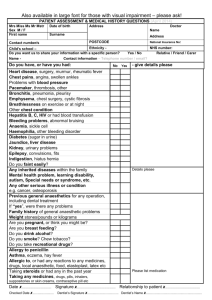
Admin Questions
advertisement

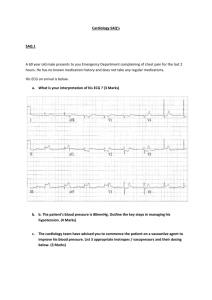
QUESTION Director of Casualty I am writing to you because your department’s incompetence killed my husband Tony. He was seen be a doctor (I don’t know his name but he was very rude and he had blond hair) when he had pains in his chest. We had to wait in the department for 12 hours and he was attached to a machine. All we was told was that he did not have a problem with his heart but we did not know what caused his pain and that night it was back and shocking. Two days later he’s dead and we got told that it was a blood clot on the lung that did it. My 5 children now don’t have a father, and your to blame. We want to know why this happened and to make sure your hospital pays for what it did to him. Yours sincerely, Lynda Charles As the director of a small country hospital, you receive this letter. Outline your actions in response to this letter. ANSWER Actions This is clearly a major issue for the family. It is potentially a major problem for the hospital, department and doctor concerned as it suggests that a pulmonary embolism may have been missed. I will therefore personally respond to the complaint Ensure that the Complaints Liaison Officer or Medical Administrator is aware of the complaint Acknowledge the receipt of the complaint within 24 hours Analyse the complaint letter and identify all the concerns of the author Retrieve the history and examine all the evidence available thoroughly. Search for any deviations from normal clinical practice, such as: Triage assessment Waiting time Assessment Seniority of resident – was he adequately advised by the senior doctor on for that shift Etc. Talk to concerned resident and nursing staff. Some form of counselling may be necessary. Draft an initial response to Ms Charles, expressing regret and sympathy for her situation. Thanks for complaining - a chance to improve systems Non-judgemental Attempt to address the individual issues raised by the complainant o Missed diagnosis of pulmonary embolism o Lack of appropriate follow-up advice o Long waiting time o Medical staff rudeness Expression of liability is not appropriate at this stage. Have draft checked by CLO and / or hospital insurance solicitor Attempt to answer the complaint within 72 hours A meeting with the family may be required at a later stage (perhaps earlier). I would try to arrange counselling for Ms Charles if not already done. Further actions o Education regarding undifferentiated chest pain / pulmonary embolism o Counselling for resident re attitude towards patient o Education of remainder of staff re patient interactions o If there was a problem with triage, then an education session for the nursing staff regarding the National Triage Scale may be worthwhile. Admin SAQ 1. A famous footballer is brought to your department after sustaining injuries in a local AFL football match. A large number of media journalists converge on your hospital to cover the story. You are the duty ED Consultant. How would you manage this situation? 2. You receive a phone call from the mother of a 6 year old boy who presented to your ED the evening before. She wishes to lodge a formal complaint as she had to wait 2 hours to be seen by a doctor. She says her son had a serious break of his forearm bones after a sporting accident and was in excruciating pain whilst in the waiting room. She has already called the Minister for Health who is a friend of hers Describe the actions you would take. SAQ 001 A 45 year old man has a pre-hospital cardiac arrest and is dead on arrival in your ED. He was sent home from your department six hours previously, after being referred by his GP with central chest pain. His family are waiting for you in your office. Explain how you would handle this difficult situation? This is a complex situation with social/medicolegal qualities Pre consultation Patient chart ordered Speak to Dr/nurse/LMO SW notified Timely balance of info vs keeping the relatives waiting Doctor issues Is this an isolated incident? Documentation MDU Mentorship Support Policy and procedure (are they fully orientated and appropriate discharge ?did they ask) Departmental process Scenario Appropriate Quiet No bleep Private Senior nurse Safety aspects Approach ID yourself as most senior in dept and you who will be dealing with this Blame ?accept blame you are “pts advocate” need to outline a plan not role to admit liability establish discharge facts ?self discharge coroner/PM nature of events arrange FU post PM/ further Ix Difficulty with IHD Check CK, TnI and ECG Departmental process and policy who discharged minimum documentation reassess policy SAQ 002 Your charge nurse approaches you to say that several of the nursing staff in your ED have voiced concerns that one of your RMOs is stealing and using opiates