintain their practice during the presentation of the sounds. During the
meditation and neutral states, eyes remained open and directed toward a fixation point on
a black screen. In this study we did not include a behavioral task because practitioners
reported that a task would disrupt their ongoing meditation. Two scans were run on two
separate days (1 day apart for experts, in general less than 1 week apart for novices) due
to the length of the scan run.
Data collection
MR images were collected with a GE Signa 3.0 Tesla scanner equipped with a
high-speed, whole-body gradient and a whole-head transmit-receive quadrature birdcage
headcoil. Whole-brain anatomical images were acquired at the end of each session using
an axial 3D T1-weighted inversion-recovery fast gradient echo (or IR-prepped fast
gradient echo) sequence. The field of view (FOV) was 240×240 mm with a 256×256
matrix. The slice thickness was 1-1.2 mm, with 0.9 by 0.9 mm in-plane resolution.
Functional data were collected using whole-brain EPI (TR = 2000, TE = 30ms). For
functional images, sagittal acquisition was used to obtain 30 interleaved 4 mm slices with
a gap of 1 mm between slices. The resulting voxel size was 3.75×3.75×5 mm (FOV =
240 mm, matrix = 64×64).
To ensure a high signal-to-noise ratio in areas prone to susceptibility artifacts, the
field inhomogeneities were lessened during data collection using high-order shim coils
that applied small correction gradients. In addition, acquisition of a 3D field map of the
magnetic field provided a complementary strategy to further reduce distortion (these data
were not acquired for the first three Buddhist experts). Based on these field maps, echo
planar imaging (EPI) data were unwarped so that accurate alignment to anatomical
images could be made. During the fMRI session, head movement was restricted using a
vacuum pillow (Vac Fix System, S&S Par Scientific). A Silent Vision system (Avotec,
Inc., Jensen Beach, FL) displayed the fixation point for the concentrative task. Eye
movements, fixations and pupil diameter were continuously recorded during the fMRI
scan using an iView system (sampling rate, 60 Hz) with a remote eye-tracking device
(SensoMotoric Instruments, 2001). We collected pupil data from 13 controls and 10
expert participants. Cardiac data were collected at 1000 Hz using GE's internal infrared
pulse oximeter.
Data analysis
Analysis techniques were similar to those described previously in our lab {{4
Lutz,A. 2008; }}. Briefly, data processing was implemented via AFNI (Analysis of
Functional Neural Images) {{80 Cox,R.W. 1996; }}. Data processing steps included
image reconstruction in conjunction with smoothing in Fourier space via a Fermi filter,
correction for differences in slice timing, 6-parameter rigid-body motion correction, and
removal of skull and ghost artifacts. The motion estimates over the course of the scan for
translation (inferior-superior, right-left, and anterior-posterior) and rotation (yaw, pitch,
roll) were charted. Time points with more than 0.5 mm of motion were removed from the
analysis. Two of the experts could not complete the second session for scheduling
reasons. Seven of the novices completed only one session as they were part of an
additional control group (see {{6 Brefczynski-Lewis,J.A. 2007; }}). One of the two
sessions was omitted for 2 of the experts and 2 of the novices, due to excessive head
motion. One of the sessions of 1 novice was omitted due to sleepiness. The final N for
the neuroimaging part of the study was 10 expert and 12 novice meditators. Between the
two subject groups, participants with only one session of data were not significantly
different (t-test, t(1,20) = -1.3, p = 0.2).
BOLD correlates of HR across states
The BOLD time series was modeled with a least-squares general linear model
(GLM) fit that included the heart rate, event-related sound responses across all states
(compassion and neutral), motion parameters in six directions and fourth-order
polynomial baseline functions. For the event-related sound responses, a standard gamma
function was used to model the shape of the hemodynamic response. For each subject, the
HR effect was modeled as 16 one-minute blocks (8 during each state) occurring during
the presentation of the sounds. The HR time series was positive during the time course of
the HR blocks and set to zero otherwise. The amplitude of each block was weighted by
the average HR value in this time window and z-transformed compared to all HR values
(HR mean across states was subtracted from each HR value and divided by the global HR
standard deviation across states). The beta coefficient of the HR regressor was converted
to percentage signal change using the mean overall baseline and spatially smoothed using
a 6mm RMS Gaussian filter; we refer to the resulting measure as the “HR/BOLD
coupling parameter”. The resultant parametric maps were transformed into the
standardized Talairach space via identification of anatomical landmarks on the highresolution anatomical image.
