Comparison of iodine contents in gastric cancer
advertisement

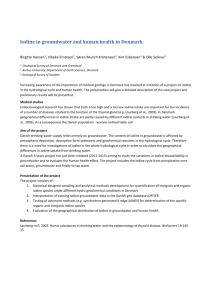
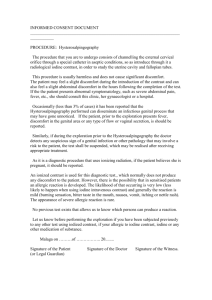
Clinical Chemistry and Laboratory Medicine Vol. 43, n. 6. June 2005: 581-584 Comparison of iodine contents surrounding normal tissues in gastric cancer and Mine Gulaboglu*1, Leyla Yildiz2, Fehmi Celebi3, Mustafa Gul4, Kemal Peker3 1Department of Biochemistry, Faculty of Pharmacy, Ataturk University, Erzurum, Turkey 2Department of Biochemistry, Faculty of Medicine, Ataturk University, Erzurum, Turkey 3Department of General Surgery, Faculty of Medicine, Ataturk University, Erzurum, Turkey 4Department of Physiology, Faculty of Medicine, Ataturk University, Erzurum, Turkey *Correspondence to: Mine Gulaboglu, Ph.D., Department of Biochemistry, Faculty of Pharmacy, Ataturk University, 25240 Erzurum, Turkey. Tel: +90-442-2360961, Fax:+90-442-2360962 E-mail: Gulaboglumine@yahoo.com Key words: Gastric cancer; iodine; tissue. List of abbreviations: NIS: sodium iodide symporter, hNIS: human sodium iodide symporter. Abstract: It is suggested that iodine plays an important role in gastric cancer. Gastric cancer comes first among the cancers in North East Anatolia region, where iodine deficiency is common. In this study, iodine levels were determined in gastric cancer and surrounding normal tissues in 19 patients with gastric cancer. Tissue iodine levels were determined by the Foss method based on the Sandell Kolthoff reaction. Tissue iodine level was lower in gastric cancer tissue (17.8 ± 3.4 ngI/mg protein, mean ± SEM) compared with surrounding normal tissue (41.7 ± 8.0 ngI/mg tissue protein) (p<0.001). There was a positive correlation between the iodine levels in gastric cancer tissue and surrounding normal tissue (r=0.845, p<0.001). There was no significant difference in cancer and surrounding normal tissue iodine levels between male and female subjects. The iodine deficiency in our region may be one of the factors increasing the gastric cancer prevalence. Decreased Na-I symporter activity reported in breast cancer tissue may also be responsible for the decreased iodine levels in gastric cancer tissue in our study. Our results support the hypothesis stating that iodine plays an important role in gastric cancer development. Introduction Iodine is an essential trace element for human health. Iodine deficiency disorders are still seen in our country as well as in many other countries in the world. (The most common consequence of iodine lack is goitre in all age groups.) Goitre rate is accepted as a reliable indicator of iodine deficiency in a population (1). Human stomach, lactating breast and thyroid share an important iodine-concentrating ability. The total amount of iodine is about 30-50 mg in the human body. Less than 30% of it is present in the thyroid gland. About 60-80% of total iodine is non-hormonal and it is concentrated in extrathyroidal tissues, but its biological role is still unknown (2). Venturi has hypothesized that in relation to the functional role of inorganic iodine in metabolism of algal and animal cells, iodide may have a phylogenetic and evolutionary ancient antioxidant role in extrathyroidal iodine-concentrating cells (3). This hypothesis of the antioxidant role of iodine is experimentally confirmed in algae by a recent study carried out by Kupper et al (4). In these cells, iodide may act as an electron donor in the presence of H2O2 and peroxidase, and the remaining iodine readily iodinates the tyrosine (and more slowly, the histidine or some protein and lipid), and so, neutralizes its own high oxidant power (5). The antioxidant action of iodide has also been described in isolated rabbit eyes (6). In early works, Stocks (7), Spencer (8), and Eskin (9,10) found a correlation between goitre, iodine and cancer, and Venturi (3,11) recently found such a correlation with gastric