Otological Seminar
advertisement

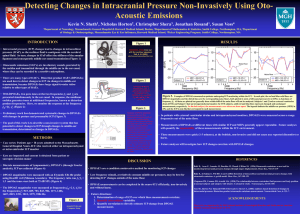
Otological Seminar Evoked Otoacoustic Emission (EOAE) 2003-5-7 R3 KST A. Cochlear amplifier: Electromotility of OHCs (Prestin): ? mechanical source of OAE, Hz-tunning, enhance vibration of basilar membrane at CF (selectivity), e.g. at low stimulus levels due to non-linear cochlear characteristics: The peak of traveling wave grow linearly at low stimulus levels, compressed at moderate to high levels. B. OAE: a. Pre-neural byproducts of cochlear amplifier (OHCs): OAE persist despite 8th nerve is blocked; destruction of OHCs: increases HL~ 60 dB b. Most efferents: to OHCs: CNS regulation (independent of CN 8 afferent fibers) c. OAE are low-level signals: Increased SNR by time-synchronized averaging of signal (amplitude, phase), decreased noise and well-fitted probe C. SOAE: a. multiple Hz, (+) in ~ 50 % normal hearing children/adults, (-) > 25-30 dB HL, b. Higher prevalence in female, right ear, Neonates and infants (2-5 kHz, 8.5 dB) > children and adults (1-2 kHz, 2.6 dB), and the other ear (+). c. SOAE: responsible for < 10 % tinnitus cases (apparent: only 2.4%) D. Characteristics of TEOAEs: 1. Click (COAE, broadband/BB), toneburst (TBOAE) 2. Evaluated in amplitude, amplitude/noise, percentage reproducibility. (Fig 22.4) 3. (+) ~ 100 % in ears with normal sensitivity & ME, (-) in HL > 30 ~50 dB 4. Increased latency with decreased Hz 5. Spectrum (& Hz latency): unique to each individual, depends on: a. Stimulus: COAE BB & lower level, TBOAE more Hz specific b. Recording (Time window): Shorter Loss of low Hz (Longer latency) c. Filter: more elimination from the start more loss of high Hz (Shorter lactency) 6. Amplitude: a. Non-linear TEOAE Amplitude Vs stimulus level (Fig. 22.6) b. varies widely across individual, Hz, c. COAE: lower & BB spectrum level TBOAE: narrower and higher spectrum SOAE: affect spectrum/level of TEOAEs: (+)higher amplitude & more peaks 1 7. Age: No effects on TEOAE level or thresholds. Higher level in female (? smaller EEC), Right ear 8. Criteria: COAE amplitude> 6 dB SPL, reproducibility >70%, 3dB SNR E. Characteristics of DPOAEs: 1. Interaction of two closer Hz (f2> f1) “Distortion” of output/product due to non-linear cochlear systems 2. Exams with constant primary tone levels & differences, Hz & ratio (f2/f1=1.22) 3. Amplitude (Non-linear increase Vs stimulus levels as as TEOAEs): a. Lower: if SOAE (-), and increased age (Hz -dependent Hz, e.g. high Hz, not stimulus levels or SOAE status-dependent) & threshold & f2 Hz. (Sex and Right/left ears: no significant difference) b. Individualized (Fig 22.9) clinical exams at lower/moderate primary stimulus levels. (Higher not as effective due to non-linear, e.g. in identifying HL) 4. 100 % in normal sensitivity & ME, (-) in HL > 50 dB, more stable over time. 5. DP grams: (& 22.10) suppression of 2f1-f2 DPOAE by f2 2f1-f2 reflects f2 hearing sensitivity. F. Clinical applications: A. Identification of HL 1. TEOAEs: best in 2, 4kHz HL by a. Relative operating characteristic (ROC) curve: (Fig. 22.14) Criteria of parameters: COAE level >6 dB, COAE/noise>3, reproducibility> 70% (equal in dDx of (+/-) HL by the 3 parameters in BB-TEOAE & No difference in COAE or TBOAE), mid-level (65-80 pSPL) stimulus, dDx HL by 20-25 dB. b. Multivariate/logistic regression analysis of OAE & OAE/noise etc.: ~100 % accuracy, e.g. with two stimulus types (two click & four TBs) at two levels (e.g. 65/86 dB) 2. DPOAE: better in 4, 6 kHz. a. DPOAE/noise ratio most sensitive (Vs DPOAE level) (Fig. 22.16): also can increase accuracy by . b. logistic regression analysis (9 dB criteria of DPOAE level) b. Hz (max at 2f1 –f2, e.g. f2/f1=1.22), Stimulus level (unequal primaries at mid-levels, L1=L2+10~15 dB, e.g. L2 = 55 dB, more sensitive than equal high levels) (Fig 22.7 & 8) 3. Both TEOAEs and DPOAEs: Hz-specific, similar accuracy at 2kHz, 4. DPOAE: measures higher HL to 50 dB, TEOAE: 25-30 dB HL 2 B. Prediction of hearing threshold: 1. TEAOAE: Low correlation (too complex relationship & high variablity) between COAE/TBOAE and behavioral threshold for prediction of behavioral thresholds. 2. DPOAEs: a. High Variability of DPOAEs & I/O (Too large range) across individuals with similar audiometric threshold unlikely to predict behavioral threshold with DPOAE amplitudes or thresholds. (Despite correlation between DPOAE levels/thresholds & DPOAE/noise and audiometric thresholds in high 4, 8 kHz). b. DPOAE/noise level Vs audiometric threshold to dDx severity of HL (Fig. 22.17) C. NB hearing screening: TEOAEs (as effective as DPOAE): decreased fail rates (3-10%) by decreased noise, more test experience etc. G. dDx 1. Auditory neuropathy: normal EOAE, but HL in behavioral threshold, abnormal ABR and acoustic reflexes 2. ? Acoustic neuroma: some EOAE (+) (? Decreased cochlear blood flow), others (-) 3. Monitor HL: ototoxic agents, NIHL, Meniere’s dz etc. References: 1. Handbook of clinical audiology, 5th eds, Katz J, et al. pp. 440-466 2. Liberman MC, et al. Prestin is required for electromotility of the outer hair cell and for the cochlear amplifier. Nature 2002;419:300-304 3. Gorga MP, et al. Otoacoustic emissions form normal- hearing and hearing-impaired subjects: distortion product responses. J Acoust Soc Am 1993;93:2050-2060 4. Gorga MP, et al. From laboratory to clinic: a large scale study if distortion product otoacoustic emissions in ears with normal hearing and ears with hearing loss Ear Hear 1997;18:440-55 5. Stover L, et al. Toward optimizing the clinical utility of distortion product otoacoustic emission measurements. J Acoust Soc Am 1996;100:956-967 6. Stover L, et al. The effects of aging on otoacoustic emissions J Acoust Soc Am 1993;94:2670-2681 7. Vinck BM, et al. Multiple analysis of otoacoustic emissions and estimation of hearing threshold: Transient evoked otoacoustic emissions. Audio 1998;37:315:334 8. Prieve BA, et al. Analysis of transient evoked otoacoustic emissions in normal hearing and hearing-impaired ears. J Acoust Soc Am 1993;93:3308-3319 3