title - UMPA
advertisement

TITLE
A mathematical model of ion movements in grey matter
during a stroke
AUTHORS
Marie-Aimée Dronnea,*, Jean-Pierre Boissela and Emmanuel Grenierb
AFFILIATION
a
Service de Pharmacologie Clinique, EA 3736, Faculté de Médecine Laennec, Rue Guillaume
Paradin, BP 8071, 69376 LYON cedex 08, France
- Marie-Aimée Dronne: md@upcl.univ-lyon1.fr
- Jean-Pierre Boissel: jpb@upcl.univ-lyon1.fr
b
Unité de Mathématiques Pures et Appliquées, Ecole Normale Supérieure, 46 allée d’Italie,
69364 LYON, France
Emmanuel.GRENIER@umpa.ens-lyon.fr
RUNNING HEAD
Modelling of ion movements during a stroke
CONTACT INFORMATION
* Corresponding author: Marie-Aimée Dronne
1
Address: Service de Pharmacologie Clinique, EA 3736, Faculté de Médecine Laënnec, Rue
Guillaume Paradin, BP 8071, 69376 LYON cedex 08, FRANCE
e-mail: md@upcl.univ-lyon1.fr
phone number: (33) 4 78 78 57 83
fax number: (33) 4 78 77 69 17
KEY WORDS
Mathematical model, ionic currents, ischaemia, stroke
ABSTRACT
The development of cytotoxic oedema during a stroke consists in cell swelling and shrinking of
the extracellular space. This phenomenon is triggered by ion movements through voltage-gated
channels, exchangers and pumps. During ischaemia, sodium, calcium and chloride enter the
neurons whereas potassium and glutamate are expelled out of the cells. A mathematical model is
proposed to represent the dynamics of membrane potentials, cell volumes and ionic
concentrations in intracellular and extracellular spaces during a stroke and to study the influence
of each ionic current on cell swelling. The model relies on electrophysiological mechanisms and
takes into account the behaviour of two types of cells: neurons and also astrocytes known to play
a key role in the excitotoxic process in grey matter. The results obtained when a severe or a
moderate ischaemia is simulated are consistent with those observed in the in vitro and in vivo
experiments. As this model appears to be robust, it is used to perform illustrative simulations
aimed at studying the effect of some channel blockers on cell swelling. This approach may help
to explore new therapeutic strategies in order to reduce stroke damage.
2
Introduction
Cytotoxic oedema is one of the main pathophysiological phenomena observed in stroke. It
implies the swelling of brain cells such as neurons, astrocytes and oligodendrocytes and results
in the decrease of the extracellular volume. This phenomenon develops within a few minutes
after brain artery occlusion and is responsible for the evolution of brain cells towards necrosis.
When a brain vessel is occluded, the surrounding tissues receive less oxygen and glucose. So,
ATP production drops, which results in a decrease of the activity of ATPases such as the Na+/K+
ATPases (Kato and Kogure, 1999). As these pumps are no longer able to prevent sodium from
accumulating in intracellular space, sodium concentration increases in the neurons. The
alteration of sodium gradient is responsible for the reversal of Na+/Ca2+ exchangers which
contributes to the increase in neuronal calcium concentration (Lee et al., 1999). Another
consequence of the drop in the activity of Na+/K+ ATPases is the increase in extracellular
potassium concentration. The alteration of potassium gradient leads to membrane depolarisation,
which triggers the opening of sodium, calcium, and potassium voltage-gated channels,
contributing to the increase in sodium and calcium concentrations in the neurons and to the
increase in potassium concentration in the extracellular space (Barber et al., 2001).
These ion movements are associated with a fast passive influx of water which tends to restore
the osmotic equilibrium and results in cell swelling (Dirnagl et al., 1999). The usual marker used
to evaluate cell swelling is the Apparent Diffusion Coefficient of water (ADCw) that can be
measured by diffusion-weighed imaging.
The development of cytotoxic oedema during stroke is also due to the excessive release of
glutamate in the extracellular space resulting from the ionic gradient changes induced by
ischaemia. In physiological conditions, the excess of extracellular glutamate can be carried in
the cell by a glutamate transporter using sodium and potassium gradients. But, as these gradients
3
are altered during ischaemia, the glutamate transporter is “reversed” and is responsible for an
efflux of glutamate (Nicholls and Attwell, 1990). The extracellular glutamate triggers the
activation of NMDA, AMPA and metabotropic receptors (Barber et al., 2001). Glutamate is
considered as a crucial factor in the excitotoxic process (Dirnagl et al., 1999).
The aim of our model is to reproduce the ion movements and cell swelling over one hour of
stroke and to study the role of the main neuronal and astrocytic channels, exchangers and pumps
involved in these phenomena. Studying the influence of these carriers on the development of
cytotoxic oedema is of major importance to explore those which could be interesting targets for
therapeutic agents.
This model was built according an approach described in a previous publication (Dronne et al.,
2004). It is a mechanistic model which relies mainly on electrophysiological mechanisms. As
some other electrophysiological models, it includes the intracellular and extracellular volumes as
variables (Shapiro, 2001; Yi et al., 2003). Moreover, we modelled the behaviour of two types of
cells (neurons and astrocytes) during ischaemia. One of the main aims of our model is to study
neuron survival during ischaemia. But, as the surrounding astrocytes are also vulnerable to
ischaemia, they contribute to the ionic concentration changes and to the decrease of extracellular
volume. So, it seems important to include astrocyte behaviour in such a model to improve the
representation of the development of cytotoxic oedema in stroke.
First, we describe the mathematical equations used in the model. Then, we present some results
obtained by the simulation of the development of cytotoxic oedema first during severe
ischaemia and secondly during moderate ischaemia. We study the robustness of the model,
explore the effect of some channel blockers and finish with a discussion about the properties of
the model and its limitations.
4
Mathematical model
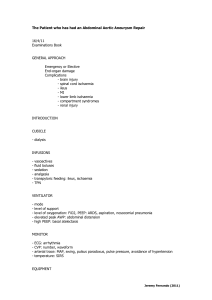
- Three compartments are considered in this model (fig. 1): the first one represents the intraneuronal space, the second one the intra-glial space and the third one the extracellular space. As
astrocytes have been reported to be the most important glial cells in grey matter, all glial cells
are assumed to behave like astrocytes in our model. So, the intra-glial compartment is
considered to be an intra-astrocytic compartment. We also make the hypothesis that the system
containing these three compartments is a closed system in which the volumes of the intracellular
spaces and extracellular space can vary but in which the global volume remains constant.
- The ionic species studied in this model are Na+, K+, Ca2+, Cl- and the glutamate ionised form.
These ions are supposed to be the main species involved in cell membrane potential, ionic
concentration and cell volume changes during ischaemia.
- Ion movements are modelled by the ionic currents through channels, exchangers and pumps.
The model takes into account the carriers needed to maintain cell homeostasis in physiological
conditions and those involved in ion movements during ischaemia. These transporters are
represented on figure 1 and the currents which cross the membranes are collected in table 1.
The model is based on equations that describe the dynamics of cell membrane potentials, the
dynamics of the intracellular and extracellular concentrations and the dynamics of cell volumes.
Membrane potentials are denoted by Vm, concentrations by [Na+], [K+], [Ca2+], [Cl-], [glu] and
cell volume proportions by f, with subscripts “n” for the neuronal space, “a” for the astrocytic
space and “e” for the extracellular space. As the volume (v) of the global system is assumed to
be constant, the neuron volume is Vn (t) v.f n (t) , the astrocyte volume is Va (t) v.f a (t) and
the extracellular volume is Ve (t) v.(1 f n (t) f a (t) )
5
By convention, positive flux terms correspond to outward movement of ions and negative flux
terms correspond to inward movement of ions. Ionic currents are related to ionic fluxes by
equation (1) in which IS represents the current of one ion S and JS the flux of this ion.
I S (t) z.F.J S (t)
(1)
where F is Faraday’s constant and z the ion valence.
So, outward movements of cations are represented by positive currents, inward movements of
cations by negative currents, outward movements of anions by negative currents and inward
movements of anions by positive currents.
Dynamics of cell membrane potentials
According to Kirchoff law, the capacitic current of the membrane equals the sum of all ionic
currents. So, the dynamics of the membrane potentials of neuron and astrocyte are described by
the following equations (equations (2) and (3)):
dVm n (t)
s
n INa n (t) IK n (t) ICa n (t) ICl n (t) Iglu n (t)
dt
Cn
dVm a (t)
s
a INa a (t) IK a (t) ICa a (t) ICl a (t) Iglu a (t)
dt
Ca
(2)
(3)
where C is the membrane capacity (in pF/µm2) and s the cell surface.
