Procedural Competency Form
advertisement

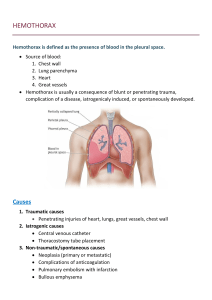
Procedural Competency Form: Simulation/Cadaver Lab Tube Thoracostomy Resident:_______________________________________ Date:__________________ Observing faculty:________________________________ Knowledge Assessment 1. Indications? 2. Important contraindications? 3. Necessary equipment? 4. Complications? 5. Describe how you would obtain informed consent in the stable patient. Checklist of performance: Pre-procedure Demonstrates ability to obtain informed consent when appropriate Evaluates patient/anatomy for potential difficulty Applies oxygen, monitor Prepares and checks equipment Positions patient correctly (arm over head to open up ribs) Verbalizes use of sedation and analgesia Procedure Observes universal precautions (gown, mask, cap, gloves, drapes) Administers local anesthetic (2% Lido to skin, rib, muscles, down to pleura) Incises the skin (3-4cm incision) at 4th or 5th IC space, mid-axillary line Insert Kelly clamp and spread tissues down to pleura “Pop” through pleura with appropriate pressure and spread the clamp Insert finger to palpate pleura and lung Use Kelly clamp to insert tube and position appropriately (clamped end) Post-procedure Secures tube with silk suture Applies appropriate dressing (vasoline gauze, cut 4x4’s,and tape) Orders and reviews post intubation chest x-ray Describes documentation (consent, indication, procedure, complications) Assessment (circle one): Unsatisfactory Area for improvement Yes No N/A Satisfactory Comments: Faculty signature:_____________________________________________________________ Resident signature:____________________________________________________________ Tube Thoracostomy Notes Indications Pneumothorax o Spontaneous o Open o Tension Hemothorax Empyema Severe effusions Flail chest requiring mechanical ventilation Prophylaxis before transport to a trauma center Contraindications For unstable injured patients with a pneumothorax or hemothorax, there are no absolute contraindications. In the stable patient, relative contraindications include coagulopathy, adhesions, or emphysematous blebs. Equipment Sterile drapes and towels Antiseptic solution (Betadine) 20mL syringe with 18 and 25 gauge needles for anesthetic 20mL of 2% Lidocaine +/- epinephrine No. 10 scalpel Large Kelly clamps x2 Chest tubes 28-36F Needle driver Forceps Large, straight and curved scissors 0 or 1-0 silk on large cutting needles Gauze pads Adhesive tape—cloth backed Drainage set-up (Pleuravac kit) o Clear, sterile plastic tubing in 6-foot lengths, ½-inch diameter o Hard plastic serrated connectors o Drainage apparatus with sterile water for water seal o Y connectors o Drainage and suction systems Complications Misplaced tube (along chest wall, subQ, or intra-abdominal/liver/sleen) Infection Laceration of an intercostal vessel or lung parenchyma Subcutaneous air leak Bleeding Indications for Surgery After Tube Thoracostomy Massive hemothorax, >1000–1500 mL initial drainage Continued bleeding o 300–500 mL in first hour o 200 mL/hour for first 3 or more hours Increasing size of hemothorax on chest film Persistent hemothorax after 2 functioning tubes placed Clotted hemothorax Large air leak preventing effective ventilation Persistent air leak after placement of second tube or inability to expand lung fully