cancer. Venturi (3) has hypothesized that iodine deficiency (I-def) or in some cases iodine excess (I-excess) is associated with the development of gastric cancer. Turkey has been included in the countries with endemic goitre (12). Recently surveys for endemic goitre have shown that no region in Turkey has a prevalence of thyroid hyperplasia lower than 2% (13). According to the WHO, the urinary iodine concentration should be higher than 10 µg/dl in a society with sufficient iodine, and the percentage of people whose urinary iodine concentration is less than 5 µg/dl should not be higher than 20% (14). Akarsu et al. (15) have reported that the prevalence of goitre in the general population is 5.6 % in Erzurum, a city in north-eastern Anatolia. The frequency of people with urinary iodine concentration lower than 5µg/dl was 37.6 %, which shows that this region is an endemic region in terms of iodine deficiency. The fact that gastric cancer is the most frequent among the cancers in Erzurum (16) where iodine deficiency is common (17), stimulated us to carry out this study to determine the iodine levels in tissues with gastric cancer and also in surrounding normal tissue. Materials and Methods Nineteen patients (7 women and 12 males, aged between 43 and 65 with a mean of 57) with gastric cancer were recruited for the study. Pathological diagnosis of gastric cancer was adenocarcinoma. Determination of tissue iodine level. Surgical biopsy specimens from stomach were collected on ice. Specimens were stored at -80 oC until homogenization. They were thawed and homogenized at 0 oC in 0.05 mol/l KH2PO4 containing 10 M KOH. The homogenates were incubated at 115 oC overnight. Homogenates were incinerated in a muffel furnace at 600 oC for 180 min (18,19). The ash was dissolved in 10 ml double distilled H20 and quantified spectrophotometrically at 420 nm using the Sandell-Kolthoff reaction (20). Tissue protein level was determined by the method of Kjeldahl (21). To account for differences in tissue cellularity, results were expressed as nanograms of I per mg protein. Surgical specimens of thyroid tissue (n=2) served as positive controls. Statistical Analysis The results are given as mean ± SEM. A paired t test was used to compare the iodine levels of malignant tumour tissue and surrounding normal tissue. A Mann-Whitney U test was used to compare cancer and surrounding normal tissue iodine levels between male and female subjects and the Pearson correlation coefficient was used to assess the relationships among the parameters. Results The results of iodine levels in stomach and thyroid tissues are shown in Figure 1.Tissue iodine level was lower in gastric cancer tissue (17.8 ± 3.4 ngI/mg protein, mean ± SEM) compared with surrounding normal tissue (41.7 ± 8.0 ngI/mg tissue protein) (p<0.001). All stomach tissue iodine concentrations were lower than those in two normal thyroid specimens, which had iodine concentrations of 566 and 611 ngI/mg protein, respectively (588.5 ± 22.5). (Figure 1). There was no significant difference in cancer and surrounding normal tissue iodine levels between male and female subjects (data not shown). There was a positive correlation between the iodine levels in gastric cancer tissue and surrounding normal tissue (r=0.845, p<0.001, Figure 2). Discussion To our knowledge, decreased iodine level in tissues of gastric cancer compared with the peripheral normal tissues has been reported for the first time in this study. In Italy, quantitative regional data of iodine-deficient goitre indirectly based on the incidence of thyroidectomies and thyroid cancer reported by Lampertico (22), are correlated with gastric cancer mortality. In fact surgical thyroid pathologies including goitre and tumours are correlated, though not exclusively, with iodine-deficiency or (more rarely) iodine-excess. Previous studies have demonstrated the