English - IPAC Canada
advertisement

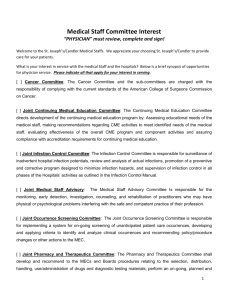
Prevalence of Antibiotic-Resistant Organisms among Adults Hospitalized in Canadian Hospitals – A Follow-up Survey, 2016 Background The emergence of antibiotic-resistant organisms is a major public health concern, particularly in hospitals and other healthcare settings (1-3). Antibiotic-resistant organisms appear to be biologically fit, and are capable of causing severe, lifethreatening infections that may be more difficult to manage because treatment options are limited. The Centers for disease Control and Prevention (CDC) estimates that each year, in the United States, 2 millions illnesses and 23,000 deaths are caused by drugresistant bacteria (4). Antimicrobial resistance may emerge in bacteria as a response to selective antibiotic pressure (5, 6), or a resistant organism may be spread from personto-person within or between healthcare facilities (7-10). Methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), extended spectrum B-lactamase (ESBL) producing Enterobacteriaceae, carbapenem-resistant Enterobacteriaceae (CREs) and Clostridium difficile represent antibiotic-resistant organisms that currently are of great clinical significance in hospitalized patients in Canada. Infections caused by each of these pathogens have been associated with excess morbidity and mortality (11-15). A high prevalence of antibiotic-resistant pathogens may lead to increased lengths of hospital stay and bed-blocking in healthcare facilities. This, in turn, exacerbates hospital overcrowding, leading to a vicious cycle characterized by impeded access to care, diminished quality of care, and greater risk of infection prevention and control failures (16). The treatment and prevention of these infections are associated with substantial increased direct and indirect costs to Canadian hospitals and society at-large. In the United States, cost estimates for managing antimicrobial resistance were estimated to be between $4 billion and $10 billion per year (US Office Technology, 1998). A report commissioned by the Canadian Coordinating Committee on Antimicrobial Resistance noted that significant gaps existed in data addressing the issue of financial costs of antibiotic resistance, but estimated that infections caused by antibiotic-resistant October 5 2015 Version 1.4 1 organisms increased direct hospital costs in Canada by $15-25 million annually (17). These estimates do not take into account indirect costs, or costs associated with infection prevention and control measures. An American study found the treatment costs associated with antimicrobial-resistant infections to be about $6,000 to $30,000 more per patient compared with the treatment costs of antimicrobial-susceptible infections (18). Ironically, this increase in the incidence of drug-resistant pathogens is occurring at a time when the discovery and development of new anti-infective agents is decreasing (2). Despite the concern about antimicrobial resistance, remarkably little is known about the epidemiology or burden of disease caused by antibiotic resistant organisms in Canada. The only national surveillance system, with linked epidemiologic and microbiologic data, tracking antimicrobial resistance in hospitalized patients is the Canadian Nosocomial Infection Surveillance Program (CNISP), currently involving 54 sentinel hospitals across the country working in collaboration with the Public Health Agency of Canada (19-25). Although the CNISP has provided valuable information, the surveillance involves a relatively small number of healthcare facilities, primarily tertiarycare teaching hospitals. Moreover, CNISP surveillance has provided important incidence data, but has not done any prevalence surveys directed at antibiotic-resistant organisms. Several provinces have now mandated public reporting of infections caused by these organisms, but these data are also limited in terms of the scope of infections reported, and by the small amount of information that is collected. An example is the province of Ontario where the only index reported for “MRSA infection” is the rate of MRSA bacteremia. This fails to capture the rates of other infections and colonization that are also associated with morbidity and mortality. The Need for Prevalence Data in Canada The prevalence rate of an antibiotic resistant organism may be defined as the total number of patients with the organism (associated with either infection or colonization) in a specific population during a specified period of time. It may be possible to determine the prevalence per 100 patients admitted to hospital during the specified time period, or to determine a prevalence density to account for length of October 5 2015 Version 1.4 2 patient stay in the hospital (for prevalence density, the denominator would be the number of patient-days). Prevalence surveys have been used for a variety of evaluations including monitoring of infection control, trends in nosocomial infection rates, device utilization, patient acuity and costs of hospital infections (26-30). Despite lacking the accuracy of prospective data, prevalence surveys can provide baseline information and help establish priorities for efficient changes (19). Antimicrobial resistance surveillance that provides accurate prevalence data is critical for the development of strategies that may be used to limit the emergence and spread of antimicrobial resistant organisms. Determining the prevalence of antibiotic resistance organisms has been recognized as an important metric for assessing the burden of disease associated with antimicrobial resistance, for identifying vulnerable patient populations, and for monitoring the effectiveness of various interventions (31). Despite numerous calls for action (10, 32, 33), Canada does not currently have a comprehensive surveillance program for collecting and integrating accurate and representative national data on antimicrobial resistance (34). This significantly limits our ability to respond to the challenges posed to our healthcare system by antimicrobial resistant organisms. This proposal focuses on the burden of illness associated with five major antibiotic-resistant pathogens: MRSA, VRE, ESBLs, CREs and C. difficile. These organisms have been selected because they are of particular concern in Canadian healthcare facilities, because there continue to be significant gaps in our knowledge of the epidemiology of these organisms in Canadian hospitals, and because the majority of Canadian hospitals currently do active surveillance for these organisms, so that relevant data are likely to be available (35). Such information is essential in order to develop and evaluate the effectiveness of hospital and public health measures for the prevention of infections caused by these organisms. Results of the first two National Prevalence Surveys for MRSA, VRE, and C. difficile Infection in Canadian Hospitals We conducted the first two national prevalence surveys of antibiotic-resistant organisms (MRSA, VRE, and C. difficile infection [CDI]) in Canada in November 2010 and November 2012. The survey performed in 2012 also included data on ESBL and October 5 2015 Version 1.4 3 CREs. This surveillance was done in partnership with Infection Prevention and Control Canada (formerly CHICA), and in collaboration with the Public Health Agency of Canada. These surveys provided us with important information regarding the burden of disease in Canadian hospitals associated with these antibiotic-resistant organisms. Results were published in July 2013 (36) and February 2015 (37). Briefly, the results can be summarized as follows: A national point-prevalence survey for infection or colonization with methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE), and for Clostridium difficile infection (CDI) was done in Canadian hospitals in 2010. A follow-up survey was done in November 2012 to determine whether there were any changes in the prevalence of these organisms; we also determined the prevalence of extendedspectrum β-lactamase (ESBL)-producing Enterobacteriaceae, and carbapenemresistant Enterobacteriaceae (CREs). Associations between prevalence and infection prevention and control policies were evaluated in logistic regression models. A total of 143 (67% of eligible facilities) hospitals with 29 042 adult inpatients participated in the survey, with representation from all 10 provinces; 132 hospitals participated in 2010 and 2012. There were no significant changes in the median prevalence of MRSA in 2010 (4.3%) compared to 2012 (3.9%), or of CDI in 2010 (0.8%) compared to 2012 (0.9%). A higher median prevalence of VRE was identified in 2012 (1.3%) compared to 2010 (0.5%) (p 0.04), despite decreased VRE screening in 2012. The median prevalence of ESBLs was 0.7% and was 0 for CREs; CREs were reported from only 10 hospitals (7.0%). A policy of routinely caring for patients with MRSA or VRE in a private isolation room was associated with lower prevalence of these organisms. Targeted screening of high-risk patients at admission was associated with lower MRSA prevalence; better hand hygiene compliance was associated with lower VRE prevalence. Mean and median prevalence of selected antimicrobial-resistant organisms in adult inpatients of Canadian acute-care hospitals, 2010 and 2012 Organism MRSA Colonization or infection Infection VRE Colonization or infection Infection CDI 2010 Prevalence (per 100 inpatients) No. Median Prevalence per patients 100 inpatients (range) 2012 Prevalence (per 100 inpatients) No. Median Prevalence per patients 100 inpatients (range) pa 1472 4.3 (0-22.1) 1218 3.9 (0-26.8) 0.81 175 0.3 (0-5.9) 170 0.3 (0-4.9) 0.78 557 0.5 (0-13.0) 738 1.3 (0-18.0) 0.04 11 350 0 (0-1.8) 0.8 (0-8.6) 18 386 0 (0-1.5) 0.9 (0-5.5) 0.28 0.29 October 5 2015 Version 1.4 4 ESBL Not measured 345 Colonization or infection Not measured 97 Infection CRE Colonization Not measured 32 or infection Infection Not measured 12 a Comparing median prevalence in 2010 with that in 2012 0.7 (0-13.5) 0 (0-4.0) 0 (0-3.0) 0 (0-1.3) The point-prevalence survey conducted in 2010 was the first such prevalence survey done in Canadian hospitals and provided baseline data for specific antibioticresistant organisms. The follow-up survey conducted in 2012 allowed to assess the trends in the prevalence of AROs. We now propose to do a follow-up point-prevalence survey in early 2016. These data will assist in further defining the burden of AROs in Canadian hospitals, and in particular to further determine trends and changes that occur over time. These results will provide important information regarding the appropriate prioritization of treatment and infection prevention programs. October 5 2015 Version 1.4 5 References 1. Schwartz B, Bell DM, Hughes JM. Preventing the emergence of antimicrobial resistance. A call for action by clinicians, public health officials, and patients. JAMA 1997; 278:944-5. 2. Spellberg B, Guidos R, Gilbert D, Bradley J, Boucher HW, Scheld WM, et al. The epidemic of antibiotic-resistant infections: A call to action for the medical community from the Infectious Diseases Society of America. Clin Infect Dis 2008; 46:155-64. 3. Webster PC. Alarm grows over management of antibiotic resistance file. Can Med Assoc J 2010; 182:1602-3. 4. The White House, National Action Plan for Combating Antibiotic-Resistant Bacteria, 2015 5. Gaynes R. Antibiotic resistance in ICUs: A multifaceted problem requiring a multifaceted solution. Infect Control Hosp Epidemiol 1995; 16:328-30. 6. McGowan JE,Jr. Antimicrobial resistance in hospital organisms and its relation to antibiotic use. Rev Infect Dis 1983; 5:1033-48. 7. Aires de Sousa M, Sanches IS, Ferro ML, Vaz MJ, Saraiva Z, Tendeiro T, et al. Intercontinental spread of a multidrug-resistant methicillin-resistant Staphylococcus aureus clone. J Clin Microbiol 1998; 36:2590-6. 8. Kim WJ, Weinstein RA, Hayden MK. The changing molecular epidemiology and establishment of endemicity of vancomycin resistance in enterococci at one hospital over a 6-year period. J Infect Dis 1999; 179:163-71. 9. Loo VG, Poirier L, Miller MA, Oughton M, Libman MD, Michaud S, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med 2005; 353:2442-9. 10. Roberts RB, de Lencastre A, Eisner W, Severina EP, Shopsin B, Kreiswirth BN, et al. Molecular epidemiology of methicillin-resistant Staphylococcus aureus in 12 New York hospitals. MRSA collaborative study group. J Infect Dis 1998; 178:164-71. 11. Conly J. Antimicrobial resistance in Canada. Can Med Assoc J 2002; 167:885-91. 12. Cosgrove SE, Qi Y, Kaye KS, Harbarth S, Karchmer AW, Carmeli Y. The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: Mortality, length of stay, and hospital charges. Infect Control Hosp Epidemiol 2005; 26:166-74. October 5 2015 Version 1.4 6 13. Pepin J, Valiquette L, Cossette B. Mortality attributable to nosocomial Clostridium difficile-associated disease during an epidemic caused by a hypervirulent strain in Quebec. Can Med Assoc J 2005; 173:1037-42. 14. Salgado CD, Farr BM. Outcomes associated with vancomycin-resistant enterococci: A meta-analysis. Infect Control Hosp Epidemiol 2003; 24:690-8. 15. Falagas, M. E., Tansarli, G. S., Karageorgopoulos, D. E., & Vardakas, K. Z. Deaths attributable to carbapenem-resistant Enterobacteriaceae infections. Emerg Infect Dis 2014; 20(7): 1170-1175. 