Children with one of two developmental disorders, Autism and
advertisement

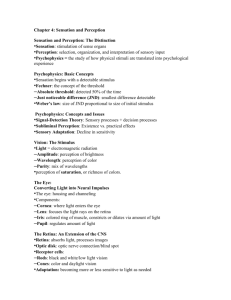
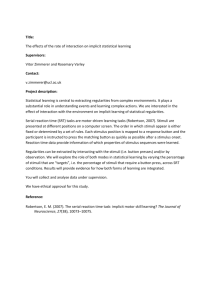
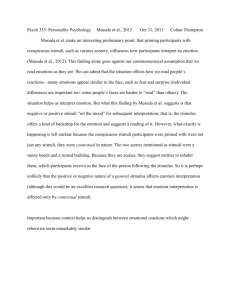
Grice et al. Abnormal of Illusory Contour Perception in WS In press, NeuroReport. ERP Abnormalities of Illusory Contour Perception in Williams Syndrome Sarah J. Grice1&2, Michelle de Haan3, Hanife Halit1, Mark H. Johnson1CA, Gergely Csibra1, Julia Grant2 & Annette Karmiloff-Smith2 1 Centre for Brain and Cognitive Development, School of Psychology, Birkbeck College, University of London 2 Neurocognitive Development Unit, & 3 Developmental Cognitive Neuroscience Unit, Institute of Child Health, London Running title: Abnormal of Illusory Contour Perception in WS CA Corresponding Author Birkbeck College, Malet Street, London WC1E 7HX, United Kingdom e-mail: Mark.Johnson@psych.bbk.ac.uk Tel: +44 207 631 6231, Fax: +44 207 631 6587 1 Grice et al. Abnormal of Illusory Contour Perception in WS 2 Grice et al. Abnormal of Illusory Contour Perception in WS Abstract Williams syndrome is a genetic disorder in which visuo-spatial performance is poor. Theorists have claimed that the deficit lies in high-level processing, leaving low-level visual processes intact. We investigated this claim by examining an aspect of low-level porcessing, perceptual completion, i.e., the ability of this clinical group to perceive illusory Kanizsa squares. We then used event-related potentials to examine neural correlates of perceptual completion. While participants were able to perceive illusory contours, the neural correlates of this apparently normal perception were different from controls. Such differences in low-level visual processes may significantly impact on the development of higher-level visual processes. We conclude that, contrary to earlier claims, there is atypical neural processing during low-level visual perception in Williams syndrome. Keywords: Williams Syndrome; Genetic Disorder; Kanizsa; Subjective figure; ERP; N1 3 Grice et al. Abnormal of Illusory Contour Perception in WS Perceptual completion is important for meaningful processing of visual inputs since objects in the real world are often partially occluded by other objects. Subjective figures have been used to study the properties of the visual system that enable this integrative processing of visual fragments. The Kanizsa Square is a common example of such a stimulus. When the four ‘pacmen’ inducer discs are properly aligned (see Figure 1), people perceive an illusory white square contour with edges occluding four filled circles [1]. The illusory percept is not induced when the pacmen elements are rotated (‘Pacmen’ stimulus, see Figure 1). Behavioural evidence obtained using habituation and preferential looking paradigms suggests that typically developing infants are subject to boundary contour completion from four months of age [2]. The neurophysiological basis of illusory contour perception has been vigorously debated [3]. However, it is now thought that processing of subjective and real contours (e.g., a real square, Figure 1c) takes place in the same visual areas [4,5]. Perception of these contours is a ‘bottom-up’ process, i.e., it is not ordinarily subject to control from higher cortical regions, although it is regulated by complex lateral, feedforward and feedback connections within visual cortex [3]. Converging evidence from a number of neuro-imaging studies utilising functional magnetic imaging (fMRI), positron emission topography (PET) and event-related potential (ERP) techniques suggests that striate (V1) and extra-striate (mainly V2 but also V3 and V4) areas are involved in this process [3-10]. One of the most sensitive and reliable measures of extra-striate processing of illusory contours is the N1 component of the transient visual event-related potential [3]. The N1 component is a negative deflection in the ERP waveform at about 145-180 ms 4 Grice et al. Abnormal of Illusory Contour Perception in WS post-stimulus. It is maximal over bi-lateral occipito-temporal scalp areas and is increased in amplitude for an illusory Kanizsa Square compared to a Pacmen figure or a Real Square. This sensitivity of the N1 component to illusory contours has been documented in a number of studies [3-6]. Williams Syndrome (WS) is a rare developmental disorder caused by microdeletion on chromosome 7 [11]. Characteristics of the disorder have been identified at the physical, behavioural, cognitive, and neurophysiological levels [11-14]. For example, people with WS tend to show