frequent association between atrophic gastritis and goitredysthyroidisms, well known as thyro-gastric syndrome, and between gastric antimucosa and antithyroid antibodies, which might be attributed to common organospecific antigens due to the same embryogenetic derivation. In fact injected antithyroid serum can cause experimental gastritis in the stomach (3). Venturi (3) has shown a trophic regulating action of iodine on gastric mucosa similar to the action on the thyroid and has shown a correlation between iodine-deficiency, goitre and atrophic gastritis. The prevalence of atrophic gastritis was correlated to the degree of iodine-deficiency and goitre. In addition, Venturi has found that a normal gastric mucosa contains more iodine than that affected by atrophic gastritis. Iodine-deficiency (or excess) might constitute a risk factor for gastric cancer and atrophic gastritis. Italians, whose gastric cancer mortality has decreased, have in fact increased yearly fish consumption. On the other hand, in northern Italy, the consumption of even small amount of fish, which is rich in iodine, is a favourable indicator of several cancers, especially of the digestive tract and stomach (23). The thyroid gland shares its capacity to actively accumulate iodide (I-) with several other tissues, including gastric mucosa, lactating mammary gland. The authors have hypothesized that dietary iodine (deficiency or excess) is associated with the development of some gastric and mammary cancer, as it is well known for thyroid cancer (2). Kilbane (18) et al. demonstrated that the tissue iodide content of breast carcinomas was significantly lower than that in remote normal tissue from the tumour-bearing breast or in fibroadenoma. It has therefore been proposed that a disorder of iodide uptake may be involved in the development of breast cancer which might be due to sodium iodide symporter (NIS) inhibiting antibodies. In fact, in various extrathyroidal tissues, such as gastric mucosa, salivary glands, and lacrimal gland, human NIS (hNIS) may act as a target antigen for T cells and cross-reacting autoantibodies, thus perhaps providing a link between autoimmune thyroid diseases and associated autoimmune diseases of other organs systems, such as autoimmune gastritis and Sjögren’s syndrome(24). Using Northern blot analysis (25), much lower levels of NIS mRNA expressions were reported in thyroid carcinoma tissue (one follicular, one anaplastic, and two papillary, tumours) compared with normal thyroid tissue. Similarly, decreased tissue iodine levels in gastric cancer tissue compared with surrounding normal tissue may result from the degeneration of hNIS pump, which takes part in the iodine transport in the cell membrane. It has recently been hypothesized that iodide might have an ancestral antioxidant function in all iodideconcentrating cells. In these cells, iodide acts as an electron donor in the presence of H2O2 and peroxidase, and the remaining iodine atom readily iodinates tyrosine or certain specific lipids (26). Iodine can add to double bonds of some polyunsaturated fatty acids of cellular membranes, making them less reactive to free oxygen radicals (27). Isolated cells from extrathyroidal tissues of mice produce ‘in vitro’ protein-bound mono-iodotyrosine, di-iodotyrosine and also other iodocompounds which seem to be iodolipids when assessed by chromatography (28). Iodolipids are present and active in mammary cells. Weetman (29) et al had already demonstrated that iodine could increase immunoglobin-G synthesis in human lymphocytes in vitro. Immune defences might have an important role in various types of tumours, and perhaps also in gastric cancer (3). Iodine concentration in the stomach and in the thyroid is impaired both by iodine excess and by substances such as nitrate, nitrites, thiocyanates and salt, which can cause goitre and probably gastric cancer (3). This trace element is a regulator of gastric trophism. This trophism regulating action on the gastric mucosa could provide a new interpretation (by impairing iodine intracellular concentration) of the pathogenetic mechanism of previously studied risk factors for gastric cancer (3). Iodine may trigger the mechanism for apoptosis (the natural death of cells) and the main surveillance mechanism for abnormal cells in the body. In the stomach iodine protects against abnormal growth of bacteria in the stomach (of which Helicobacter pylori is the most clinically significant one). Iodine in the stomach can also deactivate some biological and most chemical poisons (30). Failure to trigger the apoptosis in gastric cancer cells due to decreased iodine level may promote the growth of tumour, and explain the relationship between cancer and decreased tissue iodine level in cancer tissue. On the other hand, an excess of dietary iodine (more than 2 mg) impairs the iodide–pump and the functions of some permanently concentrating tissues (thyroid, stomach and salivary gland) causing, in the cause of greater and prolonged quantities, degenerative, necrotic and also neoplastic lesions, which are well known in thyroid gland (31). The fact that the iodine-excess is able to damage the stomach too, should be examined carefully if we consider the coastal populations of Japan (32) and China (33), which have the highest rate of gastric cancer mortality in the word, frequently eat an excessive and harmful quantity of marine algae (seaweeds), which are very rich in iodine (up to 200 mg/daily/per person). The data in literature show that iodine plays an important role in gastric cancer. In this study, lower iodine levels were found in gastric cancer tissue compared with surrounding normal tissue in patients with gastric cancer. Decreased Na-I symporter activity reported in breast cancer tissue (18) may also be responsible for the decreased iodine levels in gastric cancer tissue in our study. Our results support the hypothesis stating that iodine plays an important role in gastric cancer development. The iodine deficiency in our region may be one of the factors increasing the gastric cancer prevalence. References 1. Biber FZ, Unak P, Yurt F. Stability of iodine content in iodized salt. I.Eurosia Conference on Nuclear Science and its Application, Presentations, 2000; 1:1073-7. 2. Venturi S, Donati FM, Venturi M, Venturi A, Grossi L, Guidi A. Role of iodine in evolution and carcinogenesis of thyroid, breast and stomach. Adv Clin Path 2000; 4:11-7. 3. Venturi S, Venturi A, Cimimi D, Arduini C, Venturi M, Guidi A. A new hypothesis: Iodine and gastric cancer. Eur J Cancer Prev 1993; 2:17-23. 4. Kupper FC, Schweigert N, Gall E, Legendre JM, Vilter H, Kloareg B. Iodine uptake in laminariales involves extracellular haloperoxidase–mediated oxidation of iodide. Planta 1998; 207:163-71. 5. Venturi S, Venturi M. Iodide, thyroid and stomach carcinogenesis: evolutionary story of a primitive antioxidant? Eur J Endocrinology, 1999; 140: 371-2. 6. Elstner EF, Adamczyk R, Kromer R, Furch A. The uptake of potassium iodide and its effects as an antioxidant in isolated rabbit eyes. Ophthalmologica 1985; 191: 122-6. 7. Stocks P. Cancer and goitre. Biometrica 1924; 16: 364-401. 8. Spencer JGC. The influence of the thyroid gland in malignant disease. Br J Cancer 1954; 8: 393-411. 9. Eskin BA. Iodine metabolism and breast cancer. NY Acad Sci 1970; 32: 911-47. 10. Eskin BA. Dietary iodine and cancer risk. Lancet 1976; 8: 807-8. 11. Venturi S, Marani L, Magni MA. Syndrome thyro-gastric. Study on the relation between alimentary iodine deficiency and gastric cancer. In: Ghironzi G, Jackson CE, Schuman BM, Editors. Epidemiology Prevention and Early Detection of Gastric Cancer. Rome; CIC, 1987:279-81. 12.Scriba PC, Beckers C, Bürgi H, Escobar DR, Gembicki M, Koutras DA, et al. Goitre and iodine deficiency in Europe. The Lancet 1985; 1293-8. 