16. Clements A, Halton K, Graves N, Pettitt A, Morton A, Looke D, et al. Overcrowding and understaffing in modern health-care systems: Key determinants in meticillinresistant Staphylococcus aureus transmission. Lancet Infect Dis 2008; 8:427-34. 17. Birnbaum D, Canadian Committee on Antibiotic Resistance. Antimicrobial resistance: A deadly burden no country can afford to ignore. Can Commun Dis Rep 2003; 29:157-64. 18. Cosgrove SE. The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2006;42 Suppl 2:S82-9 19. Gravel D, Taylor G, Ofner M, Johnston L, Loeb M, Roth VR, et al. Point prevalence survey for healthcare-associated infections within Canadian adult acute-care hospitals. J Hosp Infect 2007; 66:243-8. 20. Hyland M, Ofner-Agostini M, Miller M, Paton S, Gourdeau M, Ishak M, et al. NCDAD in Canada: Results of the Canadian Nosocomial Infection Surveillance Program 1997 N-CDAD prevalence surveillance project. Can J Infect Dis 2001; 12:81-8. 21. Miller MA, Hyland M, Ofner-Agostini M, Gourdeau M, Ishak M, Canadian Hospital Epidemiology Committee. Canadian Nosocomial Infection Surveillance Program. Morbidity, mortality, and healthcare burden of nosocomial Clostridium difficile-associated diarrhea in Canadian hospitals. Infect Control Hosp Epidemiol 2002; 23:137-40. 22. Ofner-Agostini M, Johnston BL, Simor AE, Embil J, Matlow A, Mulvey M, et al. Vancomycin-resistant enterococci in Canada: Results from the Canadian Nosocomial Infection Surveillance Program, 1999-2005. Infect Control Hosp Epidemiol 2008; 29:2714. 23. Simor AE, Gilbert NL, Gravel D, Mulvey MR, Beyce E, Loeb M, Matlow A, McGeer A, Louie L, Campbell J. Methicillin-resistant Staphylococcus aureus colonization or infection in Canada: National surveillance and changing epidemiology, 1995-2007. Infect Control Hosp Epidemiol 2010; 31:348-56. October 5 2015 Version 1.4 7 24. Simor AE, Ofner-Agostini M, Bryce E, Green K, McGeer A, Mulvey M, et al. The evolution of methicillin-resistant Staphylococcus aureus in Canadian hospitals: 5 years of national surveillance. Can Med Assoc J 2001; 165:21-6. 25. Simor AE, Ofner-Agostini M, Bryce E, McGeer A, Paton S, Mulvey MR, et al. Laboratory characterization of methicillin-resistant Staphylococcus aureus in Canadian hospitals: Results of 5 years of national surveillance, 1995-1999. J Infect Dis 2002; 186:652-60. 26. French GL, Cheng AF. Measurement of the costs of hospital infection by prevalence surveys. J Hosp Infect 1991; 18 Suppl A:65-72. 27. French GL, Cheng AF, Wong SL, Donnan S. Repeated prevalence surveys for monitoring effectiveness of hospital infection control. Lancet. 1989; 2:1021-3. 28. Gikas A, Pediaditis I, Roumbelaki M, Troulakis G, Romanos J, Tselentis Y. Repeated multi-centre prevalence surveys of hospital-acquired infection in Greek hospitals. CICNet. Cretan infection control network. J Hosp Infect 1999; 41:11-8. 29. Sax H, Hugonnet S, Harbarth S, Herrault P, Pittet D. Variation in nosocomial infection prevalence according to patient care setting: A hospital-wide survey. J Hosp Infect 2001; 48:27-32. 30. Weinstein JW, Mazon D, Pantelick E, Reagan-Cirincione P, Dembry LM, Hierholzer WJ,Jr. A decade of prevalence surveys in a tertiary-care center: Trends in nosocomial infection rates, device utilization, and patient acuity. Infect Control Hosp Epidemiol 1999; 20:543-8. 31. Cohen AL, Calfee D, Fridkin SK, Huang SS, Jernigan JA, Lautenbach E, et al. Recommendations for metrics for multidrug-resistant organisms in healthcare settings: SHEA/HICPAC position paper. Infect Control Hosp Epidemiol 2008; 29:901-13. 32. Health Canada and The Canadian Infectious Disease Society. Controlling antimicrobial resistance. An integrated action plan for Canadians. Can Commun Dis Rep 1997 Suppl 7:i,iv, 1-32, i-iv, 1-32. 33. Mazzuli T. Canadian patterns of antimicrobial resistance: Overview of current trends related to hospital pathogens. Can J Infect Dis 2006 17(Suppl. B):3B-5B. 34. Stephen C, Parmley J, Dawson-Coates J, Fraser E, Conly J. Obstacles to developing a multinational report card on antimicrobial resistance for Canada: An evidence-based review. Microb Drug Resist 2007; 13:251-60. 