Notes:
Blood Losses, Fluid Gains
CASE THREE
Dr. Christie Lee
Dr. Dominique Piquette
Notes:
PART ONE
Published by Articulate® Presenter
www.articulate.com
Notes:
You are on call in the ICU and the CCRT nurse calls
you because a patient has become very short of
breath. You are in the midst of intubating and
getting central access when the nurse calls. The
call is placed over the speaker phone…
Notes:
“Dr. Jones, I’m on the sixth floor with Mrs. Pang.
She is a 54-year-old female that I got called
about because she is very short of breath. Her
saturation was 82% on room air, and she is in the
low-90’s now on 50% face mask. Her blood
pressure is 95/60 and she is tachy at 115. She just
went for a total abdominal hysterectomy bilateral salpingo-ovariectomy (TAH-SOB) this
morning. Marco, the respiratory therapist, just
drew a gas.”
Published by Articulate® Presenter
www.articulate.com
Notes:
“OK. Well be sure to order a chest Xray and some repeat blood work. I will
be down in five minutes. I’m just
stabilizing someone in the unit. If
things get worse call me right away.”
You look at the clock….it's 9:45pm. You finish tying your
last suture and just as you are removing your gloves and
gown, the overhead page comes through…
Notes:
CODE BLUE, 6TH FLOOR,
RM 509. REPEAT CODE
BLUE, 6TH FLOOR RM 509
You run frantically from the room, while removing your
gear and think what the hell is going on with Mrs. Pang?!
Published by Articulate® Presenter
www.articulate.com
Notes:
As you arrive to the sixth floor, the place is like a zoo.
There are nurses and family members crowding the
hallway and doorway. The RT is at the head of the bed
bagging while CPR has already begun.
Notes:
“Pat! What the hell happened? I just got off the
phone with you! Where is the Crash cart? Let’s get
our leads on. You in the red (RPN), take over from
Pat for CPR. Tell me when you get tired and we
will switch you off….You in the blue, Jane – get
two IV’s started now and bolus with Ringers
Lactate. Pat, what happened???”
“I got back from
talking to you on the
phone and she was
unresponsive. Her
husband was at the
bedside trying to shake
her awake. I called the
code and started CPR.
I was only gone for two
minutes…”
Published by Articulate® Presenter
www.articulate.com
Notes:
Notes:
“She was being worked up for
ovarian mass. She’s otherwise
healthy. No medical problems.
She doesn’t even take meds at
home.”
“OK…Marco, go ahead.
Let’s stop CPR, take a look
at the rhythm……there’s
no pulse, looks like PEA.
Continue CPR. Get me
some more Epi.”
“The ABG from before the code is
back – pH 7.20, PCO2 – 30, HCO3 –
15, PaO2 50, Sats are 85%, Hb
is….40?! Really?”
Published by Articulate® Presenter
www.articulate.com
Notes:
Notes:
The BP comes back at 85/50, HR at 140bpm, with sats at
100%. She has received a total of 4L of Ringers Lactate and
2 units of PRBC are on the way. Stat ICU blood work is
drawn. Her BP responds well to the fluids, and she is now
sitting at 95/50, but is still very tachycardic. You transfer
her to the ICU.
Published by Articulate® Presenter
www.articulate.com
Notes:
QUESTIONS:
- Should you cool
the patient?
- Would there be
any
contraindication to
cooling her?
PROPERTIES
Allow user to leave interaction:
Show ‘Next Slide’ Button:
Completion Button Label:
Anytime
Show upon completion
Next Slide
Notes:
On arrival to the ICU, Mrs. Pang begins to open her
eyes. She is shivering, groggy, but does not obey.
Her vitals on arrival: To – 35, BP 85/55, HR 125, Sats
100%. Her CXR is normal with good placement of
the endotracheal tube (ETT) and subclavian cordis.
Published by Articulate® Presenter
www.articulate.com
Notes:
Her repeat blood work is as follows:
Hb
40
115-165 g/L
Plt
120
150-400 x 10E9/L
WBC
11
4.0-11.0 x 10E9/L
Cr
80
44-106 μmol/L
BUN
10
3.0-7.0 mmol/L
Na
137
135-147 mmol/L
K
4
3.5-5.0 mmol/L
Cl
98
95-107 mmol/L
HCO3
15
21-28 mmol/L
pH
7.25
7.35-7.45
PCO2
34
35-45 mm Hg
Lactate
8
0.5-2.0 mmol/L
ALT
100
<31 IU/L
AST
150
<31 IU/L
Bili
10
<20.0 μmol/L
INR
1.7
0.9-1.10 INR
Notes:
You decide not to cool her because she has some
neuro recovery. In addition, the INR is a bit
concerning. You continue to give her blood, a
total of four units, and crystalloids. Because of
her ongoing hypotension, a norepinephrine
infusion is started to maintain some organ
perfusion. You finally get a chance to look
through the chart.