13. Hatemi H. Endemic goiter and iodine deficiency in Turkey. In: Urgancioglu I, Hatemi H. editors. Endemic goiter in Turkey, Istanbul: Emek Matbaacilik, 1996: 5-28. (in Turkish). 14. WHO-UNICEF-ICCIIDD. Indicators for assessing iodine deficiency disorders and their control through salt iodination. Document. WHO/NUT/1994: 6-36. 15. Akarsu E. Iodine deficiency and goiter prevalence in adults living in Erzurum. Thesis in Endocrinology and Metabolism in Internal Medicine, Faculty of Medicine, Ataturk University, 2000 (in Turkish). 16. Bakan E, Taysi S, Polat MF, Dalga S, Umudum Z, Bakan N, et al. Nitric oxide levels and lipid peroxidation in plasma of patients with gastric cancer. Jpn J Clin Oncol. 2002; 32:162-6. 17.Gulaboglu M. The comparasion of blood, urine and gastric tissue iodine levels in patients with gastric cancer. Ph.D. Thesis in Biochemistry, Faculty of Medicine, Ataturk University, 2004 (in Turkish). 18. Kilbane MT, Ajjan RA, Weetman AP, Dwyer R, McDermott EWM, O’Higgins NJ, et al. Tissue iodine content and serum-mediated I125 uptake –blocking activity in breast cancer.J Clin Endocrinol Metab 2000; 85:1245-50. 19. Lauber K. Iodine determination in biological material, kinetic measurement of the catalytic activity of iodide. Anal Chem 1975; 47:769-71. 20. Foss OP, Hankes LV Slyke DV. A study of the alkaline ashing method for determination of protein- bound iodine in serum. Clin Chim Acta 1960; 5:301-26. 21. Official Methods of Analysis, 14 th ed. Washington, DC: Association of Official Analytical Chemists, 1990. 22. Lampertico P. Pathology of the thyroid gland in Italy: final remarks. Pathologica 1982; 74:400-19. 23. Conforti P, D’Amicis A, Turrini A, Cialfa E. I consumi alimentari in Italia. Istituto Nazionale della Nutrizione. 2° Consensus Conference Italiana 1986-1996. Roma 11-12 giugno 1996; CIC Ediz. Internazionali 24. Spitzweg C, Joba W, Eisenmenger W, Heufelder AE. Analysis of human sodium iodide symporter gene expression in extrathyroidal tissues and cloning of its complementary deoxyribonucleic acids from salivary gland, mammary gland and gastric mucosa. J Clin Endocrinol Metab 1998; 83: 1746-51. 25. Spitzwey C, Morris JC. The sodium iodine symporter: It’s pathophysiological and therapeutic implications. Clin Endocrinol 2002; 57:559-81. 26. Venturi S, Venturi M. Does iodine in the gastric mucosa have an ancient antioxidant role? IDD Newsletter 1998; 14:61-2. 27. Cocchi M, Venturi S. Iodide, antioxidant function and omega-6 and omega-3 fatty acids: a new hypothesis of a biochemical cooperation? Prog Nutr 2000; 2: 15-9. 28. Banerjee RK, Bose AK, Chakraborty TK, De SK, Datta AG. Peroxidase-catalysed iodotyrosine formation in dispersed cells of mouse extrathyroidal tissue. J Endocrinol 1985; 106(2): 159-65. 29.Weetman AP, McGregor AM, Campbell H, Lazarus JH, Ibbertson HK, Hall R. Iodide enhances Ig-G synthesis by human peripheral blood lymphocytes in vitro. Acta Endocrinol (Copenh) 1983;103(2):210-5. 30. Derrry D . “How to prevent and how to survive breast cancer. Trafford Ed. http: // www. Trafford.com/4.dcgi/robots/01.0286.html.21 February 2003. 31. Ingbar SH, Woeber KA. The thyroid gland. In: Williams R. Textbook of Endocrinology. Sixth Ed. New York, Willey, 1980: 118-23. 32. Suzuki H, Higuchi T, Sawa K, Ohtaki S, Horiuchi Y. “Endemic coast goiter” in Hokkaido, Japan. Acta Endocrinol 1965; 50: 161-70. 33.Ma T, Yu ZH, Lu TZ, Wang SY,Dong CF, Hu XY, et al. High-iodide endemic goitre. Chin Med J 1982;95:692-6. Figure legends: Figure 1: Iodine levels in gastric tissue in patients with gastric cancer and surrounding normal tissue. The bars stand for the means ± SEM. The iodine level was 558.5 ± 22.5 in normal thyroid (n=2) tissue. Figure 2: The relationship of iodine levels between malignant and normal tissue in patients with gastric cancer (r=0.845, p<0.001).