החמרה לעלון
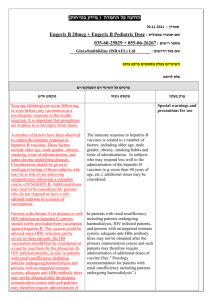
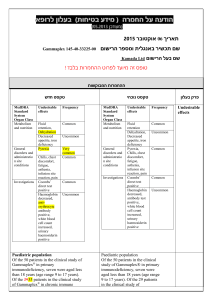
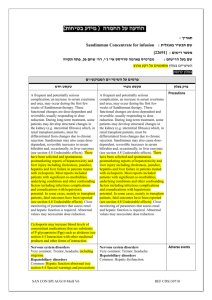
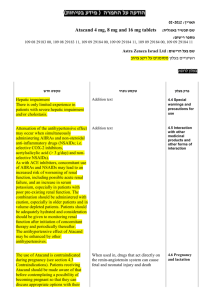
advertisement

רופא בעלון ללרופא בטיחות) בעלון )מידע בטיחות החמרה (( מידע על החמרה הודעה על הודעה )).102.50 .102.50 (מעודכן (מעודכן 213213102. תאריך Levitra 10mg orodispersible tablets שם תכשיר באנגלית ומספר הרישום 146-52-33322-01, 146-52-33322-00 שם בעל הרישום ! טופס זה מיועד לפרוט ההחמרות בלבד ההחמרות המבוקשות טקסט חדש טקסט נוכחי פרק בעלון Indication contraindications Levitra is contraindicated in patients who have loss of vision in one eye because of non-arteritic anterior ischemic optic neuropathy (NAION), regardless of whether this episode was in connection or not with previous phosphodiesterase 5 (PDE5) inhibitor exposure (see section 4.4). (Special Warnings and Medicinal products for the treatment of erectile dysfunction should generally not be used in men for whom sexual activity is inadvisable (e.g. patients with severe cardiovascular disorders such as unstable angina or severe cardiac failure [New York Heart Association III or IV]). Precautions for use) The safety of vardenafil has not been studied in the following sub-groups of patients and its use is therefore contraindicated until further information is available: - severe hepatic impairment (Child-Pugh C), - end stage renal disease requiring dialysis, - hypotension (blood pressure <90/50 mmHg), - recent history of stroke or myocardial infarction (within the last 6 months), The safety of Levitra has not been studied in the following sub-groups of patients and its use is therefore not recommended: severe hepatic impairment, endstage renal disease requiring dialysis, hypotension, resting systolic blood pressure of <90 mm Hg, recent history of stroke or myocardial infarction, within the last 6 months, unstable angina and known hereditary degenerative retinal disorders such as retinitis pigmentosa. In men for whom sexual activity is not recommendable because of their underlying cardiovascular status, agents for the treatment of erectile dysfunction should generally not be used. - unstable angina, and known hereditary retinal degenerative disorders such as retinitis pigmentosa. CYP Inhibitors Concomitant use of vardenafil with the potent CYP3A4 inhibitors ketoconazole and itraconazole (oral form) is contraindicated in men older than 75 years. The use of Levitra orodispersible tablets in combination with erythromycin, ketoconazole, itraconazole, clarithromycin, indinavir or ritonavir is contraindicated. Posology, dosage & administration Levitra 10 mg orodispersible tablet is not bioequivalent to Levitra 10 mg filmcoated tablet (see section 5.1). Special populations Elderly population (≥65 years old) Dose adjustments are not required in elderly patients. However, an increase to a maximum dose of Levitra 20 mg film-coated tablets should be carefully considered depending on the individual tolerability (see sections 4.4 and 4.8). Geriatric patients Dose adjustment is not required in elderly patients Patients with hepatic impairment Hepatic impairment Levitra 10 mg orodispersible tablets are not indicated as a starting dose in patients with mild hepatic impairment (Child-Pugh A). Patients with mild hepatic impairment should start treatment with Levitra 5 mg film-coated tablets. Based on tolerability and efficacy, the dose may be increased to Levitra 10 mg and 20 mg film-coated tablets, or Levitra 10 mg orodispersible tablets. No dose adjustment is needed in patients with mild hepatic impairment, Child-Pugh A. The maximum dose recommended in patients with moderate hepatic impairment (Child-Pugh B) is Levitra 10 mg as film-coated tablets (see section 5.2). Patients with renal impairment Renal impairment No dose adjustment is required in patients with mild to moderate renal impairment. In patients with severe renal impairment (creatinine clearance <30 ml/min) a starting dose of Levitra 5 mg film-coated tablets should be considered. Based on