The analysis of the HR/BOLD coupling parameter was performed using
voxelwise t-tests comparing the HR/BOLD coupling parameter maps across both groups
to 0. A group comparison was performed using a voxelwise t-test comparing the
HR/BOLD coupling parameter maps between the two groups. Monte Carlo simulations
were run to correct for multiple testing to achieve an overall corrected mapwise alpha of
0.05. We found that the minimum cluster size was 1030 contiguous voxels with the data
thresholded at an uncorrected voxelwise p-value of p = 0.01. The data were then overlaid
onto a high-resolution anatomical image.
BOLD correlates of HR within each state
As some of the effects found in the above analysis on the HR/BOLD coupling
parameter might merely reflect the meditation state effect in the BOLD (see Lutz et al.
2008) and in the HR (see Table 1) (i.e. creating a bi-modal distribution of these values
between states), we further estimated a HR/BOLD coupling parameter within each state
(neutral and compassion). The analytical strategy was identical as above, except that we
used two separate HR regressors in the GLM, one for each state. The z-transformation of
HR values was run separately within each state.
The main analysis of the HR/BOLD coupling parameter was performed using a
2×2 factorial design (voxelwise 2-way ANOVA) with State (resting and meditation
states) as a within-subjects factor and Group as a between-subjects factor (Matlab
package for AFNI, G. Chen). Monte Carlo simulations were run to correct for multiple
testing to achieve an overall corrected mapwise alpha = 0.05. For the State effect and
Group by State effect, we found that the minimum cluster sizes were, respectively, 1030
and 3580 contiguous voxels with the data thresholded at an uncorrected voxelwise pvalue of p = 0.01 and p = 0.05 respectively.
Heart Rate Data:
The cardiac signal was analyzed using in-house developed Matlab software
(processHRV) and CMetX freeware {{81 Allen,J.J. 2007; }}. The distance between
each R-spike (the most prominent feature of the EKG waveform) was first calculated
using processHRV to obtain an interbeat interval (IBI) series. processHRV is an EKG
beat detection software program that allows for modification of beat detections while
simultaneously viewing the resulting IBI series superimposed on a spline interpolated (at
10 samples per second) version. Missed and artifactual beats can be identified by visual
inspection of the IBI series, and corrected by manual addition or removal of individual
beats. For each subject and for each State (compassion or neutral), we extracted from the
IBI series 8 1-minute intervals of cardiac data during the presentation of emotional
sounds. Heart rate (HR), heart rate variability (HRV) and respiratory sinus arrhythmia
(RSA) were computed using the CMetX program for each of these 16 1-minute intervals.
We investigated changes in HR, HRV and RSA as a function of State (compassion versus
neutral), Block (8 1-minute intervals) and Group (experts versus novices) using an 8×2×2
factorial design (repeated measures analysis of variance (ANOVAs)).
Results
Effects of compassion state on HR
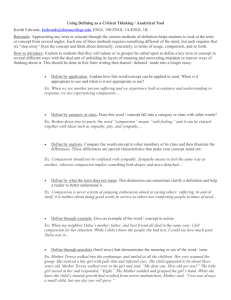
We investigated changes in HR as a function of Block, State and Group using an 8×2×2
factorial design (repeated measures analysis of variance (ANOVA)). Table 1 and Figure
1 display the results. We found that HR was higher during compassion versus neutral
states (main effect of State), and that this increase was stronger for the experts than the
novices (the interaction between State and Group is displayed in Table 1 and in Figure 1).