35. Ofner-Agostini M, Varia M, Johnston L, Green K, Simor A, Amihod B, et al. Infection control and antimicrobial restriction practices for antimicrobial-resistant organisms in Canadian tertiary care hospitals. Am J Infect Control 2007; 35:563-8. October 5 2015 Version 1.4 8 36. Simor AE, Williams V, McGeer A, et al. Prevalence of colonization and infection with methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus and of Clostridium difficile infection in Canadian hospitals. Infect Control Hosp Epidemiol 2013;34:687-93 37. Williams V, Simor AE, Kiss A, et al. Is the prevalence of antibiotic-resistant organisms changing in Canadian hospitals? Comparison of point-prevalence survey results in 2010 and 2012. Clin Microbiol Infect 2015; 21:553-9. October 5 2015 Version 1.4 9 Primary Objectives To determine the prevalence of MRSA and VRE colonization and infection among adults hospitalized in Canadian hospitals To determine the prevalence of C. difficile infection among adults hospitalized in Canadian hospitals To determine the prevalence of extended-spectrum β-lactamase (ESBL)producing organisms and carbapenem-resistant Enterobacteriaceae (CREs) colonization and infection among adults hospitalized in Canadian hospitals To compare the results of this survey with those obtained in the previous surveys done in November 2010 and November 2012 Secondary Objectives To describe demographic and select clinical/epidemiologic features of patients with prevalent MRSA, VRE, C. difficile, ESBL and CREs infection and colonization in Canadian hospitals To describe Canadian hospitals policies on screening and select infection control measures used to control AROs in Canadian hospitals Methods Patient population of interest All acute-care hospitals in Canada with at least 50 inpatients beds will be approached in this point-prevalence survey (hospitals identified from the Canadian Hospital Association (CHA) 2008 database, Volume 15.1). All hospitals that participated in the 2010 and 2012 prevalence survey will also be invited to participate in 2012. A letter inviting healthcare facilities to participate in the prevalence survey will be sent by e-mail to each facility’s Infection Prevention & Control professional (ICP). If there has been no response to this initial communication, the ICP will be contacted a second time by e-mail, and if required, an attempt will also be made to contact the individual by telephone. Eligible patients will include adult inpatients (≥ 18 years of age) hospitalized in a participating hospital on the day of the survey. Long-term care patients in these hospitals October 5 2015 Version 1.4 10 will be included if the long-term care beds are physically associated with a medical unit in the acute-care hospital, or if patients are awaiting transfer/placement to a long-term care facility. Other (free-standing) long-term care facilities, rehabilitation hospitals, complex care facilities and psychiatric hospitals will not be included. Based on the participation in the survey in 2010 and 2012, it is anticipated that at least 180 (65%) hospitals will be willing and able to participate in the 2016 survey. Surveillance design A one-day point-prevalence survey will be conducted in participating Canadian hospitals on a week-day chosen by each participating centre between February 8 and February 19, 2016. On the selected day, eligible patients will be identified by the hospital census (usually defined at midnight or at 6:00 AM). Adult patients in hospital at that time will be included in the prevalence survey. Patients admitted after the census is defined will not be included. Identification of all patients known to be infected or colonized with MRSA, VRE, ESBL or CRE, and all those known to have C. difficile infection may be done at any time in the two weeks following this date. In addition, patients hospitalized on the day of the survey who have cultures or stool specimens that were collected in the days prior or on the day of the survey and that are still pending on the moment of data collection, will also be included if they subsequently yield MRSA, VRE, ESBL, CRE or C. difficile toxin. Patient with a positive sample collected after the day of the survey will not be included. Patients with MRSA, VRE, ESBL and CRE will be defined as those requiring isolation precautions for any of these four organisms (microbiologicallyconfirmed at some point). Patients with MRSA, VRE, ESBL or CRE infection must meet CDC/National Healthcare Safety Network (NHSN) criteria (2015) for infection, and must be on antimicrobial therapy for MRSA, VRE, ESBL or CRE infection on the day of the survey. Patients with