Community respiratory clinic referral form
advertisement

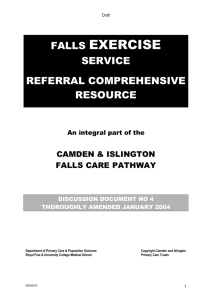
Community Respiratory Clinic Referral Form Forename: Surname: DOB: NHS No: Referral process Fax/ E-mail completed form to: Patient Address: Fax: 0300 008 3133 E-mail: westherts.resp@nhs.net To discuss suitability contact: Tel No: 01442 287604 Daytime Tel No: Relative / Carers Tel No: Diagnosis COPD Reason for Referral: Bronchiectasis Asthma Past Medical History Medication (list or attach printout) Drug Dose Frequency Spirometry Result % Predicted FEV1 FVC FEV1 / FVC ratio Preferred location for appointment: Hemel Hempstead Potters Bar GP Details or Stamp: Referred by: GP Name: Name: Practice: Contact Tel No: Watford St Albans Edgware Home visit Date referred: Community Clinic Referral Criteria: Confirmed diagnosis of COPD, asthma, bronchiectasis Condition Unstable Frequent exacerbations (>2 per year) Frequent admissions to hospital Clinical symptoms disproportionate to lung function tests or clinical decline Problematic withdrawal of steroids Complex patients requiring specialist MDT review Exclusion Criteria Lung Cancer – cancer 2 week wait referral Tuberculosis (new case) – WHHT referral ILD & NIV (direct referral from acute hospital) Patient with a current exacerbation, not responding to treatment or requiring more intensive support will be cared for under Hospital at Home. Please contact respiratory nurse specialist direct on Tel: 07944 960825 for Home Oxygen, Pulmonary Rehab & OSA complete separate community respiratory referral form