For experts, the mean HR was 64.2 +/- 8.2 STD and 67.1 +/- 9.8 STD beats per minute in
the neutral and compassion states respectively. For novices, the mean HR was 64.3 +/7.0 STD and 64.8 +/-6.7 STD beats per minute in the neutral and compassion states
respectively. We also ran identical exploratory ANOVAs on heart rate variability (HRV)
and respiratory sinus arrhythmia (RSA). HRV reflects the dynamic relationship between
sympathetic and parasympathetic nervous system influences, and RSA is thought to
measure only the parasympathetic influence {{81 Allen,J.J. 2007; }}. There were no
significant results in the analysis of these metrics and consequently, they were not used in
the subsequent analysis with BOLD data. In brief, the generation of compassion during
the task increases the cardiovascular arousal compared to the neutral state, and this
increase was modulated by meditation expertise.
BOLD correlates of HR across states
In this first analysis, the HR/BOLD coupling parameters across states can be influenced
both by the main effect of state and by changes in the degree of HR/BOLD coupling
within each state. For both groups, there was a positive coupling between HR and
average BOLD signal across neutral and compassion states in right middle insula cortex,
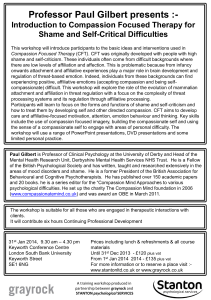
somatosensory cortex, right inferior parietal cortex and premotor cortex (BA 6) (voxelwise t-test, corrected, see Table 2). To test our main hypothesis on the role of the insula
in compassion, we contrasted the maps containing the intra-subject HR/BOLD coupling
parameters from the experts with the ones from the novices. As predicted, the amplitude
of HR/BOLD coupling parameters across states was higher for experts than novices in
the left middle/posterior insula (voxel-wise t-test, corrected, Figure 2.A, Table 3).
Positive couplings were also found in the left somato-sensory cortex, mid-anterior
cingulate cortex and in several regions associated with mirror-neuron-like systems
(premotor cortex, BA 6 and left inferior parietal lobule, see Table 3). Considering our
hypothesis, we next evaluated whether this cluster in the insula showed compassionspecific neural correlates of HR. We contrasted the HR/BOLD coupling parameter in this
region of interest (ROI) between the two conditions (compassion and neutral) and found
that this association was presented only for experts during the compassion condition, and
the coupling during compassion was higher for experts than novices (Figure 2.B).
Together these results support our main hypothesis that the brain regions underlying
emotions and feelings were positively coupled with heart rate as a function of state and
expertise.
Compassion-specific correlates of HR
In addition, we explored emotion-specific correlates of HR as a function of state
(compassion versus neutral) and group (experts versus novices) using a 2×2 factorial
design. This second analysis provided a way to identify the brain regions which
specifically correlated with the fluctuations in emotional arousal during compassion
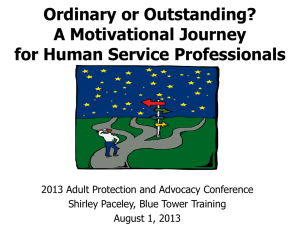
meditation. The main effect for State showed stronger HR/BOLD coupling parameter
during meditation than rest in dorsal ACC/premotor cortex and right somatosensory
cortex (voxel-wise repeated ANOVA, Figure 3, Table 4), supporting our hypothesis
regarding the role of dorsal ACC in autonomic control. No cluster in the insula passed
our correction criteria. Voxelwise analysis of Group by State interactions showed experts
to have had stronger HR/BOLD coupling parameters in a cluster encompassing the right
somatosensory cortex and right inferior parietal lobule (IPL) (Figure 4) and a large
cluster including parahippocampal / fusiform gyrus / occipital gyrus (Table 5). In the
cluster that included IPL, the magnitude of the Group-by-State interaction was driven by
a larger difference in the HR/BOLD coupling parameter between compassion and rest for
the experts than the novices (see Figure 4.D and its legend). The coupling parameter for
experts during compassion was positive and larger than the one during the neutral state
(Figure 4). These results highlighted that brain regions associated with mirror-neuron-
like systems {{69 Rizzolatti,G. 2001; 83 Iacoboni,M. 2005; }}), such as IPL, were
positively coupled with heart rate as a function of the interaction between state and
expertise, and that this effect was driven by experts during the generation of compassion.
Discussion
1) From empathy to compassion
In the current study, we found that changes in HR across states were positively
associated with the right middle insula and somatosensory regions, right IPL and
premotor regions (BA6), as well as right TPJ (Table 2). This pattern of neurovisceral
coupling was more pronounced for experts than novices in the left hemisphere (left
insula ,left somatosensory cortex and left IPL) and in the mid-ACC (Table 3, Figure 2).