poor visuospatial skills but are relatively proficient on face and language processing. It remains unclear why people with WS perform poorly on visuospatial tasks. One suggestion is that early visual processing is ‘intact’, while higher level abilities involved in visual ‘construction’ are impaired [15,16]. An alternative proposal is that individuals with WS employ an unusual perceptual style in that they tend to process visual stimuli more by the parts than the whole [17-19]. Perceptual completion is probably the lowest level visual process through which the parts of a stimulus are seen as a whole. People with WS are subject to perceptual completion when tested using standardised behavioural tests [20]. However, it is unclear whether this process has developed in the normal way at the neural level. It is possible that the apparently normal behaviour of the WS visual system could be subserved by atypical neural mechanisms. If the neural basis of perceptual completion has developed abnormally in WS, then this low-level processing could have a significant influence on the development of higher-level visual processes. Furthermore, if the neural basis of perceptual completion is atypical in WS, then visual perception cannot be legitimately claimed to be ‘intact’ in this population. 5 Grice et al. Abnormal of Illusory Contour Perception in WS The aim of the current study is: 1) to ascertain whether people with WS perceive illusory boundary completion in a behavioural test, and 2) to investigate variations in the amplitude of the N1 ERP component in this clinical population. If early perceptual processes are the same in Williams Syndrome as in controls, then the Kanizsa square should elicit a larger N1 than does the Pacmen stimulus. Alternatively, the neural mechanisms subserving illusory contour perception may have developed differently in Williams Syndrome. If this is the case, then the N1 amplitude may not discriminate between the Kanizsa Square and the Pacmen stimulus. Method Participants: Participants were 15 individuals with WS ranging in age from 10 to 50 years (mean CA: 20.9 (12.2) years), and 15 age and sex-matched controls (mean CA: 21.1 (12.4) years). There were 7 females and 8 males in each group. No participants were excluded from analysis. Stimuli: There were four types of stimuli: 3 experimental stimuli (illustrated in Figure 1) and a set of images of human faces, all presented on a dark grey background of a computer monitor. Each trial started by presenting a small light grey square (fixation stimulus) in the centre for a varying duration of 800-1200 ms, which was then replaced for 307ms by one of the experimental stimuli or a human face. The stimulus offset was followed by a 500-ms-long inter-stimulus interval before the fixation stimulus returned. The faces were presented to maintain participants’ attention. All stimuli measured 3.8 degrees of visual angle (from 75cm distance), and the size of the illusory square produced from the Kanizsa stimulus was the same size as the real 6 Grice et al. Abnormal of Illusory Contour Perception in WS square at 2.3 degrees of visual angle. The four types of stimuli were presented in random order with equal probability (25%). In order to ensure that participants attended to the stimuli, they were instructed to press a button on each presentation of a face. Electrophysiological responses to faces were not analysed. - Figure 1 about here - ERP Procedure: The experiment took place in a dimly lit, sound proofed, and electrically shielded booth. The electroencephalogram (EEG) was recorded using a Geodesic Sensor Net of 128 electrodes [21], against a vertex reference, amplified with a 0.1 to 100-Hz bandpass filtering. Participants were positioned in the sound booth behind a small table on which they were asked to rest their arms. On the table was a button box with one large red and one large blue button. The experimenter explained that the red button should be pressed every time a face appeared on the screen. The hand used to press the button depended on the individual’s preferred use. Participants were asked to practise pressing the button several times without looking down at their hand as they did so. This was mastered immediately by all taking part. A practice session using the same stimuli as the experiment was then carried out with a helper or parent inside the testing booth to instruct and encourage where necessary, until the individual understood the requirements of the task (when they pressed only to all faces and not to other stimuli). This took less than one minute for all participants, except for the youngest male with WS for whom it took approximately four minutes (because he enjoyed pressing the button to every stimulus). The behavioural response accuracy in experimental trials averaged 97% for both groups. ERP data from all practice sessions were discarded. 