tolerability and efficacy, the dose may be increased to Levitra 10 mg and 20 mg film-coated tablets, or Levitra 10 mg orodispersible tablets. Levitra orodispersible tablet is not for use in patients with end-stage renal failure (see section 4.3). No dose adjustment is needed in patients with mild, CrCl > 50-80 mL/min, moderate, CrCl > 30-50 mL/min, or severe, CrCl < 30 mL/min, renal impairment. The pharmacokinetics of vardenafil has not been studied in patients requiring dialysis. (See section “Pharmacokinetic properties”). Children and adolescents Paediatric population Levitra orodispersible tablets are not indicated for individuals below 18 years of age. There is no relevant indication for use of Levitra orodispersible tablets in children and adolescents. Levitra is not indicated for use in children. Tolerability of the maximum dose of Levitra 20 mg film-coated tablets may be lower in elderly patients (≥ 65 years old) (see sections 4.2 and 4.8). Special Warnings and Special Precautions for Use Concomitant use of CYP 3A4 inhibitors Concomitant use of vardenafil with potent CYP 3A4 inhibitors such as itraconazole and ketoconazole (oral form) should be avoided as very high plasma concentrations of vardenafil are reached if the medicinal products are combined (see sections 4.5 and 4.3). Vardenafil dose adjustment might be necessary if moderate CYP 3A4 inhibitors such as erythromycin and clarithromycin, are given concomitantly (see section 4.2 and 4.5). Concomitant intake of grapefruit or grapefruit juice is expected to increase the plasma concentrations of vardenafil. The combination should be avoided (see section 4.5). Concomitant intake of grapefruit juice is expected to increase the plasma concentration of vardenafil. The combination should be avoided. Effect on QTc interval Single oral doses of 10 mg and 80 mg of vardenafil have been shown to prolong the QTc interval by a mean of 8 msec and 10 msec, respectively. And single doses of 10 mg vardenafil co-administered concomitantly with 400 mg gatifloxacin, an active substance with comparable QT effect, showed an additive QTc effect of 4 msec when compared to either active substance alone. The clinical impact of In a study of the effect of Levitra on QT interval, in 59 healthy male volunteers, therapeutic and supratherapeutic doses of Levitra, 10 and 80 mg, respectively, produced increases in QTc interval (See section “Pharmacodynamic properties”). A postmarketing study evaluating the effect of combining vardenafil with another drug of comparable QT effect showed an additive QT effect when compared with either drug alone (See section “Pharmacodynamic properties”). These observations should be considered in clinical decisions when prescribing Levitra to patients with known history of QT prolongation or patients who are taking medications known to prolong the QT interval. Patients taking Class IA, e.g. quinidine, procainamide or Class III, e.g. amiodarone, sotalol, antiarrhythmic medications or those with congenital QT prolongation, should avoid using Levitra. these QT changes is unknown (see section 5.1). The clinical relevance of this finding is unknown and cannot be generalised to all patients under all circumstances, as it will depend on the individual risk factors and susceptibilities that may be present at any time in any given patient. Medicinal products that may prolong QTc interval, including vardenafil, are best avoided in patients with relevant risk factors, for example, hypokalaemia, congenital QT prolongation, concomitant administration of antiarrhythmic medicinal products in Class IA (e.g.quinidine, procainamide), or Class III (e.g. amiodarone, sotalol). Effect on vision Visual defects and cases of non-arteritic Transient vision loss and cases of ischemic optic neuropathy (NAION) have been reported in connection with the intake of Levitra and other PDE5 inhibitors. The patient should be advised that in the case of sudden visual defect, he should stop taking Levitra orodispersible tablets and consult immediately a physician (see section 4.3). Effects of other medicinal products on vardenafil In vivo studies Although specific interaction studies have not been conducted, the concomitant use of other potent CYP3A4 inhibitors (such as itraconazole) can be expected to produce vardenafil plasma levels comparable to those produced by ketoconazole. Concomitant use of vardenafil with potent CYP 3A4 inhibitors such as itraconazole and ketoconazole (oral use) should be avoided (see sections 4.3 and 4.4). In men older than 75 years the concomitant use of vardenafil with itraconazole or ketoconazole is contraindicated (see section 4.3). Grapefruit juice being a weak inhibitor of CYP3A4 gut wall metabolism, may give rise to modest increases in plasma levels of vardenafil (see section 4.4). The pharmacokinetics of vardenafil (20 mg) was not affected by coadministration with the H2-antagonist ranitidine (150 mg twice daily), digoxin, warfarin, glibenclamide, alcohol (mean maximum blood alcohol level of 73 mg/dl) or single doses of antacid (magnesium hydroxide/aluminium hydroxide). Although specific interaction studies were not conducted for all medicinal products, population pharmacokinetic analysis showed no effect on vardenafil pharmacokinetics of the following concomitant medicinal products: acetylsalicylic acid, ACE-inhibitors, betablockers, weak CYP 3A4 inhibitors, diuretics and medicinal products for the treatment of diabetes (sulfonylureas and metformin). non-arteritic ischemic optic neuropathy (NAION) have been reported in connection with the intake of PDE5 inhibitors, including Levitra. The patient should be advised that in the case of sudden vision loss, he should stop taking Levitra and immediately consult a physician (See section “Undesirable Effects”). Interaction with Other Medicaments and Other Forms of Interaction Effects of vardenafil on other medicinal products In vivo studies Since alpha-blocker monotherapy can cause marked lowering of blood pressure, especially postural hypotension and syncope, interaction studies were conducted with vardenafil. In two interaction studies with healthy normotensive volunteers after forced titration of the alpha-blockers tamsulosin or terazosin to high doses, hypotension (in some cases symptomatic) was reported in a significant number of subjects after co-administration of vardenafil. Among subjects treated with terazosin, hypotension was observed more frequently when vardenafil and terazosin were given simultaneously than when the dosing was separated by a time interval of 6 hours. Based on the results of interaction studies conducted with vardenafil in patients with benign prostatic hyperplasia (BPH) on stable tamsulosin, terazosin or alfuzosin therapy: When vardenafil (film-coated tablets) was given at doses of 5, 10 or 20 mg on a background of stable therapy with tamsulosin, there was no symptomatic reduction in blood pressure, although 3/21 tamsulosin treated subjects exhibited transient standing systolic blood pressures of less than 85 mmHg.. When vardenafil 5 mg (filmcoated tablets) was given simultaneously with terazosin 5 or 10 mg, one of 21 patients experienced symptomatic postural hypotension. Hypotension was not observed when vardenafil 5 mg and terazosin administration was separated by 6 hours. When vardenafil (film-coated tablets) was given at doses of 5 or 10 mg on a background of stable therapy with alfuzosin, compared to placebo, there was no symptomatic reduction in blood pressure. Therefore, concomitant treatment should be initiated only if the patient is stable on his alpha-blocker therapy. In those patients who are stable on alpha-blocker therapy, vardenafil should be initiated at Since alpha-blocker monotherapy can cause marked lowering of blood pressure, especially postural hypotension and syncope, interaction studies were conducted with Levitra film-coated tablets [in normotensive volunteers after short-term alpha-blockade and in patients with benign prostatic hyperplasia (BPH) on stable alphablocker therapy]. Hypotension, in some cases symptomatic, was reported in a significant number of subjects after co-administration of Levitra filmcoated tablets to healthy normotensive volunteers forced titrated, over a period of 14 days or less, to high doses of the alphablockers tamsulosin or terazosin. When Levitra film-coated tablets were given at doses of 5 mg, 10 mg or 20 mg on a background of stable therapy with tamsulosin, there was no clinically relevant mean maximal additional reduction in blood pressure. When Levitra 5 mg filmcoated tablets were dosed simultaneously with tamsulosin 0.4 mg, 2 of 21 patients experienced a standing systolic blood pressure <85 mm Hg. When Levitra 5 mg film-coated tablets were dosed 6 hours after tamsulosin administration, 2 of 21 patients experienced a standing systolic blood pressure <85 mm Hg. Among subjects treated with terazosin, hypotension, standing systolic blood pressure <85 mm Hg, was observed more frequently when vardenafil and terazosin were given to achieve Cmax simultaneously than when the doses were administered to separate Cmax by 6 hours. Because these studies were conducted using healthy volunteers, after forced titration of the alpha-blocker to high doses, these studies may have limited clinical relevance. Three interaction studies were conducted with Levitra film-coated tablets in patients with benign prostatic hyperplasia (BPH) on stable alpha-blocker therapy using the lowest recommended starting dose of 5mg. Levitra may be administered at any time with tamsulosin or alfuzosin. With other alpha-blockers a time separation of dosing should be considered when vardenafil is prescribed concomitantly (see section 4.4). alfuzosin, tamsulosin or terazosin. Levitra film-coated tablets, 5 mg or 10 mg, were administered four hours after alfuzosin dosing. The four-hour dosing interval was chosen to elicit the maximum potential interaction. No clinically relevant mean maximal additional reduction in blood pressure was observed over the 10-hour interval following dosing with vardenafil 4 hours after alfuzosin. Two patients, one dosed with Levitra 5 mg filmcoated tablets and the other with Levitra 10 mg film-coated tablets, experienced decreases from baseline in standing systolic blood pressure >30 mm Hg. No instances of standing systolic blood pressure <85 mm Hg were observed during this study. Four patients, one dosed with placebo, two dosed with Levitra 5 mg filmcoated tablets and one dosed with Levitra 10 mg film-coated tablets, reported dizziness. Based on these results no time interval between dosing with alfuzosin and Levitra is required. In a subsequent study in patients with BPH, when Levitra 10 mg and 20 mg film-coated tablets were dosed simultaneously with 0.4 mg or 0.8 mg of tamsulosin no cases of standing systolic blood pressure <85 mm Hg were observed. Based on these results no time interval between dosing with tamsulosin and Levitra is required. When Levitra 5 mg film-coated tablets were dosed simultaneously with 5 mg or 10 mg of terazosin, 1 out of 21 patients experienced symptomatic postural hypotension. Hypotension was not observed when vardenafil was dosed 6 hours after terazosin was administered. This should be considered when deciding about a time separation of dosing between Levitra and terazosin. No cases of syncope in this study or in the earlier alfuzosin or terazosin studies. Concomitant treatment should be initiated only if the patient is stable on his alpha-blocker therapy. In those patients who are stable on alpha-blocker therapy, Levitra should be initiated at the lowest recommended starting dose. Patients treated with alpha-blockers should not use Levitra 10 mg orodispersible tablets to initiate therapy. Levitra may be administered at any time with alfuzosin or tamsulosin. With terazosin and other alpha-blockers an appropriate time interval between dosing should be considered when Levitra is prescribed concomitantly (See section “Special warnings and precautions for use”). No significant interactions were shown when warfarin (25 mg), which is metabolised by CYP2C9, or digoxin (0.375 mg) was co-administered with vardenafil (20 mg film-coated tablets). The relative bioavailability of glibenclamide (3.5 mg) was not affected when co-administered with vardenafil (20 mg). In a specific study, where vardenafil (20 mg) was co-administered with slow release nifedipine (30 mg or 60 mg) in hypertensive patients, there was an additional reduction on supine systolic blood pressure of 6 mmHg and supine diastolic blood pressure of 5 mmHg accompanied with an increase in heart rate of 4 bpm. Lack of pharmacokinetic interaction was shown when Levitra 20 mg film-coated tablets were coadministered to patients receiving 0.375 mg of digoxin, at steady state, every other day for 14 days. There was no evidence that vardenafil pharmacokinetics were altered by co-administration of digoxin. When Levitra 20 mg film-coated tablets were co-administered with 3.5 mg of glibenclamide, Glyburide, the relative bioavailability of glibenclamide was not affected. There was no evidence that vardenafil pharmacokinetics were altered by co-administration of glibenclamide. No pharmacological, e.g. prothrombin time and clotting factor II, VII and X, interaction was shown when 25 mg of warfarin was co-administered with Levitra 20 mg film-coated tablets. Vardenafil pharmacokinetics was not affected by co-administration of warfarin. No relevant pharmacodynamic or pharmacokinetic interaction was shown when Levitra 20 mg filmcoated tablets were coadministered with 30 mg or 60 mg of nifedipine. Compared to placebo, Levitra film-coated tablets produced mean additional blood pressure reductions of 5.9 mm Hg and 5.2 mm Hg for supine systolic and diastolic blood pressure, respectively. Vardenafil (10 mg) did not potentiate the increase in bleeding time caused by acetylsalicylic acid (2 x 81 mg). Levitra 10 mg and 20 mg filmcoated tablets did not influence the bleeding time when taken alone or in combination with low dose acetylsalicylic acid (2 x 81 mg tablets). Undesirable Effects The adverse reactions reported with Levitra film-coated tablets or 10 mg orodispersible tablets in clinical trials were generally transient and mild to moderate in nature. The most commonly reported adverse drug reaction occurring in 10% of patients is headache. Undesirable Effects Tabulated list of adverse reactions All Clinical trials (ADRs) The frequencies of ADRs reported with Levitra are summarized in the table below. Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Frequencies are defined as very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000). The ADRs identified only during post marketing surveillance and for which a frequency could not be estimated, are listed under “not known”. Adverse drug reactions reported in patients in all clinical trials worldwide which are either reported as drug-related in ≥ 0.1% of the patients or rare and considered serious in their nature <critical term according to BSP GPV critical term list> אנא ראה טבלת תופעות לוואי מצורפת Penile haemorrhage, haematospermia and haematuria have been reported in clinical trials and spontaneous postmarketing data with the use of all PDE5 inhibitors, including vardenafil. At a dose of 20 mg Levitra film-coated tablets, elderly ( 65 years old) patients had higher frequencies of headaches (16.2% versus 11.8%) and dizziness (3.7% versus 0.7%) than younger patients (<65 years old). In general, the incidence of adverse reactions (especially “dizziness”) has been shown to be slightly higher in patients with a history of hypertension. Post-marketing reports of another medicinal product of this class Vascular disorders אנא ראה טבלת תופעות לוואי מצורפת Fertility, pregnancy and Lactation Adverse events Serious cardiovascular reactions, including cerebrovascular haemorrhage, sudden cardiac death, transient ischaemic attack, unstable angina and ventricular arrhythmia have been reported post-marketing in temporal association with another medicinal product in this class. . שבו מסומנות ההחמרות המבוקשות על רקע צהוב,מצ"ב העלון יש לסמן רק תוכן מהותי ולא שינויים במיקום.שינויים שאינם בגדר החמרות סומנו (בעלון) בצבע שונה .הטקסט System Organ Class Very common (1/10) Infection and Infestations Immune System Disorders Psychiatric Disorders Nervous System Headache Disorders Common (1/100 to <1/10) Dizziness Eye Disorders Ear and Labyrinth Disorders Cardiac Disorders Vascular Disorders Respiratory, Thoracic and Mediastinal Disorders Gastrointestinal Disorders Hepatobiliary Disorder Skin and Subcutaneous Tissue Disorders Musculoskeletal and Connective Tissue Disorders Flushing Nasal congestion Uncommon (1/1,000 to <1/100) Not Known Rare (can not be (1/10,000 to estimated from the available <1/1,000) data) Conjunctivitis Allergic oedema and angioedema Sleep disorder Allergic reaction Somnolence paraesthesia and dysesthesia Syncope Seizure Amnesia Visual disturbance Ocular hyperaemia Visual colour distortions Eye pain and eye discomfort Photophobia TInnitus Vertigo Increase in intraocular pressure Lacrimation increased Palpitation Tachycardia Myocardial infarction Ventricular tachyarrhythmias Angina pectoris Dyspnoea Sinus congestion Anxiety Sudden deafness Hypotension Hypertension Epistaxis Dyspepsia Gastrooesophageal reflux disease Gastritis Gastointestinal and abdominal pain Diarrhoea Vomiting Nausea Dry mouth Increase in Increase in transaminases gamma-glutamyl transferase Erythema Photosensitivity Rash reaction Back pain Increase in creatine phosphokinase Myalgia Increased muscle tone and cramping Non-arteritic anterior ischemic optic neuropathy Visual defects Renal and urinary disorders Reproductive System and Breast Disorders General Disorders and Administration Site Conditions Haematuria Increase in erection Priapism Feeling unwell Chest pain Penile Haemorrhage Haematospermia לצרכן בעלון לצרכן בטיחות) בעלון מידע בטיחות) החמרה (( מידע על החמרה הודעה על הודעה )).102.50 (מעודכן .102.50 (מעודכן תאריך 213213102. שם תכשיר באנגלית ומספר הרישום Levitra 10mg orodispersible tablets שם בעל הרישום 146-52-33322-01, 146-52-33322-00 טופס זה מיועד לפרוט ההחמרות בלבד ! ההחמרות המבוקשות פרק בעלון טקסט חדש טקסט נוכחי התוויות מתי אין להשתמש בתכשיר? אין להשתמש בתרופה אם הנך נוטל ניטרטים (כגון גליצרול טריניטראט לטיפול באנגינה ,או תורמי ניטריק אוקסיד כגון אמיל ניטריט). אם הנך חווה ירידה בראיה או אובדן ראיה פתאומיים ,הפסק את נטילת לויטרה ופנה לרופא שלך מיד. אזהרות מיוחדות הנוגעות לשימוש בתרופה: אין להשתמש בתרופה מבלי להיוועץ ברופא לפני התחלת הטיפול: תגובות בין תרופותיות: הנך נוטל תרופות המכילות ניטראטים (כגון גליצרול טריניטראט לטיפול באנגינה ,או תורמי ניטריק אוקסיד ( )NOכגון אמיל ניטריט). נטילת תרופות אלה במקביל ללויטרה יכולה להשפיע על לחץ הדם שלך באופן חמור. ניטרטים (כגון גליצרול טריניטראט לטיפול באנגינה ,או תורמי ניטריק אוקסיד כגון אמיל ניטריט), עקב השפעתם המשולבת על לחץ הדם. תרופות לטיפול בנגיף האיידס (כגון אינדינאויר, ריטונאויר); שימוש בתרופה ומזון אין ליטול את התרופה עם מיץ אשכוליות ניטראטים לטיפול באנגינה או תורמי ניטריק אוקסיד כגון אמיל ניטריט עקב ההשפעה החמורה של השילוב שלהם על לחץ הדם – אין ליטול לויטרה. אינדינאויר או ריטונאויר לטיפול בנגיף האיידס – אין ליטול לויטרה. שימוש בתרופה ומזון אל תצרוך מיץ אשכוליות כאשר אתה משתמש בלויטרה ,הצריכה עלולה להפריע להשפעה הסדירה של התרופה. איך תשפיע התרופה על חיי היום יום שלך? השימוש בתרופה זו עלול לגרום לסחרחורת וטשטוש ראייה וכן לפגום בערנות ,על כן מחייב זהירות בנהיגה ברכב ,בהפעלת נהיגה והפעלת מכונות לגרום עלול בלויטרה השימוש לסחרחורת וטשטוש ראייה .אם אתה חש בסחרחורת או אם ראיתך מושפעת לאחר נטילת לויטרה ,אל תנהג ואל תפעיל מכונות או מכשירים. מכונות מסוכנות ובכל פעילות המחייבת ערנות. הריון והנקה: כיצד תשתמש בתרופה: תופעות לוואי: טבליה מסיסה אחת ,כשעה לפני קיום יחסי מין. יש ליטול טבליה מסיסה אחת ,כ 52 -עד 06דקות לפני קיום יחסי מין. תופעות לוואי נדירות מאוד או ששכיחותן אינה ידועה( :יתכן וישפיעו על מטופל אחד מתוך 06666 מטופלים) דם בשתן (המטוריה) דימום מאיבר המין הופעת דם בנוזל הזרע מצ"ב העלון ,שבו מסומנות ההחמרות המבוקשות על רקע צהוב. שינויים שאינם בגדר החמרות סומנו (בעלון) בצבע שונה .יש לסמן רק תוכן מהותי ולא שינויים במיקום הטקסט.