A growing number of neuroimaging studies have reported a similar pattern of activation
in the insular cortex, somatosensory cortex, parietal cortex, and mid-ACC/premotor
cortex when participants are asked to imagine others’ pain from a somatosensory
perspective (e.g. while looking at body parts in painful situations, {{70 Lamm,C. 2007; ;
82 Danziger,N. 2009; }}). Thus, the coupling between HR and BOLD signal in these
regions may be interpreted within an ‘embodied’ or ‘simulation’ framework proposed by
several authors {{69 Rizzolatti,G. 2001; ; 68 Preston,S.D. 2002; 67 Sommerville,J.A.
2006; ; }} which emphasizes the importance of motor predictions and motor simulations
in processing the emotional significance of affective events. This finding was confirmed
in our second analysis where we specifically compared the neurovisceral coupling within
each state. Again we found that, during the compassion state only, HR and BOLD
activity was positively coupled in somatosensory regions, and, more strongly for the
experts, in the IPL, a region important in the imitation or understanding of others’
actions{{83 Iacoboni,M. 2005; 69 Rizzolatti,G. 2001; }}.
While the present study confirms our previous finding on the role of the insular cortex in
the state of compassion, these results also differed from our previous report {{4 Lutz,A.
2008; }} in several ways. In particular, our previous study showed a stronger activation
during compassion (State effect) and more for the experts than the novices (Group by
State interaction) in regions commonly recruited during high-level social-cognitive tasks
(e.g. mentalizing, see for review {{90 Decety,J. 2007; }}) and during the redirection of
attention to salient events (TPJ, posterior superior temporal gyrus, medial prefrontal
cortex and posterior cingulate cortex/precuneus). In the current study, this circuit was not
coupled with the HR changes either across states or within states, except for a positive
HR/BOLD coupling parameter in the right TPJ across State and for both groups (Table
2). These differences may be attributed to the different analytical strategies between these
two studies. In our previous analysis, we primarily modeled the perceptual response to
the emotional sounds and its modulation by the states (compassion vs neutral) and
expertise (experts vs. novices). By contrast, here we modeled the brain activity in 1minute intervals in which the sounds were presented (block effect) while removing from
the BOLD signal the variance attributed to the evoked response to sounds per se. This
choice was guided by the necessity to compute our cardiac measures (HR, RSA, HRV)
within time windows of at least 60 seconds {{81 Allen,J.J. 2007; }}. Because the current
analysis reflected the block effect more than the evoked brain responses to sounds, the
brain regions showing a state effect or a state by expertise effect in the current study
might reflect some of the contextual processes that participated in the modulation of the
perceptual responses to the sounds identified in our previous study. In this view, the
generation of a state of compassion recruited empathy-related regions and regions which
are part of a motor-neuron-like system that differentially modulates the perception of the
emotional sounds.
In the present study, our neuroimaging and physiological observations provide evidence
for an association between dorsal ACC activity and modulation of heart rate: the more
heart rate increases across blocks of compassion meditation, the more ACC was activated
for both groups (Figure 3). This link was not detected during the neutral state.
Accumulating evidence supports the view {{78 Critchley,H.D. 2003; }} that this region
of dorsal ACC is mediating the regulation of bodily states of arousal so the organism can
meet behavioral demands; for this reason some authors (e.g. {{85 Craig, A.D. 2007; }})
have coined the term “limbic motor cortex” for the cingulate cortex. This neurovisceral
coupling in ACC was previously observed during cognitive and emotional tasks{{78
Critchley,H.D. 2003; 77 Critchley,H.D. 2005; ; }}. Our finding adds to this literature by
showing that a purely mental state (without an explicit behavioral task) is sufficient to
produce autonomic changes via this circuitry. In this view, observations of aboulia and
motivational impairments in patients with large cingulate lesions, in the absence of
attentional or frontal executive impairments, broadly illustrate the role of this region in
generating self-initiated preparatory bodily states {{91 Devinsky,O. 1995; }}. According
to that framework, the activity in dorsal ACC during the increase in HR during
compassion may mediate some of the motivational processes underlying this prosocial
state.