In these equations, INa denotes sodium currents, IK potassium currents, ICa calcium currents,
ICl chloride currents and Iglu currents involving glutamate.
These equations are derived from the excess charge equations in intra-neuronal and intraastrocytic spaces (equations (4) and (5)).
C .Vm n (t)
2
[Na ]n (t) [K ]n (t) 2[Ca
]n (t) [Cl ]n (t) [glu ]n (t) [A 0 ]n (t) n
F.v.f n (t)
(4)
C .Vm a (t)
2
[Na ]a (t) [K ]a (t) 2[Ca
]a (t) [Cl ]a (t) [glu ]a (t) [A 0 ]a (t) a
F.v.f a (t)
(5)
6
In these equations, [A0] represents the concentration of the intracellular impermeant anions i.e.
the anions that are not able to pass through the membrane and remain in the intracellular space.
We made the hypothesis that the intracellular ionic concentrations are isotropic.
Equations (4) and (5) describe the fact that the cell membrane behaves like a condenser (of
capacity C) accumulating charges on its faces. We can notice that if we had assumed that the
excess charge was accumulating in a very tiny area near the cell membrane, we could thus have
hypothesised the electric neutrality of the intracellular compartments and used the following
equations (equations (6) and (7)):
2
[Na ]n (t) [K ]n (t) 2[Ca
]n (t) [Cl ]n (t) [glu ]n (t) [A 0 ]n (t) 0
(6)
2
[Na ]a (t) [K ]a (t) 2[Ca
]a (t) [Cl ]a (t) [glu ]a (t) [A 0 ]a (t) 0
(7)
This approximation is often used in models which focus on short-lasting phenomena such as
action potentials (Endresen et al., 2000). In these models, the volume variations can be neglected
and the chloride anion can be considered as a counter-ion. But, in our model, the precise excess
charge equations must be used to take into account the transport of chloride anion which
contributes to cell swelling.
Dynamics of ionic concentrations
The variation of ion quantity in a compartment is obtained by summing ionic fluxes across the
cell membrane which surrounds this compartment. So, the dynamics of the concentrations of
each ionic species in neuron, astrocyte and extracellular spaces are obtained with the following
equations (equations (8-22)):
df n (t).[K ]n (t) s n IK n (t)
dt
F.v
(8)
7
df n (t).[Na ]n (t) s n INa n (t)
dt
F.v
df n (t).[Ca 2 ]n (t) s n ICa n (t)
dt
2.F.v
df n (t).[Cl ]n (t) s n ICl n (t)
dt
F.v
df n (t).[glu ]n (t) s n Iglu n (t)
dt
F.v
dfa (t).[K ]a (t) sa IK a (t)
dt
F.v
dfa (t).[Na ]a (t) sa INa a (t)
dt
F.v
dfa (t).[Ca 2 ]a (t) sa ICa a (t)
dt
2.F.v
dfa (t).[Cl ]a (t) sa ICl a (t)
dt
F.v
dfa (t).[glu ]a (t) sa Iglu a (t)
dt
F.v
d(1 f n (t) f a (t)).[K ]e (t) s n IK n (t) sa IK a (t)
dt
F.v
d(1 f n (t) f a (t)).[Na ]e (t) s n INa n (t) sa INa a (t)
dt
F.v
2
d(1 f n (t) f a (t)).[Ca
]e (t) s n ICa n (t) sa ICa a (t)
dt
2.F.v
d(1 f n (t) f a (t)).[Cl ]e (t) s n ICl n (t) sa ICl a (t)
dt
F.v
d(1 f n (t) f a (t)).[glu ]e (t) s n Iglu n (t) sa Iglu a (t)
dt
F.v
(9)
(10)
(11)
(12)
(13)
(14)
(15)
(16)
(17)
(18)
(19)
(20)
(21)
(22)
Equations (18-22) express the fact that the variation of ion quantity in extracellular space is
obtained by summing ionic fluxes across neuron and astrocyte membranes.
Equations (8-22) allow the conservation of ion quantities in the system. For each type of ion S,
we have:
d(NS n (t) NS a (t) NS e (t)) df n (t).[S] n (t) dfa (t).[S] a (t) d(1 f n (t) f a (t)).[S] e (t)
0
dt
dt
dt
dt
where NS denotes the quantity of ion S
8
Dynamics of intracellular volumes
As in some other models (Shapiro, 2001), the variation of the proportion of the cell volume is
defined as the variation of the intracellular ion quantity divided by the extracellular
concentration of all ionic species. So, the dynamics of the proportions of neuron and astrocyte
volumes are described by the following equations (equations (23) and (24)):
(23)
(24)
dfn (t) 1 d f n (t).([K ]n (t) [Na ]n (t) [Ca 2 ]n (t) [Cl ]n (t) [glu ]n (t) [A 0 ]n (t) )
*
dt
S0
dt
dfa (t) 1 d f a (t).([K ]a (t) [Na ]a (t) [Ca 2 ]a (t) [Cl ]a (t) [glu ]a (t) [A 0 ]a (t) )
*
dt
S0
dt
where S0 is the sum of the extracellular concentrations in physiological conditions
As the system containing the three compartments is assumed to be a closed system with a
constant volume, S0 is constant over time.
Equations (23) and (24) are derived from equations (25-27) describing the osmotic pressures in
the intracellular and extracellular spaces.
Π n RT. [Na ]n (t) [K ]n (t) [Ca 2 ]n (t) [Cl ]n (t) [glu ]n (t) [A 0 ]n (t)
(25)
Π a RT. [Na ]a (t) [K ]a (t) [Ca 2 ]a (t) [Cl ]a (t) [glu ]a (t) [A 0 ]a (t)
(26)
Π e RT. [Na ]e (t) [K ]e (t) [Ca 2 ]e (t) [Cl ]e (t) [glu ]e (t)
(27)
where represents the osmotic pressure and where R is the universal gas constant and T the
absolute temperature
As the flow of water across cell membranes is almost instantaneous, we assume that the osmotic
pressure in each intracellular space equals the osmotic pressure in the extracellular space at each
time, i.e. Π n Π e and Π a Π e , which leads to equations (23) and (24).
9
The value of the marker rADCw (ration of Apparent Diffusion Coefficient of water), which is
usually used in medical imaging to evaluate cytotoxic oedema, can be related to the proportions
of intracellular volumes. As the rADCw value was shown to be proportional to the extracellular
volume (Verheul et al., 1994) and the extracellular proportion was displayed to have a value of
0.2 in physiological conditions (when rADCw=1) (McBain et al., 1990), rADCw can be
expressed by the following equation:
rADCw 5(1 f n (t) f a (t))
(25)
Description of the ionic currents
The detailed equations are given in the appendix.
Voltage-gated channels
Voltage-gated channels allow ions to cross the cell membrane in the same way as their
gradients. They can be divided into two classes: the transient channels (which transiently open)
and the permanent channels (which remain open over a potential threshold).
As the development of cytotoxic oedema may last from several minutes to one hour, the role of
the transient channels is neglected in our model; this phenomenon is supposed to depend mainly
on the role of the permanent voltage-gated channels.
The permanent voltage-gated channels represented in the model are the potassium delayed
rectifier channel (KDR), the potassium voltage- and Ca2+-dependent channel (BK), the sodium
persistent channel (NaP), the calcium high-voltage-activated channel (CaHVA). These kinds of
channels are found both in neuron membrane and in astrocyte membrane. Each of these channels
represents many channels and can be considered as a “mean” channel.
10
The equations used to describe all four of these channels were extracted from the model of
Yamada et al. (1998) and described by Shapiro (2001). The currents through these channels are
expressed with the Hodgkin-Huxley formulation. According to this formulation, the current of
one ion S is described by equation (26) (Hodgkin and Huxley, 1952):
p
q
IS (t) gS .m (t).h (t).(Vm(t) ES (t))
(26)
In this equation, gS represents the conductance, m the probability for the activating gate to be
open, h the probability for the inactivating gate to be open, Vm the membrane potential and ES
the Nernst potential, defined as :
ES (t)
RT
zF
ln
[S]e (t)
(27)
[S]i (t)
where R is the universal gas constant, T the absolute temperature and F Faraday’s constant
The probabilities for the channel gates to be open are expressed by the following equations:
dm(t)
dt
meq(t) m(t)
tm(t)
dh(t)
and
heq(t) h(t)
dt
(28)
tm(t)
where meq and heq are the steady state gating functions.