Published by Articulate® Presenter
www.articulate.com
Notes:
Notes:
You decide to call the surgeon to discuss the case. They
were sure there was no surgical bleeding, and ask to get a
CT before deciding to take her to the OR. While you wait
for the CT, her vitals remain unchanged. She is on
norepinephrine at 1mcg/kg/min (6mcg/min), her
temperature is 34.5, and she has yet to make any urine
despite a total of 4u of PRBC and 6L of crystalloids. You
decide to repeat the blood work.
Published by Articulate® Presenter
www.articulate.com
Notes:
Objectives:
-To be familiar
with the most
recent ACLS
guidelines.
-To discuss an
early differential
diagnosis of
cardiac arrest.
-To discuss the
principles of postcardiac arrest
care
-To discuss
common
postoperative
complications of
major
intraabdominal
and pelvic surgery
PROPERTIES
Allow user to leave interaction:
Show ‘Next Slide’ Button:
Completion Button Label:
Anytime
Show upon completion
Next Slide
QUESTIONS:
- What can you do
medically to
optimize this
patient's
condition?
- How would you
approach the
surgeons to
advocate for an
early reexploration in the
OR?
- How would you
define a massibe
blood
transfusion?
- What kind of
complications can
you expect from a
massive blood
transfusion?
Published by Articulate® Presenter
www.articulate.com
Notes:
PART TWO
Notes:
You notice that she is starting to ooze from her
cordis site. Her repeat Hb comes back at 55, plt
60, WBC 16, and INR 2.2. Her lactate is now 14,
and her HCO3 is 10. Her pH is 7.15 and her
norepinephrine requirements are up to
3mcg/kg/min (18mcg/min). You give her more
blood (4 units) and decide that it is time to
initiate a massive transfusion protocol. You ask
for the level 1 infuser and for a stat call to the OBGYN and general surgeons on call. You ask the
nurse to add a fibrinogen to your blood work and
order on spec 5 units of FFP.
Published by Articulate® Presenter
www.articulate.com
Notes:
“Dr. S – your patient is really not doing
well. I think it’s time you really think
about taking her back to the OR. I think
there is some surgical bleeding going on.
I need you to take her back for a look.
She is already in some low-grade DIC I
think, and I’m starting her on a massive
transfusion protocol. I have already
called anesthesia to come.”
Notes:
Three hours later, she comes back from the OR. There was a
total of 4L of blood removed from the peritoneal space. A
small bleeding artery was identified at the site of the
diaphragm biopsy. This was sutured. Intra-operatively, she
received a total of 2 pools of platelets, 4 units of PRBC, 5 units
of FFP, and 10 units of cryo. A total of 4L of ringers was also
administered. She comes back to the ICU on 2mcg/kg/min
(12mcg/min) of norepinephrine. She is on AC/VC mode
ventilation, sedated on fentanyl and versed, and still has not
made any urine throughout the OR.
Published by Articulate® Presenter
www.articulate.com
Mrs. Pang’s temperature at this point is 34, her blood pressure is
95/60 and her heart rate is 110.
INR
2.3
Fibrinogen
1.5
Plt
50
150-400 x 10E9/L
Hb
70
115-165 g/L
Cr
250
44-106 μmol/L
BUN
25
3.0-7.0 mmol/L
AST
3000
<31 IU/L
ALT
4050
<31 IU/L
ALP
800
40-120 IU/L
Bili
70
<20.0 μmol/L
Albumin
20
35-50 g/L
Notes:
0.9-1.10 INR
You continue with supportive management and go to
update the family.
Notes:
Objectives:
-To discuss the
definition and
complications of
massive
transfusions.
-To discuss the
physiopathology
and management
of coagulopathy
related to massive
transfusions.
Questions:
PROPERTIES
Allow user to leave interaction:
Show ‘Next Slide’ Button:
Completion Button Label:
Anytime
Show upon completion
Next Slide
- Which
transfusion
guidelines would
you follow during
a massive
transfusion
protocol?
- Who should you
contact to help
you achieve your
Published by Articulate® Presenter
www.articulate.com
transfusion
targets?
- What would you
tell the family?
- Any predictions
in terms of shortterm and longterm prognosis?
Notes:
PART THREE
Published by Articulate® Presenter
www.articulate.com
Notes:
Over the next 24 hours, Mrs. Pang begins to improve. Her
coags normalize and the shock liver begins to plateau.
She is weaned off the norepinephrine by early afternoon
and her Hb has stabilized at 100. Unfortunately, her Cr
continues to rise. She is oliguric to anuric, with only 5cc of
urine every few hours. A nephrology consultation is
initiated, but in the interim, you think of a differential for
her renal failure and send off some urine lytes that come
back within an hour:
Notes:
Urine Na – 30
Urine Cr – 20
Serum Na – 145
Serum Cr – 500
Published by Articulate® Presenter
www.articulate.com
Notes:
Over the next 48 hours, Mrs. Pang improves dramatically.
Her sedation has been weaned, she is able to obey, but she
remains on the ventilator in a PS mode because of volume
overload. Her BP is 200/110, HR 80, Sats 100% on FiO2 40%.
She remains oliguric to anuric, and her Cr is up to 800.