2) Exploring the potential impact of compassion meditation on emotional balance:
Meditation can be conceptualized as a family of complex emotional and attentional
regulatory training regimes developed for various ends, including the cultivation of wellbeing and emotional balance (for a recent review see {{5 Lutz,A. 2008; }}). The impact
of such mental training on peripheral biological processes that are important for physical
health and illness is not yet well understood. Increasing evidence suggests that meditation
may impact physiological pathways, including the cardio-vascular {{99 Wu,S.D. 2008;
100 Phongsuphap,S. 2008; 102 Benson,H. 1997; }}, immune and neuroendocrine
systems {{92 Davidson,R.J. 2003; 93 Pace,T.W. 2009; 94 Carlson,L.E. 2007; 95
Carlson,L.E. 2004; }}, which are critical for disease development and progression. To
date, the majority of studies examining the impact of meditation on peripheral biology
have investigated practices that aim to calm the mind, or improve focused attention, or
develop mindfulness (for a review of these practices see ){{5 Lutz,A. 2008; }}. These
studies have commonly reported that meditation causes parasympathetic changes in
cardiac measures {{99 Wu,S.D. 2008; 100 Phongsuphap,S. 2008; 102 Benson,H. 1997;
}}, which are known to predict various health benefits (for review {{101 Thayer,J.F.
2007; }}). In contrast, we observed that compassion meditation produced elevated heart
rate, which can occur as a result of decreased parasympathetic activity, increased
sympathetic activity or a combination of both. Since we found that compassion
meditation had no significant effect on a standard cardiac measure of parasympathetic
activity (i.e. RSA), it may be that the heart rate increases observed during compassion
meditation in the experts are more driven by increased in sympathetic activity. Such an
increase in heart rate has already been reported during specific Kundalini Yoga breathing
techniques {{98 Peng,C.K. 2004; }}. Increase in HR was also previously associated with
helping in ambiguous emergencies, even if these studies did not differentiate between
empathetic and personal distress reactions {{103 Gaertner, S.L. 1977; 104 Sterling, B.
1984; }}. Our current finding that compassion amplified the emotional saliency of
emotional stimuli is consistent with the traditional function of this meditation {{74 Dalai
Lama X 1995;}} and in combination with previous findings suggests that one outcome of
compassion training is to sensitize the practitioner to the emotional experience of others.
Traditional accounts of the compassion practice also suggest that, even if strong personal
distress can occur during compassion meditation, this distress is alleviated by two factors:
1) cultivating an equanimity stance toward suffering, in particular one’s own suffering,
such that one is able to bring suffering to mind without being swept away by it; and 2) a
conviction that, from the longest term perspective, complete relief of others’ suffering is
definitely achievable {{93 Pace,T.W. 2009; 74 Dalai Lama X 1995; }}. For that reason,
compassion meditation is often preceded by conceptual training that helps practitioners
develop cognitive schemas which cultivate a sense of equanimity and hopefulness and
meditation training that develops a non-judgmental, non-reactive stance toward one’s
habitual patterns of emotional reactivity. These two factors are said to protect the
meditators from suffering from compassion burnout. Recent studies provide preliminary
evidence for this protective effect of compassion on affective reactivity: self-compassion
was associated with less anxiety in response to a mock job interview and less distress
after getting neutral feedback in response to a videotaped speech performance {{96
Leary,M.R. 2007; }}, and the amount of practice correlated with improvements in
immune and behavioral responses to a psychosocial stressor within the group of
participants randomized to the type of compassion-based conceptual training mentioned
above {{93 Pace,T.W. 2009; }}. Although the present study did not detect any
parasympathetic effects, the impact of compassion meditation on emotion regulation
might result from a complex pattern of interaction between sympathetic and
parasympathetic influences which needs to be further explored in future studies.