7 Grice et al. Abnormal of Illusory Contour Perception in WS Stimuli were randomly presented in four mixed stimuli blocks of 110 trials. Between blocks the participant was offered a short break. The recordings from the first 10 trials of each block were discarded. The EEG was digitized at a 250-Hz sampling rate, stored on a computer disk and segmented offline into EEG trials with 200-ms prestimulus and 600-ms post-stimulus onset duration. Movement and electrical artefacts (+ /- 150 microvolts) were identified and rejected by trial-by-trial inspection of the recorded EEG. All participants achieved 24 or more valid artefact-free trials in each condition. ERP analyses: Event-related potentials for each participant were calculated by averaging the time-locked EEG segments within stimulus types. The ERPs were digitally filtered with an elliptical low-pass filter at 30Hz, converted to an average reference and adjusted with reference to a 100-ms-long pre-stimulus baseline. For statistical analyses electrodes were selected in the bi-lateral temporal-occipital areas, illustrated in Figure 2, on the basis of previous studies and the corresponding region of maximal N1 activation in the present study. The amplitude of the N1 component was measured at the peak of the maximal negative deflection within the time window between 108ms and 228 ms for both groups of participants. This window was determined as the range of peak-latency of the N1 component which was identified manually for the same 3 posterior electrodes for each participant. The N1 values measured separately at each electrode were then averaged together to give a single value for both amplitude and latency for each participant. Statistical analyses were carried out on these data using Analysis of Variance, with stimulus (3 levels) as a 8 Grice et al. Abnormal of Illusory Contour Perception in WS within-subject factor and group (2 levels) as a between-subject factor. This analysis was followed up by t-tests where necessary for interpretation. Behavioural Experiment: All participants with WS also took part in a experiment in which the ability to discriminate between the experimental stimuli was tested without recording electrophysiological data. Since the task was very simple, it was assumed that performance would be at ceiling for the normal control participants. The stimuli were exactly the same as those used for the ERP experiment. There were, by necessity, some differences to the procedure. Before the experiment started or instructions had been given, the experimenter displayed a square (different to the experimental stimulus) on the computer screen and asked the participant to identify the shape. The experimenter then displayed a flower and asked the participant ‘is there a square on the screen now?’ All participants correctly answered both questions. Instructions were then given that the computer would display different pictures one at a time and that the participant should say Yes if a square is present, and No if there is no square on the screen. Stimulus presentation was the same as for the ERP experiment, except that the ISI was dependent on a button press by the experimenter. A pilot study indicated that the participants were unable to cope with the demands of pressing the Yes / No buttons themselves. For this reason, the experimenter inputted their verbal response. Reaction-time data were not analysed for this reason. Each participant received 20 trials of each of the 4 experimental stimuli. At the end of the experiment a Kanizsa square stimulus was displayed. The participant was asked whether a square is present, and if so to trace around the square with their finger. - Figure 2 about here - 9 Grice et al. Abnormal of Illusory Contour Perception in WS Results Figure 3 illustrates the ERPs at posterior sites to each stimulus in both groups. In the ANOVA on the N1 amplitude, there was no main effect of group (F(1,28) =.24, P=NS), indicating that N1 activation over all stimuli was not different between the WS and control groups. However, there was a highly significant main effect of stimulus (F(2,56)=12.67, P<.001). Further analysis of this effect showed no difference between the responses to the Kanizsa Square and Pacmen stimuli when the two