uveitis_and_iritis
advertisement

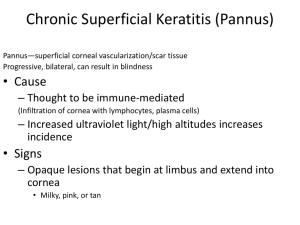
Uveitis and Iritis What is uveitis? Uveitis is inflammation of the uveal tract. The uveal tract is the name given to the part of your eye that is made up of: The iris: the part of your eye that gives it colour. The ciliary body: a small ring-like muscle that sits behind your iris. The choroid: the layer of tissue between your retina and your sclera, containing blood vessels and a pigment that absorbs excess light. Parts of your eye next to the uveal tract can also be affected. These include: The retina: the light-sensitive layer lining the interior of your eye. The optic nerve: the nerve responsible for vision. The vitreous humour: the jelly-like material that fills the chamber behind your lens. The sclera: the white outer layer of your eyeball. What are the different types of uveitis? Uveitis is classified according to the part of the uveal tract that the inflammation affects: Anterior uveitis is when the inflammation affects the anterior part of the uveal tract at the front of the eye. This can include the iris (iritis) or the iris and the ciliary body (iridocyclitis). It is the most common type of uveitis. Intermediate uveitis is when the inflammation affects the middle part of the uveal tract or eye, mainly the vitreous humour. It can also affect the underlying retina. Posterior uveitis is when the inflammation affects the back of the eye. It can affect the choroid, the head of the optic nerve, and the retina (or any combination of these structures). It includes chorioretinitis, retinitis and neuroretinitis. Panuveitis is when the inflammation affects the whole of the uveal tract. Uveitis can also be: Acute: the uveitis is of sudden onset and tends not to last very long (less than three months but usually around six weeks). Chronic: which means it is persistent. The uveitis lasts for more than three months and also relapses (comes back) within three months of stopping treatment. Recurrent: the disease can flare up (relapse) and, at other times, it settles down. The reason why some people develop chronic uveitis is not known. However, it is not thought to be due to inadequate treatment. What causes uveitis? There are many different causes of uveitis and uveitis is associated with a number of other diseases. However, in up to half of cases, no specific cause for uveitis is found. This is known as idiopathic uveitis. The known causes and associations of uveitis include the following: Autoimmune and inflammatory diseases Our immune system normally makes antibodies (small proteins) to attack bacteria, viruses, and other 'germs'. In people with autoimmune diseases, their immune system makes antibodies against the tissues of their body causing damage and inflammation. It is not clear why this happens. Some people have a tendency to develop autoimmune diseases. In such people, something might trigger the immune system to attack the body's own tissues. The 'trigger' is not known. Autoimmune diseases that are associated with uveitis include Behçet's syndrome and rheumatoid arthritis. (See leaflet called 'Rheumatoid Arthritis' for further information about this disease. Behçet's syndrome is a condition that causes recurrent mouth ulcers. It can also affect other parts of your body including your heart, lungs, gut, joints and nervous system.) It is also thought that 'idiopathic' uveitis may actually have an autoimmune basis. People with some other inflammatory diseases are also more prone to uveitis Infection Various types of bacterial, fungal and viral infections can cause inflammation of your eye and uveitis. Infections include herpes simplex, herpes zoster, toxoplasmosis, cytomegalovirus, syphilis, gonorrhoea, tuberculosis and Lyme disease. Infections are a rare cause of uveitis. Injury to the eye Uveitis can occur after injury to your eye. What are the symptoms of uveitis? The symptoms can vary depending on which type of uveitis you have. Anterior uveitis This usually affects one eye. The common symptoms are eye pain (usually felt as a dull ache in and around the eye), redness of your eye, and photophobia (which means you do not like bright light). You may develop blurred vision or even some visual loss (usually temporary). You may develop headaches and notice that your iris (the part of your eye that gives it colour) is a slightly different colour. Your eye may become watery. The symptoms tend to develop over a few hours or days. Intermediate uveitis This usually causes painless blurred vision. It is unusual to experience photophobia and redness of your eye. You may notice floaters and these are a common symptom. Floaters are dark shapes that you see, especially when looking at a brightly illuminated background such as a blue sky. Both eyes are usually affected in intermediate