3) Limitations of the study and direction for future studies
Because novices and experts differ in many respects other than simply the extent of
mental training, such as culture of origin and first language, longitudinal research that
follows individuals over time in response to compassion training will be needed to further
substantiate our findings. It will also be essential to assess the impact of such emotional
and empathic training on behavioral tasks involving altruism and more generally
involving emotional reactivity and regulation. The long-term question is to evaluate
whether repeated practice in such techniques could result in enduring changes in
emotional reactivity and affective style {{97 Davidson,R.J. 2004; }}. The fact that
systematic changes in cardiac function and neurovisceral coupling were observed during
the mental practice of compassion and in response to auditory emotional stimuli
presented during the practice, and the fact that robust differences were observed between
experts and novices, suggests that the next steps to evaluate the behavioral impact of this
training and to assess its effects longitudinally are warranted.
Acknowledgments:
We would like to acknowledge Dr. Matthieu Ricard for assistance with task design,
participant recruitment and written meditation instructions. Dr. John Dunne for Tibetan
translation and clarifications on Buddhist meditative techniques. We also thank the Mind
and Life Institute for helping to facilitate this work. Helen Weng for helpful comments on
a preliminary version of the manuscript. This work was supported by grants from the
National Institute of Mental Health (NIMH P50-MH069315 to R.J.D.), the National
Center for Complementary and Alternative Medicine (P01-AT004952 to R.J.D. and to
A.L, and U01AT002114-01A1 to A.L.), and gifts from Bryant Wangard and Ralph
Robinson, Keith and Arlene Bronstein and the John W. Kluge Foundation (to R.J.D.).
Author contributions AL, and RJD designed the study. AL was involved in data
collection. AL, LLG and D.P. analyzed the data. AL wrote the paper. All authors
discussed the results and commented on the manuscript.
Table 1: Heart Rate (HR) Results (Repeated-Measured ANOVA)
Factors
F(1,147)
p-Value
The HR analysis was performed with HR Compassion as the dependent variable, State
(Neutral vs. Compassion) and Block (8 blocks across the session) as within-subject
factors and Group (Experts vs. Novices) as the between-subject factor. Note that HR
increases for both groups during compassion, and that this increase was larger for experts
than novices (paired t-test, t(1,21) = -2.1, p < 0.05, 10 experts and 13 novices).
Table 2. BOLD correlates of HR across states
Clusters extracted from the ROIs showing a positive HR/BOLD coupling parameter
across the blocks of neutral and compassion states (average t score in each cluster) (10
experts and 12 novices). No cluster with negative HR/BOLD coupling parameter was
found.
Location
Side Volume
Middle Insula / Pre- and Postcentral gyri
R
12827
Cerebellum
R/ L 5287
Inferior Occipital gyrus
R/ L 4906
Paracentral Lobule, medial frontal gyrus
R/L 2236
Parahippocampal gyrus/ hippocampus
L
1594
Angular gyrus/ middle temporal Gyri (TPJ) R
1571
Medial Frontal gyrus
L
1360
Medial Frontal gyrus
L
1192
Inferior Parietal Lobule
R
1100
Peak Coordinates
40 3 11/ 45 -16 39
-34 -70 -34
-33 -86 -3
-1 -18 53
-32 -27 -12
41 -61 29
-10 48 24
-9 36 53
36 -44 48
t score
3.1
3.1
3.0
3.1
3.0
3.1
3.1
3.0
3.1
Table 3: Expertise-related effect in BOLD correlates of HR across states
Clusters extracted from the ROIs showing a stronger HR/BOLD coupling parameter for
experts than novices across the blocks of neutral and compassion states (average t score
in each cluster) (10 experts and 12 novices).
Location
Post- and pre-central gyri
Side Volume
L
8553
Post-central gyrus
L
1203
Inf. Frontal gyrus/ Pre-central gyrus R
2269
Medial Frontal gyrus/ paracentral lobule L
7131
Cerebellum
R/L 5460
Inferior parietal lobule
L
4073
Anterior mid-cingulate cortex
L
3334
R
Middle Frontal gyrus
2729
L
Insula
1771
Parahippocampal gyrus
L
1281
Parahippocampal gyrus
R
1301
Peak Coordinates
-28 -26 56
-59 -13 23
45 -5 26
-6 -18 55
24 -41 27
-42 -36 43
-8 -10 40
22 -17 62
-35 -3 0
-31 -30 -12
31 -29 -12
t
3.4
score
3.0
3.1
3.1
3.1
3.3
3.2
3.1
3.1
3.0
3.3
Table 4: Compassion-specific effect on HR/BOLD coupling parameters: main effect
of State
These clusters were driven by a stronger HR/BOLD coupling parameter within
compassion than neutral state across Groups. In these clusters, HR/BOLD coupling
parameters were higher during compassion than neutral state, except in one cluster in the
orbito-frontal cortex (10 experts and 12 novices).
