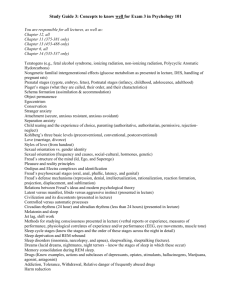
sleep disorders chart
advertisement

Narcolepsy General Symptoms Objective Findings Patho-physiology Epidemiology Interventions Sleep-wake control disorder Excessive daytime sleepiness PSG, MSLT: very short sleep latencies Prevalence - 0.05% (uncommon, but not rare) Symptomatic therapy Cataplexy Sleep-onset REM Selective loss of hypocretin neurons in the lateral hypothalamus Hallucinations Daytime naps with REM activity Reactive gliosis Remains stable Genetics? Familial aggreggation sleep paralysis Onset – 2nd decade Sleepiness: stimulants (methylphenidate, dextroamphetamine, modafinil); scheduled naps Cataplexy: Antidepressants, gammahydroxybutyrate (GHB) Paralysis, hallucinations: 5-HT antidepressants, GHB Insomnia Sleep difficulties despite adequate opportunities Prolonged sleep latency and awakenings, frequent awakenings, impaired daytime performance PSG not routinely indicated (10-15% of insomniacs show normal PSGs) Prolonged sleep latency Poor sleep continuity Circadian rhythm sleep disorders (CRSD) Mismatch between desired slepewake times and circadian rhythm phases Specific time patterns of insomnia and sleepiness Hyperarousal Maintained coscience perception into EEG defined sleep stages Reduced homeostatic drive? Increased high frequency EEG activity during sleep Increased corticolimbic system activity No specific PSG findings Mismatch of endogenous pacemaker and desired sleep-wake hours Endogenous circadian rhythms are abnormal DSPS – difficulty falling asleep and waking up Prevalence of symptoms: 3040% Prevalence of disorder: 5-10% Onset – early adulthood; increases with age Women > men Regularizing sleep-wake schedule Benzo-receptor agonists (BzRA), melatonin receptor agonist, low dose sedating antidepressants, natural remedies (melatonin, valerian) Chronic in 85% of insomnia cases Prevalence is unknown DPSP peaks in adolescence DSPS – early morning exposure to bright light; melatonin in early evening hours ASPS – evening light exposure; morning melatonin Voluntary behavior Behavioral chronotherapy – having DSPS patients go to bed at successively later times until they arrive at “normal” sleep times Abnormal timing of exposure to zeitgebers (light) ASPS – early evening sleepiness and early morning awakening Reducing time in bed Absence of photoreception (enucleated blind pts) Genetics? OSAS (obstructiv e sleep apnea syndrome) Repeated airway closures during sleep Excessive daytime sleepiness Loud snoring, rescucitative snort/gasp Repeated episodes of airflow cessation (apnea) or limitation (hypopnea) lasting >10 seconds Oxygen desaturation Obesity, hypertension Repeated arousals Upper airway “crowding” Continued efforts to breath during apneic period Occlusion of upper airway (velopharynx or hypopharynx) Mechanical factors ( Neurological (impaired hypoglossal reflex, secondary cerebral damage?) Loss of hypoxic drive Prevalence: 4-10% males, 25% females Onset: middle age; stable or progressive Mechanical: Continuous positive airway pressure (CPAP); oral appliances to protrude mandible Surgical: bariatric surgery, uvulopalatopharyngoplasty, maxillomandibular advancement REM sleep behavior disorder (RBD) General Symptoms Objective Findings Patho-physiology Epidemiology Interventions Violent behavior during REM sleep Awaken fully at time of episode Increased muscle activity during REM sleep Brainstem lesion Prevalence – unknown BzRA Lewy body disease Onset – middle age Gabapentin, dopamine agonists Idiopathic Men>Women Exacerbated by certain antidepressants! Vivid recall of storylike drems Stable, mildly progressive Usually occur during 2nd half of night Sleep walking Sleep terrors Abnormal behavior during deep NREM sleep Partial arousal from deep sleep Higher than normal stage 3/4 NREM sleep Limited recall Episodes occur during synchronous delta EEG activity Walking, eating, etc. Usually occur during first half of night PLMD (periodic limb movement disorder) Unpleasant sensations in legs that prevent sleep onset PLMD – periodic jerking movements during sleep Urge to move limbs, accompanied by dysesthesias (creepy crawly) Almost always affects lower legs (Babinskilike response) Immediately but temporarily relieved by movement Diurnal variation – worsens at night Prevalence – 25% during middle childhood; 1% of adults Usually stops by early adolescence BzRA Preemptive awakenings before usual time of sleep terrors Avoiding precipitating factors Precipitated by stress, sleep deprivation, alcohol, medications, physical movement Difficult to awaken RLS (Restless Leg Syndrome) Incomplete state transition disorders (partial arousal, but not complete awakening from NREM sleep) PLMD movements continue into light NREM stages Twitches observed every 20-90 seconds; associated with transient EEG arousals Mild Fe deficiency Secondary form associated with irondeficiency anemia, kidney failure, pregnancy (up to 27%), medications (antidepressant, antipsychotic) Reduction of DA activity in basal ganglia Abnormal Fe metabolism in CNS (need Fe as cofactor for DA synthesis) Genetics? Increased familial aggregation (50%); possible linkage to chromosome 12q DA agonists RLS prevalence: 5-10% Benzodiazapines, opiates Onset - 2nd decade of life; chronic L-dopa