here - Medway NHS Foundation Trust
advertisement

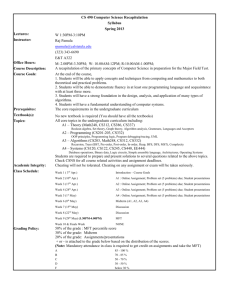
Minutes from the Medway and Swale Drugs & Therapeutics Committee Postgraduate Centre Seminar Room 2 Medway Hospital, Gillingham, Kent, ME7 5NY Wednesday 17th September 2014 12:00pm - 2:00pm 1. Members Richard Patey (RP) Oni Odelade (OO) Louise Dark (LD) Bal Minhas (BM) Bukky Francis (BF) Dr Las Ayathurai (LA) Korede Ibitoye (KI) Dr Maam Mamun (MM) In attendance Asankha Ranasinghe (AR) Lisa Price (LP) Shikohe Masood (SM) Shirley Chan (SC) Rella Workman (RM) Laura Musson (LM) Stephanie Gorman (SG) Sarah Christie (SCh) Chair; Consultant Paediatrician, Medway Foundation Trust (MFT) Prescribing Advisor, Medway Clinical Commissioning Group (CCG) Chief Pharmacist, MFT Prescribing Advisor, Swale Clinical Commissioning Group Formulary Pharmacist, MFT GP, Swale CCG Pharmacist, MCH Consultant Elderly Care, MFT Consultant Paediatrician, MFT Senior Sister – The Birth Place, MFT Urology Consultant, MFT Consultant Surgery, MFT Microbiology Consultant, MFT Anti-microbial Pharmacist, MFT Cardiac Nurse Specialist, MFT Pharmacy Secretary 2. Apologies for absence Yvette Bartlett Zika Petrovic Manpreet Pujara 3. Matters Arising 4. Minutes of the last meeting held and action points All agreed as accurate. Action Log Review The action log was reviewed – refer to log for updates. 5. Conflict of Interests None 1 6. New Drug Applications / Changes to Current Formulary Status Intradermal Sterile Water Injections LP presented the application. Sterile water is used in women who are in labour suffering with lumber pain often associated with occopito-posterior fetal position in labour. Just under 0.8ml is injected just under the skin at 4 points and is to be administered by 2 Midwives simultaneously. LP explained that it is considered safe with no recorded side effects to both mothers or babies just a stinging sensation whilst being administered. It is being used in Scarborough & NE Yorkshire NHS Trust and Birth Centre at Maidstone Hospital. A guideline and a PGD have been produced and it was confirmed that necessary documentation has been approved by PALS and Governance committee. Training will be provided for midwives and this will be on a monthly basis. The cost for each patient was estimated to be about 18p. Decision: APPROVED Action: Audit looking at outcomes and patient satisfaction should be carried out. Result from audit should be brought back to committee in a year’s time _______________________________________________________________________ 10% Metronidazole Ointment Application was discussed in full at last meeting (July) but concerns were raised as the product was unlicensed and does not have marketing authorisation in the UK. Some of the questions raised were: SC answered some of the questions raised: Surgery will be offered if treatment does not work GP’s would not need to prescribe as the ointment lasts for 6 weeks. There are no recorded side effects. SC further explained the drug is still in trials. Patients who have had surgery with non-healed wounds would be suitable for the ointment and the number of patients off trial will be low. SC highlighted that 12 other Trusts already have it on their formularies. LD advised that she was happy to speak to Pharmacists from the other Trusts to see how they got this onto the formulary with the drug still in trials. Decision: NOT APPROVED The committee was supportive but decided it cannot be added to the formulary whilst the trial is taking place due to patient safety. The committee felt that the application needed to go to the Ethics Committee as the product is still in trials. _________________________________________________________________________ Avanafil SM presented the application. Avanafil is for the treatment of erectile dysfunction in adult men. The aim is to use Avanafil when generic sildenafil has failed. SM explained that it has been noted that around 30% to 40% of men fail on their first PDE-5 inhibitor so Avanafil will be an alternative treatment and it is cost effective. The committee asked if Avanafil was to replace one of the other PDE-5 inhibitors (Tadalafil and Vardenafil) already on the formulary but SM explained that it will be best to have all on the formulary as Tadalafil tends to be more suitable for younger patients. Decision: APPROVED but Sildenafil (generic) to remain on 1st line and pathway to be updated with changes 2 _________________________________________________________________________ Dapagliflozin Dr Gough submitted an application for Dapagliflozin. He wanted GPs to be able to initiate treatment with Dapagliflozin. The committee felt that Dapagliflozin should be initiated by specialist only. The committee felt that guideline should be produced for the management of type 2 diabetes and with the