Notes:
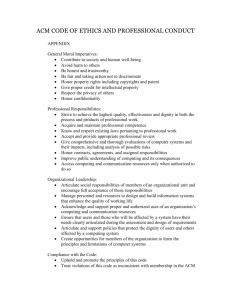
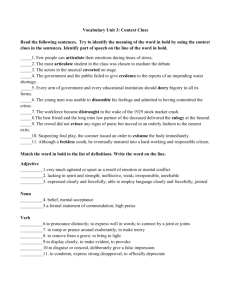
Questions:
- How would you
describe the
parenchyma of
this patient?
- Are you
surprised to see
the left lower
lobe
atelectasis/pleura
l effusion?
PROPERTIES
Allow user to leave interaction:
Show ‘Next Slide’ Button:
Completion Button Label:
Anytime
Show upon completion
Next Slide
Published by Articulate® Presenter
www.articulate.com
Notes:
QUESTIONS:
- What would you
do at this point?
- On which
evidence would
you base your
decision
regarding the best
timing to initiate
hemodialysis?
- Which modes of
dialysis are
available?
PROPERTIES
Allow user to leave interaction:
Show ‘Next Slide’ Button:
Completion Button Label:
Anytime
Show upon completion
Next Slide
- How would you
decide on a mode
of dialysis for this
patient?
Notes:
After discussion with the Nephrology Service, the decision
is made to initiate dialysis. A intravascular catheter is
inserted, and Mrs. Pang is started on SLED.
Fortunately, over the next two weeks, she shows some
evidence of renal recovery.
Published by Articulate® Presenter
www.articulate.com
Notes:
Objectives:
-To discuss the
indications and
modalities of
dialysis in the
ICU.
-To understand
the physiological
principles related
to CCRT.
-To be aware on
the on-going
controversies
regarding the best
timing, indication,
and dose of
CCRT.
PROPERTIES
Allow user to leave interaction:
Show ‘Next Slide’ Button:
Completion Button Label:
Anytime
Show upon completion
Next Slide
QUESTIONS:
- What is the
primary mode of
clearance
(diffusion vs.
convection) of
CVVH, CVVHD,
CVVHDF, SLED?
- What are the
benefits of
convection modes
over diffusion
modes?
- What
determines
clearance?
- Which mode
offers the best
clearance?
- How do you
control the
amount of fluid
removed with
each mode of
dialysis?
- Describe the
risks and benefits
of pre- vs. postreplacement in
CRRT.
Published by Articulate® Presenter
www.articulate.com
References
Bellomo, R., Cass, A., Cole, L., Finfer, S., Gallagher, M., Lo, S., McArthur, C.,
McGuinness, S., Myburgh, J., Norton, R., Scheinkestel, C., Su, S. The RENAL study
investigators. Intensity of Continuous Renal-Replacement Therapy in Critically Ill
Patients. N Engl J Med. 361 (17), 1627-1638 (2009).
Berbece, A.N., Richardson, R.M.A. Sustained low-efficiency dialysis in the ICU: Cost,
anticoagulation, and solute removal. Kidney Int. 70, 963–968 (2006).
Kor, D.J., Gajic, O. Blood product transfusion in the critical care setting. Curr Opin
Crit Care. 16(4), 309-16 (2010).
Mann, W.J., Sharp, H.T., Falk, F.J. Complications of gynecologic surgery. Up to Date.
(2006).
Morrison, L.J., Kierzek, G., Diekema, D.S., Sayre, M.R., Silvers, S.M., Idris, A.H.,
Mancin, M.E. 2010 American Heart Association Guidelines for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care Science. Circulation. 122 (18), 665675 (2010).
Notes:
RCPSP Objectives:
6.2. Cardiovascular Dysfunction
6.2.1. The ability to recognize the problem, provide emergency life support, and embark upon a diagnostic and
management program.
6.2.2. Demonstrate knowledge of:
6.2.2.1. the methods and application of “Advanced Cardiac Life Support” techniques
7.1
Hematological/Oncologic Disorders
7.1.1 The ability to recognize the problem of a patient with a malignancy, a thrombotic or thrombolytic disorder,
bleeding, neutropenia, or anemia, provide for any indicated life-sustaining support, and proceed with an orderly
course of investigation, management, continued monitoring, and support.
7.1.2
6.5.
Demonstrate knowledge of:
7.1.2.1 the pathogenesis and management of thrombocytopenia, anemia, and
7.1.2.3 the coagulation sequence, fibrinolytic pathway, and their associated
7.1.2.5 blood component therapy and alternatives available
neutropenia
disorders
Renal Dysfunction
6.5.1 The ability to recognize the problem of a patient with oliguria or evidence of advancing or established
renal failure, institute measures to preserve remaining renal function, and provide for precise diagnosis, adequate
supportive measures, and appropriate therapy.
9.5.1
Core competencies
9.5.1.2 indication for continuous renal replacement therapy
9.5.2.1 supervision of continuous renal replacement therapy
Published by Articulate® Presenter
www.articulate.com
 0
0