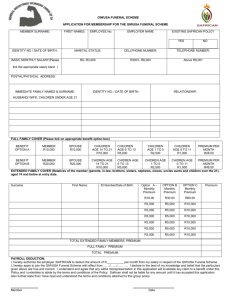
Ezweni Funeral Plan Application Form

Nestlife Group Funeral Plan Application Form
PAYMENT METHOD: Bank Debit Order Salary Stop Order
Main Member Details Assure Risk Solutions:
TT_____________________________________
Title: Surname & First Name:
Date of birth:
Occupation:
ID No:
Postal address:
Phone No (H): Cell No: Phone No (W):
Product Details
Product Name: Cover Main Member : R _________________ Cover Extended Family Cover : R ________________
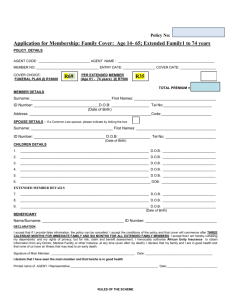
Type of Plan: Family Single Parent Single
Name Surname
Dependant Details
Date of Birth/ID No: Relationship Additional Premium:
Details of Extended Family Members
(If more than five ext. members please use separate sheet)
Surname First Name Relationship Birth Date / ID No Sum
Assured
Premium
Per Month
Title Initials
Nominated Beneficiaries
First Name Surname Birth Date / ID No Relationship Benefits
I, the applicant/policy holder under this policy, hereby nominate the above-mentioned person as the beneficiary in terms of this policy, to receive all benefits payable under this policy. I hereby indemnify NestLife against any claim by myself or by my relatives/estate in respect of the payment of the policy benefits to the beneficiary
Bank Debit Order Authority Premium Calculation
Account Holder Name Account Number Main Member Premium: R
Bank
Branch Name
Branch Code
Relationship to Member
Additional Premiums :R
Total Premium :R
Underwritten by:
FSP No. 6409
Account Type Deduction Date Please tick(x) the applicable box below
1 st 7 th 15 th 20 th 22 nd 25 th 26 th 30/31 st
I hereby grant NestLife Assurance permission to debit my bank account with the monthly premiums on the nominated date (current or arrears), including amendments that may be made in terms or the contract and during the life of the contract. To avoid bank charges and possible cancellation of this policy, please ensure that there are sufficient funds in your bank account on the date of t he deduction.
Signature Of Account Holder: ………………………………………….Date: ……………………………..
Salary Deduction Details
I, ……………………………………………………the undersigned premium payer with ID Number
SALARY
No: ……………………DEPARTMENT: ………………………..INSTITUTION: ……………………………………PAY POINT:…………………….. h ereby authorize the account of my department to deduct from my salary a monthly premium equal to ………………………………………….The first deduction is to be made at the end of the month of ………………………………………20……….. the premium stated must be remitted to the underwriter of the scheme from whom I have purchased a funeral policy. Should the premium be adjusted by the company, I agree that the adjusted premium may be deducted from my salary until such time as I cancel this authority in writing or until substitute it with a new authority.
I hereby understand that should a deduction not be made for any reason, my monthly premium shall not be paid over to the underwriter of the scheme by my employer, and furthermore that I will be responsible for the payment. Should my payment as stated and agreed upon on the stop order not be received by the 7 th of every month, my benefits will be with withdrawn.
SIGNED AT: ……………………………………………… DATE: ……………………………………….
SIGNATURE OF PREMIUM PAYER/EMPLOYEE: ……………………………………………………….
Premium Payer Details
Name & Surname
ID No.
Phone No (H): Phone No. (W):
Cell No:
Declaration
Cell No:
I hereby apply for the NestLife Funeral Plan in accordance with the conditions and exclusions of the plan as set out in the quotation and policy document. I understand that a policy summary, including my personal details, chosen benefits and claims procedures (as intended in Section 48 of the Long-term
Insurance Act), will be posted to me. In accordance with the Long-term Insurance Act, you have 30 (thirty) days, any payment that has been received will be refunded. I am aware of the waiting periods applicable to this policy. There is a limit of (1) one policy per Main Member under the Nestlife Funeral Plan.
I, the undersigned, hereby declare and warrant that all information supplied herein, is true and complete. I am aware, and understand that any nondisclosure or misrepresentation which is material to the determination of the risk by NestLife, may lead to the policy being declared null and void, in which case all premiums paid, will be forfeited. I am certain that the product which I am applying for, meets my needs and feel that I have all the necessary information in order to make an informed decision in respect of the purchase thereof. The Long-term benefits under this policy are subject to the provisions as set out in NestLife's Statutes and the provisions of the master policy. The long-term policy shall come into force and effect on the inception date provided that the offer for insurance made by the Policyholder by way of the proposal form is unconditionally accepted by NestLife and the first premium payable in terms of the Policy was received by Nestlife.
………………………………… Date: …………………. Signature of Main Member / Policy Holder:
Terms & Conditions
Max age at entry for member and spouse is 74 years under the Family Plan and 84 years under the Single Plan
Max age at entry for Extended Family is 84 years
Max of 6 children
6 months waiting period for all new members
24 month suicide exclusion
The waiting period is waived in the event of accidental death
There is no refund of premiums on withdrawal or death of the principal member
Underwritten by:
FSP No. 6409
Schedule of Benefits and Rates
CATE COVER
F
1
G
1
2
H
3
3
2
3
D
1
E
1
2
2
3
C
1
A
1
B
1
Single persons with or without children age 18 – 64 years
R10 000.00
Single persons age 65 – 74 years
R 5 000.00
R 8 000.00
R10 000.00
Single persons age 75 - 85 years
R 5 000.00
R 8 000.00
R10 000.00
Family cover – main member aged 18 – 64 years
R10 000.00
Family cover – main member aged 65 – 74 years
R 5 000.00
R10 000.00
Extended Family age 18 – 64 years
R10 000.00
Extended Family age 65 – 74 years
R 5 000.00
R10 000.00
Extended Family age 75 – 85 years
R 5 000.00
R10 000.00
These Rates include a 20% Broker commission.
All application forms must be fax or email to:
Fax : 086 505 7383
Email : funeral@assurerisk.co.za
PREMIUMS
R 37.70
R 33.80
R 52.00
R 63.70
R 63.70
R 98.80
R123.50
R 52.00
R 42.90
R 91.00
R 31.20
R 28.60
R 53.30
R 53.30
R105.30 x
Underwritten by:
FSP No. 6409