recent NICE TA for Canagliflozin the preferred SGLT2 inhibitor should be clearly stated. Decision: Dapagliflozin to remain as Specialist Initiation only and GPs will continue to prescribe after specialist initiation. _________________________________________________________________________ Fultium D3 caps Fultium D3 800units capsules already on formulary, but there is now a new strength of 3200units capsules. This means that patients will only need to take one capsule a day instead of four capsules of the lower strength to treat vitamin D deficiency. Decision: APPROVED Action: Policy to be updated with new preparation _________________________________________________________________________ InVita D3 Oral Solution This is also a new strength and formulation of vitamin D preparation. Only need to take contents of one ampoule weekly instead of daily. Decision: APPROVED Action: Policy to be updated for new preparation _________________________________________________________________________ Sumatriptan/Naratriptan Sumatriptan – Already on the formulary Decision: APPROVED as generic Naratriptan – This is a non formulary drug and therefore a full submission will be needed before it can be considered Decision: NOT APPROVED _________________________________________________________________________ Botox for Achalasia LD explained that the application was made to the DTC as there was a request for Botox for Achalasia, an indication that is not commissioned by Medway CCG. For this particular patient, it was agreed that the cost will come out of Medicine division budget. OO explained that all the indications for Botox is currently being reviewed by HCIAG and once a policy has been produced then this will be brought back to the committee. 7. Guidelines/Pathways Botox for OAB (gynae) pathway 3 Points raised: Needs a title OO highlighted that the dose for the treatment of OAB should be 100units as per SPC Pathway states dose as 200units and references NICE CG 171 (but recommendation by NICE was before Botox was licensed for OAB) Action: This needs to be fed back to Miss Basu and dose also to be clarified. (BF to action) ________________________________________________________________________ Rivaroxaban for DCCV SG presented the updated guideline for DCCV. The committee Points raised regarding the guideline were: Patient consent form has been produced, however was not brought to the meeting. A review date should be added to the guideline. Patient letter SG explained that the consent form is not pre-printed and once the patient has gone through all the questions then page 7 of the guideline will be printed off and patient will have to sign and then put in their medical notes. She further explained that the PIL will go through PALS (Sarah Bush producing this) and the pathway will go through the governance committee. SG asked the committee that if patients are on Apixaban what will be the procedure for CV for such patients and the committee agreed that a line should be added to the guideline for alternative NOACs. Decision: APPROVED and to be rolled out in November _________________________________________________________________________ Pain pathway Points raised were: Changes to title to indicate use in secondary non-specialist settings. Fentanyl patch to change on JF to specialist initiation (orange). Buprenorphine patch to change to black on JF. Zomorph listed as generic Morphine sulphate and adding the preferred brand as Zomorph (make green to highlight as first line use). Add Nortriptyline to JF Decision: APPROVED _______________________________________________________________________ Erectile dysfunction prescribing policy Policy was discussed along with the application for Avanafil. Decision: APPROVED and to be updated with new approved PDE-5 inhibitor. _________________________________________________________________________ COPD guideline – This was not discussed as there is going to be applications for new inhalers. _________________________________________________________________________ Teicoplanin RW presented the updated guideline which is specifically for bone, joint and prosthetic joint 4 infections. She explained that the guideline had been updated to include the recent changes to the SPC and to reflect the doses and monitoring required in patients with impaired renal function. KI felt that section 7.2 should be reworded from 2 weekly to fortnightly to avoid confusion on how often the follow up is done. Decision: APPROVED _________________________________________________________________________ Community Cellulitis Pathway RW explained that there are currently a number of in patients being treated for cellulitis that could in fact be treated as outpatients. Alaisdair Stewart has seen the pathway produced for management of the cellulitis; he feels