from the ED. How do you handle this situation? (or sexually harassing staff, abusing patients, doing incompetent stuff; you pick the atrocity) Introductory statement This is a serious charge that may have significant implications in terms of the systems in place for handling of opiates, the RMO involved, the team and the law. Management will need to encompass all these aspects. Investigate the allegations Talk to the nurses making the allegations requesting specifics: 4where 4when 4how - narcotics taken from dangerous drugs cupboard Vs. taken from the pt for whom they were intended 4action taken by nursing staff 4relationship to the RMO; If @ drug cupboard: 4investigate the drug cupboard contents and the daily tally 4talk to those staff involved with drug counts on the affected days If from patients intended to be given the drugs: 4Talk to the nurses caring for the patients re. amounts given, where stored between aliquots & where remains disposed of 4Review patients charts Suspicious behaviours Undue drowsiness Over-prescribing of opiates esp pethidine (eg; excessive doses) Giving opiates to patients themselves rather than by nursing staff Unexplained absences from ED Review RMOs performance 4Request feedback from registrars & consultants re. RMO’s performance clinically & as member of the team 4Look for “at risk” behaviour patterns 4Ask re performance in previous terms 4Chart review of patients treated by RMO Advise from hospital legal team 4Legal obligations re: 4Reporting of opioid theft/ abuse to police services for investigation 4Reporting of potential opiate abuse to the medical board Discuss with RMO 4Appointment time 4private room 4minimize disturbances 4ask re. Coping & whether any issues that RMO wishes to raise 4discuss allegations with RMO and ask for response to allegations 4non-judgemental approach 4Safety of RMO once allegations made (suicide risk greatest in first days after exposed) If allegations correct: 4offer drug counselling information / confidential medical services for doctors 4suggest sick leave until counselling/ drug rehabilitation in place 4ensure confidentiality 4address any underlying stressors that may be contributing to drug use If denies allegations that appear true: 4Gather evidence 4Will need external review eg; medical board 4Formal investigation instigated Review the procedures in the ED re. handling of opiates 4QA review of the policies and procedures involved in handling of all S8 drugs 4compare handling policies and procedures with those in other similar emergency departments 4quality improvement SAQ 003 Your medical superintendent sends you a memo saying that your junior medical staff numbers are about to be reduced from 8 to 6. How do you respond? Detail your further responses if you do not achieve the desired outcome. (The impending closure of your observation ward would be an alternative problem to consider). Immediate response: Ask for an appointment in a few days time to discuss the issues involved Gather information: Potential Impact on Emergency Department Patient? Current Clinical Indicators & Waiting times Number and type of complaints Critical Incidents/near misses and root cause analysis if done Junior Doctor Issues… Are junior doctors leaving? (And Why? Better training/opportunities elsewhere, poorly treated, stress, fatigue, poorly supported) Roster issues with less staff? More nights/increased stress Gather data on number of patients seen vs years since graduation (SHOs tend to see more patients so their loss has a much greater impact) Policy and Procedure Emergency is a mandatory term for interns (ie probably would lose staff at a JHO/SHO level, increased supervision needed for interns) College guidelines: Access Block, Waiting times vs Triage category Safe working hours project AMA Any reasons for decreased staff Decreased junior doctors numbers across hospital Apparent budget constraints Other departments have a greater need Investigate potential solutions for reduction in staff 1. Find an alternative workforce: Locum junior staff or increase senior staff numbers General Practitioners Close non-essential or less-essential services to free up doctors Paediatric registrar to see children directly Nurses: Nurse practitioners to run minor injury clinic, early pregnancy assessment clinic, community wound reviews, nurse initiated protocols (analgesia, bloods, x-ray) 2. Decrease number of patients Improved discharge planning - TRACC nurse etc to decrease unplanned representations to ED Only do core ED business 3. Measures to prevent blow-out in waiting times Rapid Assessment Team 4. Improve junior doctor training and support During Meeting… Set out information in writing, clearly and concisely. Approach to interview should be of honesty and collaboration. Demonstrate a clear willingness to be part of the solution. Further Action Needed? If no