As we are studying a long-lasting phenomenon (compared to phenomena such as action
potentials), we use the steady state gating functions (meq and heq) instead of the time-dependent
gating functions (m and h). This simplification is often necessary in models reproducing longlasting phenomena (Yi et al., 2003).
We model the currents of neuronal and astrocytic channels with the same expressions but with
different values of conductances to take into account the characteristics of these two types of
cells. For example, potassium permeability was shown to be larger in astrocyte than in neuron.
This difference of permeability is of major importance as it can explain the fact that the
astrocyte rest potential is 20 mV lower than the neuron rest potential (Vmn = -70 mV and Vma =
-90 mV) (Chvatal et al., 1999).
11
As potassium plays a key role in astrocyte, we also model the current of another potassium
voltage-gated channel in astrocyte: the potassium inward rectifier channel (Kir). The expression
used to describe this current comes from the model of Fox et al. (2002).
Pumps
Pumps (or ATPases) are needed to maintain homeostasis in all types of cells. So, we model both
in neuron and in astrocyte the following pumps: the Na+/K+ pump, the Ca2+ pump and the Clpump. These pumps allow ions to cross cell membrane in the opposite way of their gradients but
they are ATP-consuming. As their functions depend on energy production, they are not able to
maintain cell homeostasis in severe ischaemia. Their failure is the pivotal event leading to cell
death.
The expressions of the currents through these pumps in physiological conditions come from
equations used by Shapiro (2001) and extracted from the model of Lemieux et al. (1992). A
function is introduced in these equations to describe the decrease of ATP production during a
severe ischaemia: [ATP](t) [ATP] max .(0.35) (t/15) where t is measured in minutes. This function,
used in some other models (Yi et al., 2003), has been obtained by fitting Jennings and Reimer’s
data on ATP decline during ischaemia (1991).
So, during severe ischaemia, the currents through each pump are expressed by the following
equation: Ipump i (t) (0.35) (t/15) Ipump p (t) where Ipumpp represents each current through the
pump in physiological conditions.
During moderate ischaemia, the ionic currents through the pumps are supposed to decrease
proportionally to ATP production but also to remain over a functional threshold. So, the currents
through
each
pump
can
be
expressed
Ipump i (t) (p ATP (1 pATP ).(0.35) (t/15)).Ipump p (t)
12
by
the
following
equation:
In this equation, pATP is the proportion of the residual production of ATP (pATP equals 1 in
physiological conditions and 0 in complete ischaemia). We choose p ATP=0.6 to illustrate the
model behaviour during moderate ischaemia.
Exchangers
Exchangers allow ions to cross the cell membrane in the opposite way of their gradients but,
contrary to pumps, they do not use the energy coming from ATP. They use the energy produced
by the movement of ions crossing the membrane in the same way as their gradient. The
exchangers modelled both in the neuronal compartment and in the astrocytic compartment are
the Na+/Ca2+ exchanger, the glutamate transporter and the Cl-/HCO3- exchanger. We also
include in the astrocytic compartment the Na+/K+/Cl- cotransport which plays a major role in
glial cells (Walz, 1992).
-
The Na+/Ca2+ exchanger expels Ca2+ out of the cell by using sodium gradient.
-
The glutamate transporter allows glutamate to enter the cell thanks to sodium and
potassium gradients.
-
The Cl-/HCO3- exchanger uses chloride gradient to expel the HCO3- out of the cell.
-
The Na+/K+/Cl- cotransport allows astrocyte to take up the excess of extracellular K+ in
some pathological conditions (Walz, 1992). This exchanger uses the energy of sodium
and chloride gradients.
The expressions of the currents through these exchangers come mainly from the models of
DiFrancesco and Noble (1985) and Shapiro (2001). To model the currents through the glutamate
transporter, we rely on the characteristics of glutamate uptake and release (during physiological
conditions and during ischaemia) described by several authors (Nicholls and Attwell, 1990;
Rossi et al., 2000; Szatkowski et al., 1990; Takahashi et al., 1997).
13
As concentration gradients are altered during ischaemia, these exchangers and transporters may
function in a reversed way and thus may contribute to cell swelling (Lee et al., 1999).
Channels linked to receptors
Channels linked to receptors allow ions to cross the membrane in the same way as their
gradients when the corresponding ligand is fixed on the receptor.
The main receptors that are known to be activated by the glutamate released in excess in the
extracellular space are the NMDA receptor and the AMPA receptor. As the neuronal NMDA
receptors were shown to be more excitable than the neuronal AMPA receptors during ischaemia,
we only consider the NMDA receptor on the neuron membrane (Barber et al., 2001). Several
authors insist on the fact that there are no effective NMDA receptors on the astrocyte membrane
(Steinhauser and Gallo, 1996; Verkhratsky and Steinhauser, 2000). So, the AMPA receptor is
the only receptor represented in the astrocytic compartment.
- AMPA receptor
The AMPA receptor gates a channel that is permeable to monovalent cations such as Na+ and
K+. Some experiments showed that some of these channels could also be permeable to Ca2+
(Steinhauser and Gallo, 1996). But, as this point is still controversial, we assume that the
channel related to the astrocytic AMPA receptor carries only Na+ and K+. To model the current
of these ions through the channel, the Goldman-Hodgkin-Katz formulation is used. According to
this formulation, the current of one ion S is described by the following equation:
[S] (t).e zFVm(t) RT [S] (t)
i
e
IS (t) PS .
.Vm(t).
zFVm(t)
RT
RT
e
1
2 2
z F
where PS is the membrane permeability for ion S
14
(29)
To model the fact that the channel only opens when glutamate is fixed on the receptor, an
activation function is included in the current. This activation function was described by
Destexhe et al. (1998). It depends on the extracellular concentration of glutamate and on the
membrane potential.
- NMDA receptor
The neuronal NMDA receptor gates a channel that is permeable to monovalent and bivalent
cations such as Na+, K+ and Ca2+.
The ionic currents through this channel are modelled according to the Goldman-Hodgkin-Katz
formulation in which an activation function and a blocking function have been introduced.
These functions were described by Destexhe et al. (1998): the activation function is similar to
that used for the AMPA receptor and the blocking function describes the role of Mg2+ which
prevents the cations from crossing the channel. This blocking function depends on the
magnesium concentration and on the membrane potential since it has been observed that
depolarisation could expel Mg2+ out of the channel.
Extra currents
- Glutamate current
In the model, glutamate is assumed to cross neuron and astrocyte membranes via the glutamate
transporter (described above). This transporter allows the uptake of glutamate in physiological
conditions. But, we also have to model the mechanism that carries glutamate out of the cell in
order to maintain the gradient of glutamate. The major releasing way is due to the fusion of
synaptic vesicles with the cell membrane. As this phenomenon relies on complex mechanisms
involving ATP production and the use of calcium and adhesion molecules, we first decided to
model this release with a phenomenological approach instead of a mechanistic one. This
approach can be accepted in so far as the model is focused on ion movements and cell swelling
15
during ischaemia. Several experiments showed that during ischaemia, glutamate release by
synaptic vesicles stops rapidly whereas glutamate transporter remains active and becomes the
major carrier of glutamate (Wahl et al., 1994). So, according to the objective and the time scale
of our model, only the glutamate transporter needs a mechanistic modelling.
- Chloride current
In the model, chloride is assumed to be carried by the chloride pump, the Cl-/HCO3- exchanger
and the Na+/K+/Cl- cotransport on astrocyte membrane. To express the fact that other chloride
channels and exchangers (such as the K+/Cl- exchanger, the stretch-activated chloride channel)
are involved in cell swelling, a global chloride current is added in the model. The HodgkinHuxley formulation is used to express this current.
Determination of the model parameters
The model includes nineteen non-linear ordinary differential equations which need to be solved
simultaneously. To solve this set of equations, we have to specify the initial values of the
variables and the values of the model parameters. The main parameters are the conductances
which appear in the ionic currents. As twenty-eight ionic currents are considered, twenty-eight
conductances have to be specified.
To determine the initial values of membrane potentials, cell volumes and ionic concentrations in
the three compartments, we use the literature usual values (values given in appendix). But the
determination of the conductance values is more complex. The reported values of channel
conductances vary enormously from one experiment to another. They depend on the species
(rodent, human), the type of cell (neuron, astrocyte), the localisation on the cell (soma, dendrite,
axon) and the experimental conditions (temperature, pH, ionic strength). For instance, in the
hippocampal pyramidal cells, the conductance value of the delayed rectifier channel was shown
16
to be 15 pS/µm2 in the dendrites and 1350 pS/µm2 in the soma. In the Purkinje cells,
measurements indicate 600-900 pS/µm2 for the dendritic conductance and up to 9000 pS/µm2
for the somatic conductance (De Schutter and Bower, 1994; Hoffman et al., 1997; Traub et al.,
1994). To cope with the wide variability of the conductance values reported in the literature, we
apply the following procedure:
-
First of all, the twenty-eight conductances have to be chosen to obtain a fixpoint at t=0.
This condition is realised when the neuronal and the astrocytic currents of each of the
five ionic species are null. So, the twenty-eight conductances have to verify ten
constraints. Therefore, eighteen conductance values are chosen at random within their
physiological ranges and the values of the ten conductances left are calculated to obtain a
fixpoint at t=0. Then, these calculated values are tested to know whether they are
contained in their physiological ranges or not.
-
Then, the fixpoint stability is tested. The fixpoint is supposed to be stable when all the
variables return to their initial values after simulating a stimulus in the model.
-
The aim of the third test is to check whether the cell membranes depolarise when the
pumps are stopped.
The first and second conditions have to be respected to reflect the behaviour of neurons and
astrocytes in physiological conditions. The third point has to be positive to be consistent with the
behaviour of these cells during ischaemia.
If all of these conditions are respected, the set of conductance values is stored and used to solve
the differential equation set. We perform this procedure several times and compare the results
obtained with different conductance sets (results shown in the next section).
Results
17
Simulation of the development of cytotoxic oedema during severe ischaemia
We present the dynamics of the main variables of the model: the membrane potentials, the ionic
concentrations and the cell volumes over one hour of severe ischaemia. These results were
obtained with the following conductance set:
{ngKDR, ngBK, ngNaP, ngCaHVA, nrNaK, nrCa, nrCl, ngNaCa, ngtrg, ngClexch, nPK,
ngCldiff, nggludiff, agKDR, agBK, agKir, agNaP, agCaHVA, arNaK, arCa, arCl, agNaCa,
agtrg, agClexch, agastro, aPK, agCldiff, aggludiff} = {2725.181, 3.367, 2.233, 18.895, 13.632,
5.000, 20.000, 1.839, 0.023, 0.289, 0.021, 0.032, 0.012, 65955.315, 0.659, 5.909, 0.001,
165.080, 5.962, 5.000, 20.000, 1.784, 0.029, 5.169, 0.398, 0.001, 0.019, 0.019} (in pS/µm2)
Dynamics of cell potentials
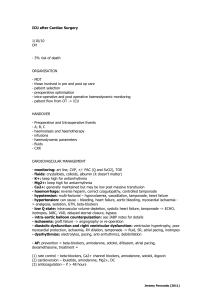
Figure 2 shows that neuron and astrocyte membranes tend towards a complete depolarisation in
severe ischaemia. This depolarisation is due to the fact that, in severe ischaemia, pumps are no
longer able to carry ions in the opposite way of their gradients. Moreover, even if some active
carriers are not affected by the drop in ATP production (such as the Na+/Ca2+ exchanger and the
glutamate transporter) and remain effective during ischaemia, their influences are limited
compared to those of the passive carriers. As a consequence, during a severe ischaemia, ions
cross the cell membranes mainly through the passive carriers (such as the voltage-gated
channels) until there is an equilibrium between intracellular and extracellular concentrations. So,
the Nernst potentials become null (according to equation (27)) and, as the concentrations and the
volumes stop varying, the sums of the currents of each ionic species become null (according to
equations (8)-(22)). If we consider that each current can be approximated by a Hodgkin-Huxley
formulation (equation (26)), we can deduce that the membrane potentials tend to zero.
18
Dynamics of ionic concentrations
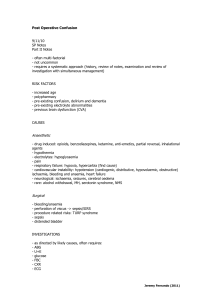
The dynamics of neuronal and extracellular concentrations are represented on figure 3.
- In our simulations, [K+]e increases up to around 100 mM ten minutes after the vessel occlusion.
This value is very similar to the experimental data of Hansen (1978) which show an increase of
[K+]e up to 90 mM four minutes after the brain ischaemia onset. This increase is known to result
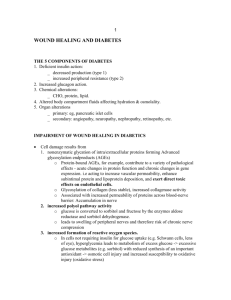
from the efflux of potassium through potassium voltage-gated channels. Our results show that
potassium is released from the neuron first through the BK channel then through the KDR
channel which appears to be the major potassium carrier during severe ischaemia (fig. 4). The
simulated potassium currents through astrocytic voltage-gated channels are larger than those
through neuronal voltage-gated channels (figure not shown). This result is consistent with the
fact that potassium permeability is larger in astrocytes than in neurons (Silver et al., 1997).
- The simulated dynamics of sodium displays an increase of the neuronal concentration from 18
mM to 40 mM (fig. 3). The simulations presented on figure 4 show that, in severe ischaemia,
sodium enters the neurons first through the NaP voltage-gated channel and the Na+/Ca2+
exchanger then through the NaP channel and the receptor-channel NMDA. This latter channel
opens because of the increase of glutamate concentration in the extracellular space (fig. 3). In
several in vitro experiments, the NaP channel was shown to be strongly involved in the influx of
sodium during ischaemia (LoPachin et al., 2001).
- In our simulations, [Ca2+]n increases from 0.0006 mM to 0.4 mM (fig. 3). This increase has
been observed in many experiments on ischemic neuronal tissues (Dirnagl et al., 1999; Lee et
al., 1999). It is one of the main consequences of the excitotoxic process. An excess of calcium
concentration in the intracellular space leads the cell towards necrosis.
The simulated dynamics of calcium is slower than those of the other ions (fig. 3): [Ca2+]n
reaches its maximum ten minutes after the occlusion whereas [Na+]n and [Cl-]n reach their
19
maxima five minutes after the occlusion. The calcium influx follows the movements of the other
species such as Na+ and glutamate (Silver et al., 1997). At the stroke onset, there is an
equilibrium between the influx of calcium through the CaHVA voltage-gated channel and the
efflux of calcium carried by the Na+/Ca2+ exchanger (fig. 4). Then, as sodium gradient is altered
during ischaemia, the activity of the exchanger tends to be reversed. Thus, the calcium influx
overcomes the calcium efflux. Besides, as the glutamate concentration increases in the
extracellular space, it triggers the opening of the channels linked to NMDA receptors. These
channels allow calcium to enter the cell, which contributes to the increase in calcium
concentration in the intracellular space. The effect of NMDA receptor activation on the
accumulation of intracellular calcium is well known and was described by many authors
(Kumura et al., 1999; Rossi et al., 2000).
- Our results show that glutamate concentration increases in the extracellular space from 0.001
mM to 2.5 mM (fig. 3). This excessive release of glutamate in the extracellular space is the
major feature of the excitotoxic process. Glutamate is known to be an excitatory molecule that
triggers the activation of the surrounding cells via glutamate receptors such as the NMDA and
AMPA receptors (Barber et al., 2001). In physiological conditions, the release of glutamate by
synaptic vesicles is balanced by the uptake of glutamate by the glutamate transporter. But, when
a severe ischaemia is simulated, we observe that this carrier contributes to the excessive release
of glutamate (fig. 4). Glutamate transporter reversal is caused by the alteration of potassium and
sodium gradients. Several experiments displayed the deleterious role of this transporter during
ischaemia (Rossi et al., 2000; Wahl et al., 1994).
- The simulated dynamics of chloride shows that intracellular concentration increases from 14
mM to 27 mM (fig. 3). This increase is due to the fact that anions tend to maintain electric
neutrality in the cell.
Dynamics of cell volumes
20
When a severe ischaemia is simulated, the volumes of neurons and astrocytes increase and the
extracellular volume drops by 50% (figure not shown). This value is consistent with the results
of the experiments which displayed that the extracellular space can be half decreased in the most
infarcted areas (Berry et al., 1998).
The dynamics of the extracellular volume is usually represented by the dynamics of the
biomarker rADCw (fig. 5). The results of the simulations display that rADCw tends to the value
0.5 one hour after vessel occlusion. Some experimental results obtained with MRI in human
brain during a stroke also showed that rADCw could decrease down to a value between 0.5 and
0.6 (Rohl et al., 2001). Some authors characterised the infarcted area as an area where rADCw
value is below 0.75 (Desmond et al., 2001).
Simulation of the development of cytotoxic oedema during moderate ischaemia
To study the differences between the dynamics of the variables in severe and in moderate
ischaemia, the same conductance set is used in the equations.
When a moderate ischaemia is simulated, the membrane potentials depolarise up to -20 mV (fig.
2) and rADCw tends to 0.8 (fig. 5). These dynamics are consistent with the features of
penumbra. In stroke, penumbra has been defined as an area of moderate ischaemia that can
recover thanks to spontaneous reperfusion or therapy. Some authors characterised the penumbra
as an area where rADCw value is between 0.75 and 0.9 (Desmond et al., 2001).
Study of the model robustness
The previous results have been obtained with one set of conductances referred to as S*={g1*,…,
gj*,…, g28*} (their values are given in the first section of the results). To take into account the
variability of the conductance values reported in the literature, we consider that each of these
21
values can vary within a wide interval Ij=[gj*-0.9gj*; gj*+0.9gj*]. The conductance values are
chosen at random within these intervals and each set of conductances is studied according to the
procedure described in the fifth section of the model description. Out of 1000 sets of
conductances chosen at random, 446 passed the stages of stability and depolarisation. These 446
sets are used to evaluate the distribution of the variables and to study how the results are
influenced by the sets of conductances. The model robustness is studied both in severe
ischaemia and in moderate ischaemia.
On figure 6, the results obtained in severe ischaemia show that 83% of the neuronal potential
values are between -0.035 and 0.005 mV, 80% of the extracellular potassium concentration
values are between 105.5 and 106.5 mM and 78% of the neuronal potassium concentration
values are between 105.5 and 106.5 mM. For rADCw, 76% of the values are between 0.4 and
0.6. We can also notice that the results obtained with the conductance set S* are very close to
the mean values of these distributions. This study displays that the results obtained in severe
ischaemia are not strongly affected by the set of conductances.
The study of the distributions of the main variables in moderate ischaemia gives similar results
and leads to the same conclusion: most of the conductance sets imply the same model behaviour
(figures not shown).
So, the model appears to be robust either when a severe ischaemia is simulated or when a
moderate one is simulated. As a consequence, our simulations are performed with the
conductance set S* which is representative of all the conductance sets.
Effects of channel blockers
22
To study whether a conductance has an important role in cytotoxic oedema development, we
make this conductance tend to zero. By decreasing the conductance to zero, we simulate the
effect of blocking the corresponding channel.
Figure 7 shows the dynamics of rADCw over one hour of moderate ischaemia when the NaP
channels are blocked 20 minutes after vessel occlusion. This result displays the increase of
rADCw after the blocking of NaP channels. To know if there is some difference in NaP channel
behaviour according to the degree of ischaemia, the values of rADCw after one hour of
occlusion are calculated according to the residual ATP production (fig. 8). On this figure, we
observe that whatever the degree of ischaemia, rADCw is increased when the NaP channels are
blocked. So, gNaP can be said to contribute to cytotoxic oedema development. The effect of
gKDR is represented on figure 9. On this figure, rADCw decreases when the KDR channels are
blocked, whatever the degree of ischaemia. So, gKDR can be considered to contribute to prevent
cytotoxic oedema development.
Table 2 presents the effect of each type of conductance on cell swelling: gKDR has a protective
effect whereas gBK and gKir have nearly no effect. As well as gNaP, the conductances
gCaHVA, gNaCa, gastro and PK have deleterious effects. Our results also show that gtrg tends
to prevent cell swelling in moderate ischaemia and to emphasize this phenomenon in severe
ischaemia. This is due to the complex role of the glutamate transporter which is able to take up
glutamate when there is a moderate increase of glutamate in the extracellular space but which
contributes to release glutamate when this increase is in excess.
Discussion
As cytotoxic oedema is one of the main phenomena which lead the cells toward necrosis during
the first hour of stroke, it is important to better understand the mechanisms involved in this
23
phenomenon and to study the roles of the ionic currents on cell swelling in order to explore new
potential therapeutic pathways during a stroke.
We built a mathematical model to simulate the main mechanisms involved in cytotoxic oedema
development. This model is based on the classical electrophysiological properties but, contrary
to most of the electrophysiological models, it allows cell volumes to vary. Moreover, two types
of cells are taken into account: neurons and astrocytes. Astrocytes are generally neglected in the
models, but they play a key role in the excitotoxic process and they contribute to the decrease in
extracellular volume during stroke (Anderson et al., 2003).
First of all, this model was built with respect to the fundamental physical and chemical
properties such as quantity conservation, osmotic equilibrium and excess charge properties in
intracellular and extracellular spaces. Moreover, it was shown to be robust: the results of the
simulations are slightly depending on the parameter set chosen to solve the model equations.
This model can be used to represent the dynamics of membrane potentials, ionic concentrations
(in intracellular and extracellular spaces) and cell volumes over one hour after vessel occlusion
both in severe and moderate ischaemia. So, with this model, we are able to distinguish the
features of the infarcted area and those of the penumbra. Penumbra is defined as an area of
moderate ischaemia which can recover thanks to reperfusion or therapy whereas the infarcted
area is considered as an area of necrotic cells. The aim of the main therapeutic strategies is to
make penumbra evolve towards recovery in order to limit stroke consequences such as paralysis.
If we simulate a severe ischaemia, we observe that [K+]e increases up to 100 mM and that
[Na+]n, [Ca2+]n and [Cl-]n increase up to respectively 40 mM, 0.4 mM and 27 mM. When a
moderate ischaemia is simulated, these extracellular and neuronal concentrations also tend to
24
rise but with smaller amplitudes. These results are consistent with the data of several in vitro
experiments (LoPachin et al., 2001; Silver et al., 1997). The simulated dynamics of cell
potentials display that cell membranes depolarise up to 0 mV during severe ischaemia and up to
-20 mV during moderate ischaemia. This value was observed in some animal experiments and
used in models representing the occurrence of spreading depressions in penumbra (Kager et al.,
2000). The decrease of the value of rADCw represents the decrease in extracellular volume due
to cell swelling. The simulations show that, one hour after vessel occlusion, rADCw reaches 0.5
when ischaemia is severe and tends to 0.8 when ischaemia is moderate. These results are
consistent with some results obtained with diffusion-weighed imaging, such as those of
Desmond et al. (2001) who observed that the rADCw value is less than 0.75 in the infarcted area
and between 0.75 and 0.9 in the penumbra.
This model helps to better understand the role of each ionic current in the dynamics of ionic
concentrations and in cell swelling during stroke. The simulations of vessel occlusion display
that potassium efflux is mainly due to the KDR channel while sodium enters the cell through the
NaP channel, the Na+/Ca2+ exchanger and the channel of the NMDA receptor. The main carriers
involved in the simulated influx of calcium are the CaHVA channel and the channel of the
NMDA receptor. We also observed an efflux of glutamate due to the reversal of the glutamate
transporter.
Then, the influence of each current conductance on cell swelling was studied to select the
carriers which can be considered as potential therapeutic targets. Our results show that gNaP,
gCaHVA, PK, gNaCa and gastro contribute to the development of cytotoxic oedema whereas
gKDR tends to prevent cell swelling. So, the selective block of NaP channels, CaHVA channels,
25
NMDA receptors, Na+/Ca2+ exchanger or Na+/K+/Cl- cotransport could be considered as
interesting therapeutic pathways. Some of these selective blockers have already been tested in
stroke. Fosphenytoin, which blocks the sodium voltage-gated channels, was shown to allow the
penumbra to recover in rodent but was not effective in man. Similarly, some blockers of the
calcium voltage-gated channels, such as Nimodipine (VENUS, Horn et al., 2001) and
Flunarizine (FIST, Franke et al., 1996) gave encouraging results in animal but disappointing
results in man. Some antagonists of the NMDA receptors such as Selfotel (Morris et al., 1999)
and Aptiganel (Albers et al., 2001) were also tested but all the phase-III trials had to be
abandoned because of the lack of efficacy and the occurrence of side effects. Such mathematical
models can help to explore other therapeutic targets in order to contribute to the development of
new neuroprotective drugs in stroke.
However, the predictive role of the model has to be tempered by its limitations which are due to
the assumptions used to build the model. First, we have focused the model on ion movements in
grey matter whereas stroke generally affects both grey matter and white matter. The modelling
of the development of cytotoxic oedema in white matter will be discussed in a forthcoming
publication.
In this model, the diffusion of ionic species has not been taken into account. However, ions are
able to diffuse in the extracellular space and from an astrocyte to another through astrocyte gapjunctions (Lin, 2002). We can suppose that, if we had included these diffusion phenomena in the
model, the dynamics of ionic concentrations and cell volumes would have been qualitatively
similar to those previously described but quantitatively smaller. This point is currently being
studied.
26
In this model, we represent the main neuronal and astrocytic channels, exchangers and pumps
that maintain cell homeostasis in physiological conditions and that are responsible for ion
movements in ischaemia. But many other carriers are present on neuron and astrocyte membrane
and some of them might also have an influence on cell swelling.
This work was supported by the French Ministry of Research (ACI “AVC-iSi”, project
N°02TS041).
REFERENCES
Albers, G.W., Goldstein, L.B., Hall, D., Lesko, L.M., 2001. Aptiganel hydrochloride in acute
ischemic stroke: a randomized controlled trial. Jama. 286 (21), 2673-2682.
Anderson, M.F., Blomstrand, F., Blomstrand, C., Eriksson, P.S., Nilsson, M., 2003. Astrocytes
and stroke: networking for survival? Neurochem Res. 28 (2), 293-305.
Barber, P.A., Auer, R.N., Buchan, A.M., Sutherland, G.R., 2001. Understanding and managing
ischemic stroke. Can J Physiol Pharmacol. 79 (3), 283-296.
Berry, I., Ranjeva, J.P., Duthil, P., Manelfe, C., 1998. Diffusion and perfusion MRI,
measurements of acute stroke events and outcome: present practice and future hope.
Cerebrovasc Dis. 8 Suppl 2 8-16.
Chvatal, A., Anderova, M., Ziak, D., Sykova, E., 1999. Glial depolarization evokes a larger
potassium accumulation around oligodendrocytes than around astrocytes in gray matter of rat
spinal cord slices. J Neurosci Res. 56 (5), 493-505.
De Schutter, E., Bower, J.M., 1994. An active membrane model of the cerebellar Purkinje cell.
I. Simulation of current clamps in slice. J Neurophysiol. 71 (1), 375-400.
27
Desmond, P.M., Lovell, A.C., Rawlinson, A.A., Parsons, M.W., Barber, P.A., Yang, Q., Li, T.,
Darby, D.G., Gerraty, R.P., Davis, S.M., Tress, B.M., 2001. The value of apparent diffusion
coefficient maps in early cerebral ischemia. Am J Neuroradiol. 22 (7), 1260-1267.
Destexhe, A., Mainen, Z. F., Sejnowski, T. J., 1998. Kinetic models of synaptic transmission, in:
Koch, C., Segev, I. (Eds.), Methods in neuronal modeling: from ions to networks, MIT Press,
Cambridge, pp. 1-26.
DiFrancesco, D., Noble, D., 1985. A model of cardiac electrical activity incorporating ionic
pumps and concentration changes. Philos Trans R Soc Lond B Biol Sci. 307 (1133), 353-398.
Dirnagl, U., Iadecola, C., Moskowitz, M.A., 1999. Pathobiology of ischaemic stroke: an
integrated view. Trends Neurosci. 22 (9), 391-397.
Dronne, M.A., Boissel, J.P., Grenier, E., Gilquin, H., Cucherat, M., Hommel, M., Barbier, E.,
Bricca, G., 2004. Mathematical modelling of an ischemic stroke: an integrative approach. Acta
Biotheor. 52 (4), 255-272.
Endresen, L.P., Hall, K., Hoye, J.S., Myrheim, J., 2000. A theory for the membrane potential of
living cells. Eur Biophys J. 29 (2), 90-103.
Fox, J.J., McHarg, J.L., Gilmour, R.F., Jr., 2002. Ionic mechanism of electrical alternans. Am J
Physiol Heart Circ Physiol. 282 (2), H516-530.
Franke, C.L., Palm, R., Dalby, M., Schoonderwaldt, H.C., Hantson, L., Eriksson, B., LangJenssen, L., Smakman, J., 1996. Flunarizine in stroke treatment (FIST): a double-blind, placebocontrolled trial in Scandinavia and the Netherlands. Acta Neurol Scand. 93 (1), 56-60.
Hansen, A.J., 1978. The extracellular potassium concentration in brain cortex following
ischemia in hypo- and hyperglycemic rats. Acta Physiol Scand. 102 (3), 324-329.
Hodgkin, A.L., Huxley, A.F., 1952. A quantitative description of membrane current and its
application to conduction and excitation in nerve. J Physiol. 117 (4), 500-544.
28
Hoffman, D.A., Magee, J.C., Colbert, C.M., Johnston, D., 1997. K+ channel regulation of signal
propagation in dendrites of hippocampal pyramidal neurons. Nature. 387 (6636), 869-875.
Horn, J., de Haan, R.J., Vermeulen, M., Limburg, M., 2001. Very Early Nimodipine Use in
Stroke (VENUS): a randomized, double-blind, placebo-controlled trial. Stroke. 32 (2), 461-465.
Jennings, R.B., Reimer, K.A., Steenbergen, C., 1991. Effect of inhibition of the mitochondrial
ATPase on net myocardial ATP in total ischemia. J Mol Cell Cardiol. 23 (12), 1383-1395.
Kager, H., Wadman, W.J., Somjen, G.G., 2000. Simulated seizures and spreading depression in
a neuron model incorporating interstitial space and ion concentrations. J Neurophysiol. 84 (1),
495-512.
Kato, H., Kogure, K., 1999. Biochemical and molecular characteristics of the brain with
developing cerebral infarction. Cell Mol Neurobiol. 19 (1), 93-108.
Kumura, E., Graf, R., Dohmen, C., Rosner, G., Heiss, W.D., 1999. Breakdown of calcium
homeostasis in relation to tissue depolarization: comparison between gray and white matter
ischemia. J Cereb Blood Flow Metab. 19 (7), 788-793.
Lee, J.M., Zipfel, G.J., Choi, D.W., 1999. The changing landscape of ischaemic brain injury
mechanisms. Nature. 399 (6738 Suppl), A7-14.
Lemieux, D.R., Roberge, F.A., Joly, D., 1992. Modeling the dynamic features of the
electrogenic Na,K pump of cardiac cells. J Theor Biol. 154 (3), 335-358.
LoPachin, R.M., Gaughan, C.L., Lehning, E.J., Weber, M.L., Taylor, C.P., 2001. Effects of ion
channel blockade on the distribution of Na, K, Ca and other elements in oxygen-glucose
deprived CA1 hippocampal neurons. Neuroscience. 103 (4), 971-983.
McBain, C.J., Traynelis, S.F., Dingledine, R., 1990. Regional variation of extracellular space in
the hippocampus. Science. 249 (4969), 674-677.
29
Morris, G.F., Bullock, R., Marshall, S.B., Marmarou, A., Maas, A., Marshall, L.F., 1999. Failure
of the competitive N-methyl-D-aspartate antagonist Selfotel (CGS 19755) in the treatment of
severe head injury: results of two phase III clinical trials. The Selfotel Investigators. J
Neurosurg. 91 (5), 737-743.
Nicholls, D., Attwell, D., 1990. The release and uptake of excitatory amino acids. Trends
Pharmacol Sci. 11 (11), 462-468.
Rohl, L., Ostergaard, L., Simonsen, C.Z., Vestergaard-Poulsen, P., Andersen, G., Sakoh, M., Le
Bihan, D., Gyldensted, C., 2001. Viability thresholds of ischemic penumbra of hyperacute
stroke defined by perfusion-weighted MRI and apparent diffusion coefficient. Stroke. 32 (5),
1140-1146.
Rossi, D.J., Oshima, T., Attwell, D., 2000. Glutamate release in severe brain ischaemia is
mainly by reversed uptake. Nature. 403 (6767), 316-321.
Shapiro, B.E., 2001. Osmotic forces and gap junctions in spreading depression: a computational
model. J Comput Neurosci. 10 (1), 99-120.
Silver, I.A., Deas, J., Erecinska, M., 1997. Ion homeostasis in brain cells: differences in
intracellular ion responses to energy limitation between cultured neurons and glial cells.
Neuroscience. 78 (2), 589-601.
Steinhauser, C., Gallo, V., 1996. News on glutamate receptors in glial cells. Trends Neurosci. 19
(8), 339-345.
Szatkowski, M., Barbour, B., Attwell, D., 1990. Non-vesicular release of glutamate from glial
cells by reversed electrogenic glutamate uptake. Nature. 348 (6300), 443-446.
Takahashi, M., Billups, B., Rossi, D., Sarantis, M., Hamann, M., Attwell, D., 1997. The role of
glutamate transporters in glutamate homeostasis in the brain. J Exp Biol. 200 ( Pt 2) 401-409.
30
Traub, R.D., Jefferys, J.G., Miles, R., Whittington, M.A., Toth, K., 1994. A branching dendritic
model of a rodent CA3 pyramidal neurone. J Physiol. 481 ( Pt 1) 79-95.
Verheul, H.B., Balazs, R., Berkelbach van der Sprenkel, J.W., Tulleken, C.A., Nicolay, K.,
Tamminga, K.S., van Lookeren Campagne, M., 1994. Comparison of diffusion-weighted MRI
with changes in cell volume in a rat model of brain injury. NMR Biomed. 7 (1-2), 96-100.
Verkhratsky, A., Steinhauser, C., 2000. Ion channels in glial cells. Brain Res Brain Res Rev. 32
(2-3), 380-412.
Wahl, F., Obrenovitch, T.P., Hardy, A.M., Plotkine, M., Boulu, R., Symon, L., 1994.
Extracellular glutamate during focal cerebral ischaemia in rats: time course and calcium
dependency. J Neurochem. 63 (3), 1003-1011.
Walz, W., 1992. Role of Na/K/Cl cotransport in astrocytes. Can J Physiol Pharmacol. 70 Suppl
S260-262.
Yamada, W. M., Koch, C., Adams, P. R., 1998. Multiple channels and calcium dynamics, in:
Koch, C., Segev, I. (Eds.), Methods in neuronal modeling: from ions to networks, MIT Press,
Cambridge, pp. 137-170.
Yi, C.S., Fogelson, A.L., Keener, J.P., Peskin, C.S., 2003. A mathematical study of volume
shifts and ionic concentration changes during ischemia and hypoxia. J Theor Biol. 220 (1), 83106.
31
APPENDIX
Appendix A: model parameters
Table 1: Initial values of the variables
variable
value
unit
[Ca2+]e(0)
2
mM
[Ca2+]a(0)
0.0006
mM
[Ca2+]n(0)
0.0006
mM
[Cl-]e(0)
149.397
mM
[Cl-]a(0)
7
mM
[Cl-]n(0)
14
mM
[K+]e(0)
5.4
mM
[K+]a(0)
130.66
mM
[K+]n(0)
130.66
mM
[Na+]e(0)
140
mM
[Na+]a(0)
17.741
mM
[Na+]n(0)
17.741
mM
[glu]e(0)
0.001
mM
[glu]a(0)
3
mM
[glu]n(0)
3
mM
fa(0)
0.3
-
fn(0)
0.5
-
Vma(0)
-73.3
mV
Vmn(0)
-53.3
mV
Table 2: Model constants
parameter
definition
value
unit
Ca
astrocyte capacity
20.92
pF/µm2
32
Cn
neuron capacity
22.44
pF/µm2
F
Faraday’s constant
96480
C.mol-1
R
universal gas constant
8.3145
J.mol-1.K-1
sa
astrocyte surface
2092.41
m2
sn
neuron surface
2244.66
m2
T
absolute temperature
310.15
K
v
global volume
25000
m3
Appendix B: description of the currents
Sixteen types of carriers (channels, exchangers, receptor-channels and pumps) are taken into
account in the model. Nineteen currents represent ion movements across neuron membrane and
twenty two represent ion movement across astrocyte membrane. The equations of the currents
through the different carriers are described below. The currents are expressed in pA/µm 2 and the
conductances in pS/µm2.
-
Voltage-gated channels:
Astrocytic and neuronal potassium channel KDR
IKDR 10
m
3
α(Vm 20)
α(Vm 20) β(Vm 20)
with α(Vm)
-
2
gKDR.m .h.(Vm EK)
0.0047.(Vm 12)
(Vm 12) 12
1 e
and
and
h
1 e
β(Vm) e
Astrocytic and neuronal potassium channel BK
IBK 10
3
gBK.m.(Vm EK)
250.[Ca
m
250.[Ca
2
] .e
i
2
] .e
i
Vm 24
Vm 24
0.1e
1
(Vm 25) 4
Vm 24
33
(Vm147) 30
-
Astrocytic potassium channel Kir
IKir 10
m
-
3
2e
gKir.m.([K ] /([K ] 13)).(Vm EK)
e
e
1
(1.62.(F/( RT)).(Vm EK))
Astrocytic and neuronal calcium channel CaHVA
ICaHVA 6.10
m
αm
αh
-
αm
1 e
1 e
F .gCaHVA.m. h.
and
αm βm
8.5
(Vm 8) 12.5
h
[Ca
( 2 )
2
] [Ca
] .e
i
e
( 2 )
1 e
αh
αh βh
βm
and
0.0015
(Vm 29) 8
2
and
1 e
βh
35
(Vm 74) 14.5
1 e
0.0055
(Vm 23) 8
Astrocytic and neuronal sodium channel NaP
INaP 10
m
αm
-
4
3
gNaP.m.(Vm ENa)
αm
and
αm βm
1 e
h
200
(Vm 18) 16
αh
αh βh
and
βm
1 e
25
(Vm 58) 8
Pumps:
Astrocytic and neuronal Na+/K+ ATPase
[K ]
2
e
IKpump 10 rNaK.
[K ] 3.7
e
with
F
φ
2
3
[Na ]
0.052.Sinh φ
i .
.
[Na ] 0.6 0.026.e φ 22.5.e φ
i
.(Vm 176.5)
RT
INapump
3
IKpump
2
34
-
Astrocytic and neuronal Ca2+ ATPase
ICapump 10
-
2
Astrocytic and neuronal Cl- ATPase
IClpump 10
-
2
[Ca ]
i
rCa.
[Ca 2 ] 0.0002
i
2
[Cl ]
i
rCl.
[Cl ] 25
i
Exchangers:
Astrocytic and neuronal Na+/Ca2+ exchanger
2 gNaCa
ICaexch 10 .
.
4
12
INaexch
3
(FVm/(2RT) )
(FVm/(2RT) )
3
2
3
2
[Na ] .[Ca ] .e
[Na ] .[Ca ] .e
i
e
e
i
3
2
3
2
1 0.0001.([N a ] .[Ca ] [Na ] .[Ca ] )
e
i
i
e
ICaexch
2
-
Astrocytic and neuronal glutamate transporter
IKtrg 10
3
gtrg.(2Vm Etrg)
3
[Na
]
[glu]
[K
]
RT
e .
e
i .
Etrg
Log
F
[Na ] [K ] [glu]i
i
e
INatrg 3IKtrg
Iglutrg IKtrg
-
Astrocytic and neuronal Cl-/HCO3- exchanger
IClexch 10
-
2
[Cl ]
i
gClexch.([ Cl ] 4) .
i
[Cl ] 2
i
2
Astrocytic Na+/K+/Cl- exchanger
35
IKastro 10
2
[K ]
[Na ] ([Cl ] ) 2
e
e .
e
.
gastro.
[K ] 2.7 [Na ] 25 ([Cl ] ) 2 1600
e
e
e
INaastro IKastro
IClastro 2IKastro
-
Receptor-channels:
Astrocytic AMPA receptor
IKAMPA 10
with
([K ] [K ] ).e 1
2
3 PK.F
i
e
.[K ] .A([glu], Vm).Vm.
e
RT
e 1
FVm
RT
and A([glu], Vm)
1100.[glu]
1100.[glu]
e
e
190
([Na ] [Na ] ).e 1
2
3 PNa.F
i
e
INaAMPA 10 .
.[Na ] .A([glu], Vm).Vm.
e
RT
e 1
with
-
PNa PK
Neuronal NMDA receptor
([K ] [K ] ).e 1
2
3 PK.F
2
i
e
IKNMDA 10 .
.[K ] .A([glu], Vm).B([Mg
], Vm).Vm.
e
RT
e 1
A([glu], Vm)
72.[glu]
e
72.[glu] 6.6
e
and
B([Mg
2
], Vm)
1 0.028.e
1
0.062.Vm
([Na ] [Na ] ).e 1
2
3 PNa.F
2
i
e
INaNMDA 10 .
.[Na ] .A([glu], Vm).B([Mg
], Vm).Vm.
e
RT
e 1
with
PNa PK
ICaNMDA 10
with
3 4PCa.F
.
RT
2
.[Ca
2
] .A([glu], Vm).B([Mg
e
2
PCa 6PK
Extra currents:
36
([Ca
], Vm).Vm.
2
2
2
] [Ca ] ).e
1
i
e
2
e
1
-
Astrocytic and neuronal glutamate current
Igludiff 10
-
3
* ggludiff * (Vm Eglu)
Astrocytic and neuronal chloride current
ICldiff gCldiff * (Vm ECl)
37
Figure legends
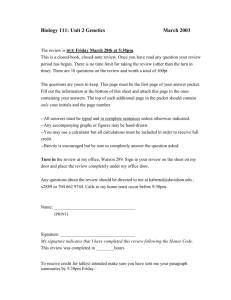
Fig. 1. Components of the model: the three compartments (intra-neuron space, intra-astrocyte
space and extracellular space) and the channels, exchangers and pumps which carry ions K+,
Na+, Ca2+, Cl- and glutamate across the cell membranes.
Fig. 2. Dynamics of the membrane potentials (in mV) vs. time (in min) during a severe
ischaemia (solid) and during a moderate ischemia (dash-dot). Left: depolarisation of the neuron
membrane. Right: depolarisation of the astrocyte membrane.
Fig. 3. Dynamics of the ionic concentrations (in mM) vs. time (in min) during a severe ischemia.
Top: large increase in Ca2+, Na+, Cl- concentrations and decrease in K+ and glutamate
concentrations in the neuron. Bottom: large increase in K+ and glutamate concentrations and
decrease in Ca2+, Na+ and Cl- concentrations in the extracellular space.
Fig. 4. Dynamics of the main neuronal currents (in pA/µm2) vs. time (in min) during a severe
ischaemia: a) potassium currents, b) sodium currents, c) calcium currents and d) currents
involving glutamate.
Fig. 5. Dynamics of rADCw vs. time (in min) during a severe ischaemia (solid) and during a
moderate ischaemia (dash-dot). rADCw decreases from 1 down to 0.5 over one hour of severe
ischemia and from 1 down to 0.78 over one hour of moderate ischemia.
38
Fig. 6. Study of the result robustness after the simulation of one hour of severe ischaemia with
1000 different conductance sets chosen at random in their physiological ranges. Distribution of
four variables of the model: a) the extracellular potassium concentration, b) the neuronal
potassium concentration, c) the neuron potential and d) the rADCw.
Fig. 7. Dynamics of rADCw vs. time (in min) during a moderate ischaemia and when a NaP
channel blocker is introduced 20 minutes after the occlusion onset. rADCw decreases from 1
down to 0.76 within the twenty first minutes and, after introducing the NaP channel blocker, it
dramatically increases before stabilizing at 0.82.
Fig. 8. Influence of an NaP channel blocker on the values of rADCw after one hour of stroke vs.
the residual production of ATP (pATP). Whatever the residual production of ATP, the rADCw
values are higher with the NaP channel blocker (solid) than without any blocker (dash-dot).
Fig. 9. Influence of a KDR channel blocker on the values of rADCw after one hour of stroke vs.
the residual production of ATP (pATP). Whatever the residual production of ATP, the rADCw
values are lower with the KDR channel blocker (solid) than without any blocker (dash-dot).
39
pump
Cl-
Cl-
pump
2K+
Ca2+
Ca2+
pump
Na+/K+
pump
Na+/K+
3Na+
3Na+
Ca2+
Na+
exchanger
Na+/Ca2+
exchanger
Na+/Ca2+
pump
Cl-
Na+ voltage-gated
channel (NaP)
K+ voltage-gated
channel (KDR, BK, Kir)
K+ voltage-gated
channel (KDR, BK)
K+
Ca2+
Ca2+ voltage-gated
2+
channel (CaHVA) Ca
Ca2+ voltage-gated
K+
Cl-
Ca2+
3Na+
Na+ voltage-gated
channel (NaP) Na+
Ca2+ channel (CaHVA)
K+
pump
Ca2+
Extracellular
space
3Na+
Neuron
2K+
K+
K+
glutamate glu
transporter Na+
glu glutamate
transporter
Na+
receptor
AMPA
receptor
Ca2+
Na+ NMDA
Astrocyte
Na+
K+
Na+
K+
receptor
Na+ AMPA
HCO3-
exchanger
- Cl /HCO3
Cl
glu
Cl-
contransporter
2ClNa+/K+/Cl+
K
exchanger
Cl-/HCO3- Cl-
HCO3glu
extra currents
extra currents
Figure 1
40
Cl-
nVm
aVm
10
20
30
40
50
60
t
10
-20
-20
-40
-40
-60
-60
-80
-80
Figure 2
41
20
30
40
50
60
t
Kn
Can
130
Nan
70
0.6
0.5
0.4
0.3
0.2
0.1
120
110
100
90
10 20 30 40 50 60
t
Ke
60
50
40
30
10 20 30 40 50 60
t
Cae
3
2.5
2
1.5
1
0.5
120
100
80
60
40
20
10 20 30 40 50 60
t
Cln
30
27.5
25
22.5
20
17.5
15
12.5
20
10 20 30 40 50 60
t
Nae
10 20 30 40 50 60
10 20 30 40 50 60
t
Cle
150
140
120
100
80
60
40
20
t
glun
4
3.5
3
2.5
2
1.5
1
0.5
149
148
147
146
10 20 30 40 50 60
Figure 3
42
t
10 20 30 40 50 60
t
10 20 30 40 50 60
t
glue
4
3.5
3
2.5
2
1.5
1
0.5
10 20 30 40 50 60
t
a)
b)
IKDR
INaP
potassium currents
0.12
IBK
sodium currents
0.1
IKNMDA
0.08
-0.02
0.06
-0.04
0.04
-0.06
1
2
3
t
4
INaNMDA
INaexch
-0.08
0.02
1
2
3
4
-0.1
t
-0.12
c)
d)
ICaHVA
calcium currents
ICaNMDA
glutamate currents
1
2
3
4
t
0.002
ICaexch
-0.03
Igludiff
0.001
-0.01
-0.02
Itrg
0.003
0.01
-0.001
-0.002
-0.003
Figure 4
43
1
2
3
4
t
rADCw
10
20
30
40
0.9
0.8
0.7
0.6
0.5
0.4
Figure 5
44
50
60
t
a)
b)
number
number
0.25
0.2
0.2
0.15
0.15
0.1
0.1
0.05
0.05
105
106
c)
107
108
Kn
Ke
105
106
107
108
d)
number
number
0.25
0.6
0.5
0.2
0.4
0.15
0.3
0.1
0.2
0.05
0.1
nVm
-0.15
-0.1
-0.05
0.2
0.05
Figure 6
45
0.4
0.6
0.8
rADCw
rADCw
10
20
30
40
0.95
0.9
0.85
0.8
Figure 7
46
50
60
t
rADCw
1
0.9
0.8
0.7
0.6
0.5
pATP
0.2
0.4
0.6
Figure 8
47
0.8
1
rADCw
1
0.9
0.8
0.7
0.6
0.5
pATP
0.2
0.4
0.6
Figure 9
48
0.8
1
Type of carrier
Type of cell
Current
Ions
potassium voltage-gated channel
neuron/astrocyte
IKDR
K+
potassium voltage-gated and calciumdependent channel
neuron/astrocyte
IBK
K+
potassium voltage-gated channel
astrocyte
IKir
K+
sodium voltage-gated channel
(persistent current)
neuron/astrocyte
INaP
Na+
calcium voltage-gated channel
neuron/astrocyte
ICaHVA
Ca2+
NMDA receptor
neuron
INMDA
K+, Na+, Ca2+
AMPA receptor
astrocyte
IAMPA
K+, Na+
Na+/Ca2+ exchanger
neuron/astrocyte
Iexch
Na+, Ca2+
glutamate transporter
neuron/astrocyte
Itrg
K+, Na+, glutamate
Na+/K+/Cl- exchanger
astrocyte
Iastro
K+, Na+, Cl-
Cl-/HCO3- exchanger
neuron/astrocyte
IClexch
Cl-, HCO3-
pump Na+/K+
neuron/astrocyte
Ipump
K+, Na+
pump Ca2+
neuron/astrocyte
ICapump
Ca2+
pump Cl-
neuron/astrocyte
IClpump
Cl-
extra glutamate current
neuron/astrocyte
Igludiff
glutamate
extra chloride current
neuron/astrocyte
ICldiff
Cl-
(delayed rectifier current)
(inward rectifier current)
(high voltage-activated)
Table 1: Channels, transporters and pumps represented in the model
49
Conductance
Effect on cell swelling
gKDR
-
gBK
=
gKir
=
gNaP
+
gCaHVA
+
gNaCa
+
gtrg
+/-
gastro
+
PK
+
Table 2: Effect of the main conductances on cell swelling
50