there are too many patients being treated as inpatients and highlights that more support is needed out in the community. Points raised regarding the pathway below: Class 1 – Doses need to be reviewed Class 3 – Ceftriaxone dose written as 2g without frequency Duration of all treatment to be made clearer on table There is already a pathway for cellulitis used by MEDOCC and not very clear if this supersedes it or just another duplication of pathway. RW explained that the guideline is still being reviewed by the antimicrobial pharmacists and the doses will be adjusted as appropriate. RW is not aware of the pathway used by MEDOCC but she will liaise with Dr Simon Collins, Medical Director of MCH to clarify this. Decision: APPROVED subject to changes as stated above. _________________________________________________________________ CAP guidelines Dr Vincent-Smith should be working on this in line with the Enhancing Quality programme. _________________________________________________________________ Intralipid LD brought to DTC as she felt it needed clinical engagement. Part of the introduction (section 1) in the guideline needs to be reworded and also not clear in terms of immediate management of local anaesthetic toxicity if section 3 (immediate management) should be carried out before section 5 (treatment of cardiac arrest with lipid emulsion). Some of the committee members felt that the guideline is for hospital use only and they had little or no contribution to it. Decision: Committee felt that the guideline is okay but maybe should go to the MMC. _________________________________________________________________ Stroke Pathway This was circulated via email and all members agreed. Decision: APPROVED _________________________________________________________________ Rifaximin shared-care guideline This has not been done by the Gastroenterology team and all doctors leading on it have now left the Trust. Decision: NOT APPROVED. The committee agreed that a letter should be sent to the Gastroenterology team stating that a new submission for Rifaximin will have to be made to 5 the DTC if the team still plans to use the drug as it has been well over 6 months since the initial application was made. 8. Formulary Adherence 9. MHRA Safety Alerts Drug safety update – July Drugs and driving: limits to be set for certain controlled drugs IV dantrolene: risk of skin and injection site reactions – use a filter needle. Fentanyl patches: potential for life-threatening harm from accidental exposure (especially children) Administration errors with drug infusion: checking procedures should be in place. Drug safety update – August Levonorgestrel and ulipristal acetate: suitable for all women regardless of weight or BMI Ofatumumab: risk of serious and fatal infusion reactions. 11. NICE NICE TA 303 – Teriflunomide for treating relapsing-remitting multiple sclerosis. LD explained that MFT is registered as a specialist centre for minimal conditions and still not decided about MS so we can still treat at MFT. APPROVED. NICE TA 312 - Alemtuzumab for treating relapsing – remitting multiple sclerosis. As above for MS, MFT can treat. APPROVED. NICE TA 315 – Canagliflozin in combination therapy for treating type 2 diabetes. APPROVED. NICE TA 316 – Enzalutamide for metastatic hormone-relapsed prostate cancer previously treated with a docetaxel-containing regimen. APPROVED. NICE TA 317 – Prasugrel with percutaneous coronary intervention for treating acute coronary syndromes. APPROVED for specialist initiation only. NICE TA 318 – Lubiprostone for treating chronic idiopathic constipation. APPROVED for specialist initiation only. (Gastroenterologist to complete NICE review form). NICE TA 319 – Ipilimumab for previously untreated advanced (unresectable or metastatic) melanoma. APPROVED. For the treatment of MS, the committee felt that there should be a protocol/guideline for the different therapies. It was therefore agreed that Dr Memon should be invited to the next DTC meeting to discuss this. It was also decided that the current NICE TA forms are sufficient audit trails and application forms do not need to be submitted. 12. Any Other Business 6 Nebulised Colomycin Response received from Lisa Vincent-Smith. Guidelines were being worked on by the Community Respiratory Team. Jane Kindred, Lead Respiratory Nurse can be contacted. Specialist Centre MFT is registered as a specialist centre for minimal conditions; the main areas are Gynae, Neonatal and Inherited cardiac disorders. This in turn means if MFT is not registered as a specialist centre for other conditions we are not able to treat (unless there is a shared care arrangement). It is still not decided about MS; therefore we are still able to treat at MFT. Date of next meeting Wednesday 15th October, 2014 (PG Centre Trust Boardroom) 7