Location
Side Volume Peak Coordinates F
Middle occipital gyrus/cuneus 7137 R
25 -86 10
6.7
score
6845
Middle occipital gyrus/cuneus
L
-21 -91 8
6.7
5802 L
Orbito-frontal cortex
-36 45 -7
6.5
Dorsal anterior cingulate cortex 5943 L
-9 9 47
6.0
3608 R
Post- and precentral gyri
34 -15 46
5.8
Table 5: Compassion-specific effect on HR/BOLD coupling parameter: State by
Group interaction.
These clusters showed a stronger HR/BOLD coupling parameter within compassion than
neutral state more strongly for experts than novices (10 experts and 12 novices).
Location
Sid Volum Peak
F
R
Pre- and post central gyri/ IPL
4141
38 -29 50
5.3
e
R
e
Coordinates
sc
Parahippocampal/ Occip./ fusiform gyri
5173
23 -76 11
6.5
ore
Legend 1: Compassion increases emotional cardiovascular arousal. Average HR
significantly increased from neutral to compassion states for 10 experts (red) and 13
novices (blue) (main effect of State, see Table 1). During both states, emotional
vocalizations were presented to the participants. Note that the practitioners showed
significantly larger HR increase than the novices (State by Group interaction, see Table
1).
Legend 2: Expertise effect on HR/BOLD coupling parameter across states.
A. Voxel-wise analysis comparing the coupling between HR and BOLD across states
(compassion and neutral) between 10 experts (red) and 12 novices (blue) (z = 2,
corrected, color code: orange, p < 0.05, yellow, p < 0.02) in insula (ins.). B. The cluster
in the left insula shows an expertise-related effect consistent with our previous study
(Lutz, 2008). The average HR/BOLD coupling in the left insula (Ins.) was larger for
experts than novices (t-test, t(1,20) = 3.6, p < 0.005) and significantly positive for experts
(t-test, t(1,9) = 3.9, p < 0.005). The coupling in this cluster shows additional emotionspecific effects: for both groups, there was no significant coupling within the neutral state
(t-test, at least p>0.45 with each group), but, within the compassion state, the coupling
was higher for experts than novices (t-test, t(1,20) = 3.8, p < 0.005) and was significantly
positive only for the experts (t-test, t(1,9) = 4.0, p < 0.005). The HR/BOLD coupling
represents the percent BOLD signal change per ratio of change in heart rate.
Legend 3: Compassion-specific neural correlates of HR. A. Voxel-wise analysis of the
main effect of State (compassion vs. neutral) on the HR/BOLD coupling parameter in the
dorsal ACC/premotor cortex (y = 22, corrected, color code: orange, p < 0.05, yellow, p <
0.02) 10 experts (red) and 12 novices (blue)). B. In this cluster the HR/BOLD coupling
parameter was larger during the compassion state than the neutral state for 10 experts
(red) and 12 novices (blue) (repeated ANOVA, main effect of state, F(1,20) = 8.1, p =
0.01). This finding suggests stronger cardiovascular autonomic control from the dorsal
ACC during the compassion state than the neutral state.
Legend 4: Expertise effect on compassion-specific neural correlates of HR. A.
Voxel-wise analysis of Group (experts vs. Novices) by State (compassion vs. neutral)
interaction on the HR/BOLD coupling parameter in somatosensory and inferior parietal
lobule (z = 52, corrected, color code: orange, p < 0.05, yellow, p < 0.02, 10 experts (red)
and 12 novices (blue)). B. Compassion expertise affects the HR/BOLD coupling
parameter, in particular in the inferior parietal lobule (IPL). In the cluster from A., the
experts showed a larger HR/BOLD coupling parameter in compassion than neutral states
and than the novices (repeated ANOVA, F(1,20) = 7.2, p < 0.05).
Bibliography: