Appendix 1
advertisement

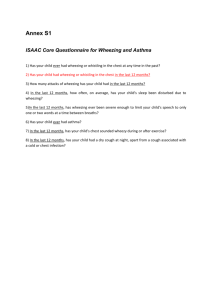
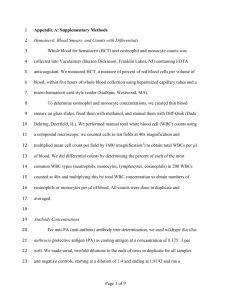
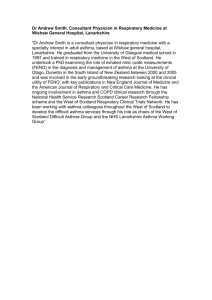
Online Data Supplement Title: Prediction of asthma in symptomatic preschool children using exhaled Nitric Oxide, Rint and specific IgE Authors: Daan Caudri Alet Wijga Maarten O. Hoekstra Marjan Kerkhof Gerard H. Koppelman Bert Brunekreef Henriette A. Smit Johan C. de Jongste Methods Recruitment of participants All children participated in the Prevention and Incidence of Asthma and Mite Allergy (PIAMA) birth cohort study. This multicentre study was conducted in 3 different regions of The Netherlands: north (Groningen and surroundings), central (Bilthoven, Wageningen and surroundings) and southwest (Rotterdam and surroundings). Recruitment took place between March 1996 and May 1997 by means of a validated screening questionnaire,[E1] distributed by midwifes to 10,232 pregnant woman visiting one of 52 prenatal clinics. According to the results of this screening the women were divided in an allergic and a non-allergic group. Women with any of the following self-reported symptoms were defined as allergic: asthma, hay fever, house dust allergy, house dust mite allergy or pet allergy. Children of allergic women were defined as ‘high-risk’. Based on the screening 7,862 women (2,779 allergic and 5,083 non-allergic) were invited to participate in the study, approximately 50% (n=4,146) agreed and gave informed consent (1,327 allergic and 2,819 non-allergic). The PIAMA cohort includes an intervention part, studying the effect of impermeable mattress covers, and a natural history part. Figure E1 shows the flow diagram for recruitment of the intervention and the natural history arm. In the present study we considered children from both the intervention and the natural history part. As previously published, the intervention had no effect on the incidence of allergy or respiratory symptoms.[E2] Furthermore there was no association between the intervention and the measurements of FENO, Rint or specific IgE. At 3 months and 4 years all high-risk children (n=1327) and a subsample of the low-risk children (n=625) would be invited for a medical examination (Figure E1). Eligible for the present study were only children who were invited for the medical examination at 4 years (n=1808) and who, in addition, had a positive response to at least one of the following 3 questions in the questionnaire at age 3 or 4 years: Has your child had wheezing or whistling in the chest in the last 12 months? Has your child had tightness of the chest or shortness of breath in the last 12 months? Has your child had cough during the night, when he/she did not have a cold or a chest infection, in the last 12 months? In total n=848 children fulfilled these criteria and were included in the study population. Data collection: Questionnaires were sent to participating parents for self-completion at the 3rd trimester of pregnancy, 3 months after birth, at the age of 1 and yearly thereafter. The final questionnaire was sent at the age of 8. Information was collected on birth and socioeconomic characteristics; indoor environmental, lifestyle, and demographic factors; and on the child’s health in at every age (e.g. allergies, eczema, respiratory symptoms, doctors’ diagnoses and medication use). FENO Measurement at age 4: Exhaled FENO was measured offline by the balloon method, according to European Respiratory Society/American Thoracic Society guidelines.[E3] Children were asked to take a deep breath through a charcoal NO-scrubber, and to exhale immediately into a collection device employing dynamic flow restriction, using a two-way valve. Exhalation flow was kept constant at 50 mL·s–1 over a pressure range of 5–20 cm H2O. Mouth pressure was monitored during the measurement using a manometer. After discarding dead space air for 3–4 s, exhaled air was collected in a NO impermeable 150 mL Mylar balloon (Jurjen de Vries BV, Leeuwarden, the Netherlands).