groups were collapsed (t(29)=1.14, P=NS), but both stimuli elicited a larger N1 amplitude than did the Real Square stimulus (Kanizsa vs. Real Square, t(29)=2.28, P<.05; Pacmen vs. Real Square, t(29)=3.48, P<.05). The prediction based on the hypothesis of abnormal early visual processing in WS was supported by a significant group-by-stimulus interaction (F(2,56)=7.66, P<.001). In the control group, the N1 to the Kanizsa Square was significantly larger than that to the Real Square (t(14) = 2.6, P<.05), which was in turn significantly larger than the N1 to the Pacmen (t(14)=2.53, P<.05) (see Figure 3). By contrast, for the WS group there was no difference between the N1 amplitude elicited to the Kanizsa Square and the Pacmen stimuli (t(14)=.97, P=NS), but the N1 amplitude elicited by both was significantly more negative than that to the Real Square (Kanizsa vs. Real Square, t(14)=2.97, P<.05; Pacmen vs. Real Square, t(14)=1.78, P<.05). There were no significant differences in N1 latency across stimuli (F(1,28) = 1.36, P=NS) or group (F(1,28) =1.46, P=NS), and there was no interaction of stimulus latency with group (F(1,28) =.84, P=NS). -Figure 3 about hereFor the behavioural task, all participants were able to identify a square and reject a non-square. All participants were able to perceive the Kanizsa square and to trace around it with their finger. Two participants were unable to cope with the demands of 10 Grice et al. Abnormal of Illusory Contour Perception in WS the behavioural task, and 1 was unable to take part for other reasons. The average score for the remaining 12 participants was at the ceiling level of 19/20 trials correct (range 15-20 /20 correct) for each of the experimental stimuli. Discussion The results from this study show that while people with Williams Syndrome can perceive illusory contours, the neural mechanisms that support this process are atypical. Despite the fact that the overall size of the N1 response was normal, the differences in amplitude between stimuli were abnormal in WS compared to healthy controls. These data offer only partial support for the oft-cited view that early visual processing is ‘spared’ in the disorder whereas visuomotor construction is impaired (Farran, Jarrold & Gathercole, 2001; Mervis, Robinson, & Pani, 1999), since the neural correlates display functional differences to controls (see also Grice et al. 2001). Our present study contained no ‘construction’ component, yet our clinical participants showed significantly different patterns of cortical activation compared to controls. It is unlikely that visual construction abnormalities over development could have caused the abnormalities in the functioning of these early perceptual mechanisms. Equally, deficits on visuospatial tasks such as drawing and ‘pattern construction’ are unlikely to be caused solely by an impairment in ‘visual construction’ ability. More plausible is our hypothesis that neural mechanisms supporting early perceptual processes are disordered in WS, and that this could have multiple consequences for higher visual processing. One other study has also suggested that perceptual processing in WS may be disordered. Grice et al. (2001) found gross abnormalities of binding-related oscillatory gamma-band activity in adults with WS during perception of faces. The oscillatory 11 Grice et al. Abnormal of Illusory Contour Perception in WS response in the WS group was abnormal in that it was not modulated by differences in the orientation of the face. In addition, the gamma-band activity was disorganised and ‘smeared’ in a manner similar to that found by Csibra et al. [22] in very young infants before organised, adult-like gamma-bursting appears at around 8 months of age. Recent research has suggested that gamma-band integration processes may be modulated by top-down cortical control. Our current data provide further evidence that processes involved in perceptual integration are atypical in WS. However, the atypical N1 response is likely to reflect abnormalities at the bottom-up sensory level associated with extra-striate visual processing mechanisms. There are other possible explanations for the lack of difference between the N1 amplitudes to Kanizsa Square and Pacmen stimuli in the WS group. The most conservative hypothesis is that a possible increase in activity to the Kanizsa Square is too small to be detected at the scalp due to differences in neuroanatomy between WS and control participants. However, this appears unlikely since the overall amplitude of the N1 in WS was normal, and there was a