uveitis. Posterior uveitis This commonly causes painless blurred vision. In some people, it can also cause severe visual loss. If you have posterior uveitis you may notice floaters, as described above. You may also develop scotomata. Scotomata are small areas of less sensitive, or absent, vision in your visual field. These areas are surrounded by normal sight. It is usual for only one of your eyes to be affected in posterior uveitis and symptoms tend to take longer to develop. How is uveitis diagnosed? Uveitis is usually suspected on the basis of the symptoms that you have. If your doctor suspects that you have uveitis, you will usually be referred to an eye specialist for further examination and confirmation. The doctor may start by testing your vision. This allows them to assess any differences in vision between your eyes. It also means that they can tell if the uveitis is causing your vision to worsen. The doctor examining your eye will usually use an ophthalmoscope (a hand-held instrument) to examine the interior of your eye. This directs a beam of light into your eye and allows the doctor to examine the inside of your eye where the beam falls. The doctor will usually put in some eye-drops just before the examination. These make your pupils wider so that they can see into your eye more easily. The doctor may also use a special microscope called a slit-lamp to examine your eye. If you have uveitis, the doctor will see some specific changes in your eye that allows them to make the diagnosis. You may also need some other investigations depending on what the doctor thinks is the likely cause of your uveitis. These can include blood tests and X-rays. What is the treatment for uveitis? Treatment for uveitis aims to help relieve pain and discomfort in the eye(s), treat any underlying cause (if possible), and to reduce the inflammation. This may prevent permanent loss of vision or other complications. Treatment usually includes the following: Treatment to relieve pain and discomfort Cycloplegic eye drops: these are special eye drops that can be used to relieve pain by causing the pupil in your eye to dilate (widen). The drops cause your pupil to dilate by relaxing the muscle in the ciliary body. As a result, pain reduces and the inflamed iris is able to rest and recover. Examples include atropine and cyclopentolate eye drops. However, they can have some side-effects. They can make your pupil appear large, can cause temporary blurred vision and also difficulty with focusing. When the effect of the drops wears off, these sideeffects will disappear. The drops need to be used as frequently as every hour when uveitis is first diagnosed. If the drops are not used, the inflammation in the iris may cause it to become 'stuck' to the lens causing permanent scarring. Dark glasses: if your symptoms include photophobia (sensitivity to bright light), wearing dark glasses may be helpful. Painkillers: painkillers, such as paracetamol, taken by mouth may also help. Steroid eye drops are used to reduce the inflammation in uveitis. They are usually the main treatment. Although steroid eye drops usually work well, in some cases side-effects occur, which are sometimes serious. Therefore, steroid eye drops are usually only prescribed by an ophthalmologist (an eye specialist) who can monitor the situation. Possible side-effects that sometimes occur include ulcers on the cornea of the eye which can be very painful and affect your vision. If steroid eye drops are used for long periods of time, they can lead to cataracts or glaucoma. In severe uveitis, steroids are sometimes given by injection into or around your eye. They can also be given by mouth. Again, these can have sideeffects if used in the long-term. The main side-effects from steroids taken by mouth occur when they are used for more than a few weeks. These include thinning of the bones (osteoporosis), thinning of the skin, weight gain, muscle wasting and an increased risk of serious infection. If steroid treatment is needed in the longer term to treat uveitis, a second drug known as an immunosuppressive drug may be used. This can help to reduce the amount of steroids needed and/or help to control the uveitis if steroids are not working. Treatment of underlying conditions and causes Any underlying cause of your uveitis also needs to be treated (if possible). This means treating any underlying infection, inflammatory disease or autoimmune disease. Occasionally, surgery is needed to treat uveitis (usually chronic uveitis). For example, if someone has persistent floaters that are affecting their ability to see, the vitreous humour in the eye can be removed. Floaters tend to develop because of inflammation causing damage to the vitreous humour. Surgery may also be used to treat the complication of cataracts that can occur.