C. difficile infection will be identified as those receiving at least one dose of treatment for CDI with a C. difficile targeted antibiotic (oral vancomycin, metronidazole, or fidaxomicin) on the day of the survey for laboratory-confirmed (toxinpositive) C. difficile, or determined to have had pseudomembranous colitis on endoscopy within the previous 14 days. (Definitions in Appendix I) October 5 2015 Version 1.4 11 Data to be collected for each patient with MRSA, VRE, ESBL, CRE and CDI include: (i) age; (ii) sex; (iii) hospital service on the day of the survey (medicine, surgery, obstetrics/gynecology, intensive care unit, etc); (iv) for MRSA, VRE, ESBL and CRE, whether the most recent isolate was obtain as a clinical specimen (to determine the presence of an infection), or as a screening/surveillance specimen (eg. nasal or rectal swab); (v) whether the patient was thought to be infected (using standard definitions) or colonized; (vi) the anatomic site of the isolate (nose, skin, surgical site, respiratory, blood, etc); (vii) whether the organism was initially identified during the current admission or a previous admission; (viii) whether the organism was thought to have been acquired during this admission or a previous admission; (ix) whether the organism was thought to be healthcare-associated (index facility or other healthcare facility); (x) for C. difficile infection, whether this represented a first episode or recurrence (Appendix I). Data will also be obtained to describe each participating hospital: (i) number of admitted inpatients in the hospital on the survey date (at midnight); (ii) total number of inpatients beds; (iii) number of ICU beds; (iv) hospital location (city, province, postal code); (v) type of facility (adults only, mixed adults-pediatrics); (vi) educational category of facility (teaching vs non-teaching hospital); (vii) scope of services provided (acute trauma, burns, oncology, stem-cell transplants, solid organ transplants, neurosurgery, cardiac surgery, dialysis, etc); (viii) number of FTE infection control professionals (ICPs); (ix) hospital policies on MRSA/VRE/ESBL/CRE screening and some aspects regarding management of carriers/infected; (x) laboratory methods for detection of AROs; (xi) the total number of patients on the day of the survey who are on additional precaution in the hospital for any reason (Appendix II). All of the data are to be collected by a hospital Infection Control Professional (ICP) or appropriately trained delegate under the ICP’s supervision. Facilities will not be asked to obtain any additional cultures for the survey. Only data available in the chart or in the infection prevention and control program records will be collected; no patient interviews will be expected or required. October 5 2015 Version 1.4 12 Data analysis The primary outcome measures will be the mean and median (with 95% Confidence Intervals) prevalence rates of MRSA, VRE, ESBL, CREs and C. difficile infection per 100 inpatients. The prevalence of MRSA, VRE, ESBL and CREs infections will also be determined. Regional (or provincial) rates will be calculated, and the rates will also be determined based on: (i) hospital size and (ii) hospital type (teaching vs nonteaching). Patients with AROs will be described by demographic information, and by hospital service. The rates found in this survey will be compared to the rates found in the 2010 and 2012 surveys to assess any change over time. Ethics This point-prevalence survey is observational, without any change in patient care. Moreover, it will be considered to be within the scope of infection surveillance for many of the hospital’s Infection Prevention & Control programs. In order to maintain confidentiality, each hospital will be assigned a numeric code, and each patient will also be assigned a unique study number for entry into the database. No personal identifying data will be provided to the study investigators. Consequently, Review Ethics Board (REB) approval may not be required at all participating hospital sites. However, hospitals may submit the proposal to their local REB for approval if the wish. To facilitate any requirements for REB approvals at some sites, REB approval has been obtained at Sunnybrook Health Sciences Centre (Toronto). Support This is an unfunded surveillance initiative. The project has been endorsed by Infection Prevention and Control (IPAC) Canada. October 5 2015 Version 1.4 13