Practice -2
advertisement

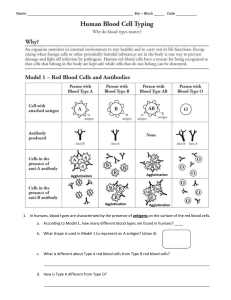
COLLEGE OF HEALTH – HAIL Medical laboratory Dept.- Second term THIRD YEAR – Blood banking Antiglobulin Test PRACTICE -2 Antiglobulin Test The antiglobulin test (Coombs test) was introduced by Coombs, Mourant, and Race in 1945[41] as a method for detecting “incomplete” Rh antibodies (i.e., IgG antibodies capable of sensitising red cells but incapable of causing agglutination of the same cells suspended in saline) as opposed to “complete” IgM antibodies, which do agglutinate saline-suspended red cells. Direct and indirect antiglobulin tests can be carried out. In the direct antiglobulin test (DAT), the patient's cells, after careful washing, are tested for sensitisation that has occurred in vivo; in the indirect antiglobulin test (IAT), normal red cells are incubated with a serum suspected of containing an antibody and subsequently tested, after washing, for in vitro–bound antibody. The antiglobulin test is probably the most important test in the serologist's repertoire. The DAT is used to demonstrate in vivo attachment of antibodies to red cells, as in autoimmune haemolytic anaemia alloimmune HDN, and alloimmune haemolysis following an incompatible transfusion. Antiglobulin Reagents Polyspecific (Broad-Spectrum) Reagents The majority of red cell antibodies are noncomplement–binding IgG; anti-IgG is therefore an essential component of any polyspecific reagent. Anti-IgA is not required because IgG antibodies of the same specificity always occur in the presence of IgA antibodies. Anti-IgM is also not required because clinically significant IgM alloantibodies that do not cause agglutination in saline are much more easily detected by the complement they bind. Monospecific Reagents Prepared By Dr. Abdulrahman elreshid 1 Monospecific reagents can be prepared against the heavy chains of IgG, IgM, and IgA and are referred to as anti-γ, anti-μ, and anti-α; antibodies against IgG subclasses are also available. Specific antibodies against the complement components C4 and C3 and C3 breakdown products can be prepared Recommended Antiglobulin Test Procedure The test should be carried out in glass tubes (75 × 10 or 12 mm). Plastic tubes are not recommended because they may adsorb IgG, which could neutralize anti-IgG of the antiglobulin reagent. Detection of Incomplete Antibodies by Means of the Direct Antiglobulin (Coombs) Test Principle The DAT involves testing the patient's cells without prior exposure to antibody in vitro. For the investigation of cases of AIHA, antiglobulin reagents specific for IgG, IgM, IgA,C3c, and C3d can be used. . * “saline” refers to 9 g/l NaCl buffered to pH 7.0. Method Make a 2-5% suspension of red cells that have been washed four times in saline. Add 1 volume (drop) of the cell suspension to 2 volumes (drops) of antiglobulin reagent. Centrifuge for 10-60 sec. Refer to reagent manufacturer's instructions for specific details. Prepared By Dr. Abdulrahman elreshid 2 Examine for agglutination after gently resuspending the button of cells. A concave mirror and good light help in macroscopic readings. If the result appears to be negative, confirm this microscopically. Macroscopic appearances of agglutination in round-bottom tubes or hollow tiles. Agglutination is shown by various degrees of “graininess”; in the absence of agglutination, the sedimented cells appear as a smooth round button, as on the extreme right. Each DAT or batch of tests should be carefully controlled as previously described. Check negative results with the polyspecific antihuman globulin (AHG) or anti-IgG reagents by the addition of IgG-sensitized cells and anti-C′ by the addition of complement-coated cells. DAT Using Column Agglutination Technology A card of several microtubes enables multiple sample testing. The microtubes contain a solid-phase matrix and the antiglobulin reagent to which patient's red cells are added. During centrifugation, unagglutinated cells pass to the tip of the tube, but agglutinates fail to pass through the gel, which acts as a sieve. As the antiglobulin reagent is already present in the microtubes, no washing or addition of IgG-coated cells to negative tests is required. Refer to individual manufacturer's instructions for details of methods for performing the tests. The advantages of column agglutination technology are as follows: 1. Ease of use and reading and can theoretically be performed by relatively unskilled staff. 2. Less chance of aerosol contamination from infected samples because no cell washing before IATs. 3. The cards can be kept for up to 24 hours, enabling the results to be Prepared By Dr. Abdulrahman elreshid 3 reviewed by experienced staff. 4. Ease of automation and positive sample identification. However, the technology is expensive and its performance does not always compare favourably with the standard LISS–IAT in experienced hands. * DiaMed, AG, Switzerland. ** Bio Vue, Ortho-Clinical Diagnostics, New Jersey. False-Negative Antiglobulin Test Results There are several causes of false-negative test results: 1. Failure to wash the red cells properly—the antisera may then be neutralized by immunoglobulins or complement in the surrounding serum or plasma 2. Excessive agitation at the reading stage—this may break up agglutinates, leading to a false-negative result. 3. The use of impotent antisera so that weakly sensitized cells are not detected. 4. The use of antisera lacking the antibody corresponding to the subclass of immunoglobulin responsible for the red cell sensitization. 5. The presence of an antibody that is readily dissociable and is eluted in the washing process. DAT method in case of HDN – Wash a 3% suspension of the infant’s red cell four times in physiological saline Decant the final supernatant fluid. – Resuspend the packed cells. Add two volumes of AHG reagent and mix. – Centrifuge slowly for 1 minute. Tilting the tube back and forth, examine for agglutination. When there is no agglutination, transfer a small number of cells to a slide and examine microscopically for agglutination.Ensure that the AHG is active by adding 1drop of IgG AHG control cells to the tube as explained previously for the indirect AHGtest. Prepared By Dr. Abdulrahman elreshid 4 – A positive DAT indicates antibody coating of the infant’s red cells. In tropical countries most infants with severe ABO HDN give a positive DAT. ● Check the haemoglobin and serum bilirubin of the infant. Examine aRomanowsky stained blood film from the infant for features of HDN. The blood film will show spherocytosis which may be marked, polychromasia (due to reticulocytosis) and nucleated red cells Note: ABO HDN is rarely sufficiently severe to require an exchange blood transfusion. In a situation in which it is indicated, Group O blood (of the same Rhesus group as the baby) should be selected and crossmatched with the mother’s serum. In contrast to Rhesus HDN, ABO HDN may occur in the first pregnancy and may or may not affect subsequent pregnancies depending on the ABO group of the infant. HDN due to Rhesus incompatibility Rhesus HDN is usually caused by immune anti-D and less commonly by other Rhesus antibodies. It occurs when a Rh negative mother with circulating IgG anti-D antibody (formed from a previous Rhesus incompatible pregnancy) becomes pregnant with a Rh positive infant and IgG anti-D passes into the fetal circulation, destroying fetal cells. The infant can be born severely anaemic and jaundiced. The severity of disease increases with each Rh positive pregnancy. Infants with Rhesus HDN are usually more severely affected than infants with ABO HDN. Prepared By Dr. Abdulrahman elreshid 5