[E4] For every child, duplicate exhaled air samples and a sample of ambient air were collected. Balloons were sealed, stored and analysed within 8 h with a chemiluminescence analyser. Exhaled FENO is expressed in particles nitric oxide per billion (ppb). In the western and middle areas of the Netherlands, a Sievers NOA 280 analyser (Boulder, CO, USA; sensitivity 0.5 ppb, detection range 0.5– 500.000 ppb, sample flow 200 mL·min–1, sampling rate 4·s–1 (middle), 20·s–1 (western)), was used. In the northern area, an Ecophysics CLD 700 AL analyser (Ecophysics, Basel, Switzerland; sensitivity 1 ppb, detection range 0–50.000 ppb, sample flow rate 700 mL·min–1, data sampling rate 0.5·s–1) was used. A check for systematic differences between the different NO analysers was performed by measuring balloons filled with calibration gas on all analysers on the same day. This analysis revealed a good agreement, with no significant systematic differences between the analysers.[E5] Rint measurement at age 4: Measurements were carried out using the MicroRint (Micro Medical Ltd, Rochester, UK), a portable device including a shutter and pneumotachograph, connected to a palmtop computer with an online display showing mouth pressure, time of shutter closure, Rint values, and the median value of all Rint data recorded during one session. Its software calculates Rint (expressed in kPa.L-1) using the back extrapolation technique to t = 15 ms after shutter closure during 100 ms. A maximum of 10 tracings can be gathered for each measurement. Daily calibrations of pressure and flow (volume) were carried out using a manometer and a 2-L precision pump. All measurements were carried out with a filter (Micro Medical Ltd) in place for reasons of hygiene, and to prevent dysfunction of the pneumotachograph due to any saliva.[E6] Specific IgE measurement at age 4: Specific immunoglobulin E (IgE) to inhalant allergens (house dust mite (Dermatophagoides pteronyssinus), cat, dog, grass (Dactylis glomerata), birch (Betula verrucosa) and mould (Alternaria alternata)) were determined by a Radio Allergo Sorbent Test. Atopy was defined as specific IgE concentration >0.70 IU·mL–1 for at least one inhalant allergen. Statistical Analysis: Logistic regression was used to investigate the relationship between the three measurements (FENO, Rint and specific IgE) and respiratory outcomes assessed at the ages of 5, 6, 7 and 8 years. A longitudinal analyses was then performed, combining information on the outcomes at every age in one model. In this analysis we have to take into account that the repeated measurements in the same individual are correlated, in order to calculate correct standard errors and p-values of our estimates. A Generalized Estimation Equations (GEE) model was used. As correlations between repeated measurements can be expected to depend on the time lag between 2 measurements, a 3-dependent correlation matrix was modelled. Interaction of the measurements with age (as a categorical variable) was included in the GEE model, in order to allow the associations to vary with age. Besides a complete case analysis, a multiple imputed analysis was performed to investigate and correct for any bias that may result from complete case analysis.[E7] The imputed datasets were created following the guidelines as described by van Buuren et al.[E8] Apart from all variables in the final models, the following variables (due to their strong association with the missing data) were used in the imputation matrix: region, urbanisation, parental education, age mother, pregnancy duration, mode of delivery, number of siblings, pet avoidance due to allergy, symptoms of wheeze/dyspnea/eczema, eosinophilic count at age 4, Rint measurements at age 8, total and specific IgE measured at age 8, FENO measured at age 8. The benefit of an imputed analysis depends on two factors: 1) the strength of the association between the imputed variable and variables used for the imputation; and 2) the availability of complete data on these variables used for imputation. In table E1 these data are summarized in two columns for each predictor variable (FeNO/ Rint/ Specific IgE). The first column represents the % of usable cases, which is the proportion of children with missing data on the predictor variable that have data available on the variable used for imputation.