significant difference between the responses to these stimuli and to the Real Square. Alternatively, it may be that the N1 activation to the Kanizsa Square did reflect the encoding of the illusory square in WS, but that the N1 to the Pacmen was enlarged and reaching equal amplitude for a different reason. However, it is difficult to determine a property of the Pacmen stimulus that is not shared with the Kanizsa or Real square. Conclusion Individuals with WS are subject to illusory contour perception. Our behavioural results demonstrate that people with WS can clearly discriminate between the 12 Grice et al. Abnormal of Illusory Contour Perception in WS experimental stimuli, can identify the illusory square and can trace around it with their finger. On the basis of current evidence, however, we conclude that the neural mechanisms underlying early perceptual processing in WS are functionally different from those of typically developing controls, and that this may have downstream consequences for higher-level integration or when demands on the perceptual system are more strenuous than in the current behavioural experiment. An interesting possibility is that the encoding of the illusory square, which enables the successful behavioural performance, happens later in the processing stream in WS than in healthy individuals. The present study provides a first step in establishing the nature of the abnormalities in sensory processing in WS. Our findings conclusively challenge the idea that it is only the later ‘construction’ stages of visual processing that are atypical in this genetic disorder. Rather, we have shown that the neural mechanisms underlying a fundamental early visual process are atypical in Williams Syndrome. Further, we suggest that this abnormality is likely to contribute to previously observed deficits in later visuospatial processing. Acknowledgements We thank the Williams Syndrome Foundation (UK) and the families that participated. Financial support came from the UK Medical Research Council (PhD studentship and Programme Grant Nos. G9715642 and G9715587). 13 Grice et al. Abnormal of Illusory Contour Perception in WS References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Kanizsa G. Scientific American 234, 48-52 (1978). Kavsek MJ. Child Development 73, 331-344 (2002). Proverbio AM and Zani A. Neuropsychologia 40, 479-491 (2002). Kruggel F, Herrmann CS, Wiggins CJ, et al. Neuroimage 14, 1327-1336 (2001). Sugawara M and Morotomi T. Scandinavian Journal of Psychology 32, 352357 (1991). Herrmann CS and Bosch V. Neuroreport 12, 901-904. (2001). Pegna AJ, Khateb A, Murray MM, et al. Neuroreport 13, 965-968 (2002). Lee TS and Nguyen M. Proceeding of the National Academy of Science U S A 98, 1907-1911 (2001). Korshunova SG. Neuroscience Behaviour & Physiology 29, 695-701 (1999). Larsson J, Amunts K, Gulyas B, et al. European Journal of Neuroscience 11, 4024-4036 (1999). Donnai D and Karmiloff-Smith A. American Journal of Medical Genetics 97, 164-171. (2000). Bellugi U, Wang PP and Jernigan TL. In: Broman S and Grafman J, eds. Atypical cognitive deficits in developmental disorders: Implications for brain function. Hillsdale, NJ: Erlbaum, 1994:23-56. Bellugi U, Lichtenberger L, Jones W, et al. Journal of Cognitive Neuroscience 12, 7-29. (2000). Grice SJ, Spratling MW, Karmiloff-Smith A, et al. Neuroreport 12, 26972700 (2001). Farran EK, Jarrold C and Gathercole SE. J Child Psychology, Psychiatry & Allied Disciplines 42, 719-728 (2001). Mervis CB, Robinson BF and Pani JR. American Journal of Human Genetics 65, 1222-1229. (1999). Bellugi U, Sabo H and Vaid J. In: Stiles - Davis J, Kritchevsky M and Bellugi U, eds. Spatial Cognition: Brain bases and development. Hillsdale, NJ: Lawrence Erlbaum Associates, 1988. Deruelle C, Mancini J, Livet MO, et al. Brain & Cognition 41, 276-298. (1999). Karmiloff-Smith A. Trends in Cognitive Sciences 2, 389 - 398 (1998). Wang PP, Doherty S, Rourke SB, et al. Brain & Cognition 29, 54-65 (1995). Tucker D. Electro encephalography and Clinical Neurophysiology 87, 154163 (1993). Csibra G, Davis G, Spratling MW, et al. Science 290, 1582-1585 (2000). 14 Grice et al. Abnormal of Illusory Contour Perception in WS Figure Legends Figure 1: The three experimental stimuli used for both behavioural and ERP experiments. See text for description. Figure 2: A schematic showing the scalp locations of the bi-lateral occipital and temporal sites selected for ERP analysis. Figure 3: The grand average ERP waveforms to the three stimuli averaged over bilateral occipito-temporal scalp areas. 15