[E8] The second column represents the correlation (Spearman’ s coefficient) between the predictor variable and the variable used for imputation, among the children with available data. Using the ‘Multivariate Imputation by Chained Equations’ (MICE) procedure in the statistical program R version 2.6.2, ten imputed datasets with each n=848 subjects were created.[E9, E10] All 10 datasets were analysed using above specified GEE models and results were then combined using PROC MIANALYZE in SAS 9.1 (SAS Institute, Inc., Cary, NC). Results Results from the multiple imputation analyses are reported here. Figure E2 displays the odds ratios of 10log-transformed FENO (per IQR increase) on all outcomes. Odds ratios at different ages were calculated by including an interaction term with age (as a categorical variable) in the model. Compared with complete case analysis none of the associations changed direction, but most associations decreased slightly in strength. Confidence intervals narrowed, which can be explained by the fact that multiple imputation makes it possible to use all available data. All odds ratios that were significant in the complete case analysis remained significant in multiple imputated analysis. Figure E3 gives the odds ratio of Rint (per IQR increase) on all outcomes. There were very little differences between results from complete case and multiple imputation analysis. Figure E4 and gives the odds ratios of a positive specific IgE on all outcomes. Compared with complete case analysis all odds ratios of IgE decrease in strength in the multiple imputed analyses, especially for the outcomes ‘steroid use’ and ‘doctors diagnosis of asthma. This decrease is much more pronounced than for the other 2 tests: FENO and Rint. Again we see that confidence intervals are decreased in the multiple imputed analysis. None of the associations change direction and all odds ratios remain strongly significant. References 1. Lakwijk, N., R. T. Van Strien, G. Doekes, B. Brunekreef, and J. Gerritsen. 1998. Validation of a screening questionnaire for atopy with serum IgE tests in a population of pregnant Dutch women. Clin Exp Allergy 28(4):454-8. 2. Brunekreef, B., R. van Strien, A. Pronk, M. Oldenwening, J. C. de Jongste, A. Wijga, M. Kerkhof, and R. C. Aalberse. 2005. La mano de DIOS...was the PIAMA intervention study intervened upon? Allergy 60(8):1083-6. 3. Baraldi, E., and J. C. de Jongste. 2002. Measurement of exhaled nitric oxide in children, 2001. Eur Respir J 20(1):223-37. 4. Pijnenburg, M. W., E. T. Lissenberg, W. Hofhuis, L. Ghiro, W. C. Ho, W. P. Holland, and J. C. de Jongste. 2002. Exhaled nitric oxide measurements with dynamic flow restriction in children aged 4-8 yrs. Eur Respir J 20(4):919-24. 5. Brussee, J. E., H. A. Smit, M. Kerkhof, L. P. Koopman, A. H. Wijga, D. S. Postma, J. Gerritsen, D. E. Grobbee, B. Brunekreef, and J. C. de Jongste. 2005. Exhaled nitric oxide in 4-year-old children: relationship with asthma and atopy. Eur Respir J 25(3):455-61. 6. Merkus, P. J., J. Y. Mijnsbergen, W. C. Hop, and J. C. de Jongste. 2001. Interrupter resistance in preschool children: measurement characteristics and reference values. Am J Respir Crit Care Med 163(6):1350-5. 7. van der Heijden, G. J., A. R. Donders, T. Stijnen, and K. G. Moons. 2006. Imputation of missing values is superior to complete case analysis and the missingindicator method in multivariable diagnostic research: a clinical example. J Clin Epidemiol 59(10):1102-9. 8. van Buuren, S., H. C. Boshuizen, and D. L. Knook. 1999. Multiple imputation of missing blood pressure covariates in survival analysis. Stat Med 18(6):681-94. 9. S. Van Buuren & C.G.M. Oudshoorn. mice: Multivariate Imputation by Chained Equations. R package version 1.16; 2007. Available from http://web.inter.nl.net/users/S.van.Buuren/mi/hmtl/mice.htm. 10. R Development Core Team (2007). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available from http://www.R-project.org. Figure legends Figure E2. Predictive value of FENO measured at 4 yrs on all outcomes at 5-8 yrs, using multiple imputation analysis Black dots are crude odds ratios for FENO (per IQR increase in 10log(FENO)). *: Open dots are adjusted for clinical history (allergic mother/ doctors diagnosis of eczema/ wheezing at age 4). Figure E3. Predictive value of Rint measured at 4 yrs on all outcomes at 5-8 yrs, using multiple imputation analysis Black dots are crude odds ratios for Rint (per IQR increase). *: Open dots are adjusted for clinical history (allergic mother/ doctors diagnosis of eczema/ wheezing at age 4). Figure E4. Predictive value of specific IgE measured 4 yrs on all outcomes at 58 yrs, using multiple imputation analysis Black dots are crude odds ratios for specific IgE. *: Open dots are adjusted for clinical history (allergic mother/ doctors diagnosis of eczema/ wheezing at age 4). Tables Table E1 Predictor variables Variables used in imputation FeNO at 4 Nmissing Navailable = 542 = 308 % usable r(FeNO) cases Predictor variables FeNO at age 4 n.a. Rint at age 4 44 0.12 Specific IgE at age 4 26 0.22 Model covariates (clinical history) Wheezing frequency at age 4 91 0.05 Atopy of mother 100 0.03 Eczema at age 4 95 0.08 Outcome variables (wheezing/ steroid use/ shortness of breath/ asthma diagnosis) At age 5 90 0.15 At age 6 88 0.14 At age 7 85 0.13 At age 8 84 0.20 Variables related to missingness of predictor variables* Maternal age 100 0.08 Maternal education 98 0.05 Paternal education 95 0.07 Degree of urbanisation 100 0.03 Study region 100 0.11 Presence older siblings 100 0.01 Caesarian section 99 0.05 Pregnancy duration 99 0.13 Eczema siblings 99 <0.01 Variables related to value of predictor variables* Avoidance of allergens indoors 99 0.02 Wheezing age 1 94 0.02 Wheezing age 2 97 0.02 Wheezing age 3 97 0.02 Shortness of breath age 4 92 0.10 Steroid use age 4 89 0.08 Asthma diagnosis age 4 81 0.04 Blood eosinophils at age 4 37 0.23 FeNO measured at age 8 45 0.16 Rint measured at age 8 57 <0.01 Specific IgE measured at age 8 56 0.12 Rint at 4 Nmissing Navailable = 366 = 482 % usable r(Rint) cases Specific IgE at 4 Nmissing Navailable = 447 = 380 % usable r(Specific IgE) cases 16 27 0.12 n.a. 0.05 39 40 - 0.22 0.05 n.a. 89 100 94 0.21 0.05 0.02 91 100 95 0.21 0.03 0.16 89 86 80 81 0.16 0.21 0.18 0.11 89 86 82 82 0.21 0.22 0.30 0.25 100 98 95 100 100 100 99 100 99 0.02 0.02 0.04 0.08 0.09 0.02 0.09 0.06 0.04 100 98 95 100 100 100 99 99 99 0.06 0.05 0.07 0.01 0.01 0.17 <0.01 0.05 0.10 99 95 96 96 90 87 79 25 39 49 47 0.03 0.13 0.12 0.13 0.10 0.14 0.06 0.09 0.01 0.44 0.08 99 94 96 98 91 88 78 0 42 52 46 0.15 <0.01 0.08 0.08 0.13 0.09 0.10 n.a. 0.28 0.10 0.39 At every age the 4 outcome variables (wheezing/ steroid use/ shortness of breath/ asthma diagnosis) all had the same % of usable cases, correlations were also very similar and only the highest value is reported. Note that some variables associated with missingness of one of the predictor variables, were also correlated with the value of a predictor variable. *: Predictor variables are FeNO, Rint and Specific IgE measured at age 4. Figures Figure E1. The Prevention and Incidence of Asthma and Mite Allergy (PIAMA) recruitment scheme. Figure E2. Predictive value of FENO measured at 4 yrs on all outcomes at 5-8 yrs, using multiple imputation analysis 7 5 crude adjusted* Wheezing 2 1 10 Odds Ratio per inter quartile range increase in log (FENO) 3 0.5 5 7 5 6 7 8 Inhaled steroid use 3 2 1 0.5 5 7 5 6 7 8 Doctors' diagnosis asthma 3 2 1 0.5 5 6 7 8 Age, years Figure E3. Predictive value of Rint measured at 4 yrs on all outcomes at 5-8 yrs, using multiple imputation analysis 7 5 crude adjusted* Wheezing 3 Odds Ratio per inter quartile range increase in Rint 2 1 0.5 5 7 5 6 7 8 Inhaled steroid use 3 2 1 0.5 5 7 5 6 7 8 Doctors' diagnosis asthma 3 2 1 0.5 5 6 7 8 Age, years Figure E4. Predictive value of specific IgE measured at 4 yrs on all outcomes at 5-8 yrs, using multiple imputation analysis 40 crude adjusted* Wheezing 20 10 Odds Ratio for specific IgE for inhalent allergens 5 2 1 0.5 5 40 20 6 7 8 Inhaled steroid use 10 5 2 1 0.5 5 40 20 6 7 8 Doctors' diagnosis asthma 10 5 2 1 0.5 5 6 7 8 Age, years