resolution apparent, escalate the concerns to the next person up the management ladder (district manager, state health minister) If still no resolution apparent and reduction of junior doctors does eventuate… Audit clinical indicators/waiting times/complaints/complications/overtime costs/critical incidents /sick leave every 4 weeks Formally document critical incidents and near misses Increase support to junior staff - extend senior/reg cover, informal and formal debriefing, promote healthy lifestyle, ensure appropriate meal breaks, pay overtime as needed if staff willing and able to do it. Notify other departments and junior doctors and ask for their support and understanding during this time. Can they back up our claims and notify management of issues they encounter as they arise If patient outcomes become affected? Report to Executive Director of Medical Services, District Manager, State Health minister, AMA, Unions. Whistle blowing and media to be used as a very last, extreme resort. SAQ 004 Set up a protocol in your ED for the management of (insert one of the following here): DKA Thrombolysis Chest pain MI Suspected epiglottitis Suspected AAA Thrombolysis Protocol Be careful of the wording of the question re: “how to write” versus “write the protocol” Template for “How to develop a policy or protocol” 1. Gather key stakeholders a. ED staff b. Other relevant departments 2. Gather information a. Current evidence b. Protocol from other hospitals (don’t reinvent the wheel) c. Consider hospital infrastructure (eg access to cath lab) 3. Develop a Policy with the frame work.. a. Purpose and Scope (Who the policy is to be used by) b. Content c. Indications d. Contraindications e. Dose f. Issues g. Side Effects h. Complications and their treatment i. Date for review 4. Educate and Certify 5. Quality Assurance and Policy Review as evidence changes THROMBOLYSIS POLICY Purpose of this Policy: To provide appropriate reperfusion therapy aiming for a door-to-needle time in thrombolysis of less than 30 minutes Use of this Policy: This policy is for use in the Emergency Department as part of the Chest Pain Policy. Background of Chest Pain Management: Immediate management of chest pain or ischaemic symptoms should consist of: 1. Application of oxygen and administration of aspirin/GTN 2. Full set of vital signs 3. Treat any life threats (arrhythmia) History is brief and should focus on 2 points: 1. Is this ischaemic chest pain? 2. Are their contraindications to lysis? A ECG should be performed within 5 minutes of presentation shown to a senior doctor (training registrar or consultant) for identification of ST elevation AMI which fulfil criteria for thrombolysis A CXR is not vital prior to thrombolysis Indications for Thrombolysis 1. ECG criteria for AMI fulfilled a. New bundle branch block b. 1mm ST elevation 2 or more of inferior leads c. 2mm ST elevation in precordial leads d. true posterior AMI (ST elevation V9, ST depression V1) 2. AMI with <12hours of chest pain 3. No contraindications for lysis a. Allergy (if using Streptokinase i. SK in past ii. Documented strep throat in last month iii. Aboriginal or Torres Straight islander iv. Known allergy to SK b. Bleeding Risk i. Recent neurosurgery ii. Recent surgery < 4 weeks iii. Haemorrhagic CVA at any time iv. Ischaemic CVA < 3 months v. Recent Trauma < 4 weeks vi. Medical condition that would be complicated by bleeding: suspected dissection or pericarditis vii. Active internal bleeding: GIT bleeding, haematuria 4. Consider Relative Contraindications a. PUD b. Pregnancy or Post partum state c. Prolonged CPR d. Coagulopathy or Anti-coagulation e. Diabetic Retinopathy f. Severe uncontrolled HTN (consider nitrates or B-blockers then lysis) Drugs The Heart Foundation of Australia recommends second generation fibrin specific fibrinolytic agents that are available as a bolus (ie tenectaplase) as the fibrinolytics of choice. Tenecteplase provides a mortality benefit in patients age < 75 years with large infarcts who present early, but at a higher cost, and higher risk of stroke in older patients. Streptokinase is cheaper and may have a lower risk of stroke, but is more complex to administer and frequently causes transient hypotension. Dose Streptokinase: 1.5 x 106 Units in 100 mL normal saline over 60 minutes Adjunct to Thrombolysis 1. Heparin 2. Beta blockers 3. GTN infusion 4. Magnesium 5. Insulin 6. Hypokalemia Referral to PAH for Angioplasty 1. Contraindications to thrombolysis 2. Failed thrombolysis after 90 minutes 3. <75 years old and presenting with cardiogenic shock Side Effects: Bleeding Manual pressure if external bleeding Protamine 25-50 mg slow IVI (max 50 mg in 10 min) to neutralise 100 Units of heparin 6U of platelets IVI to raise platelet count by 50,000 Cease fibrinolytic and other anticoagulants Treat effect of other agents (eg warfarin with Prothrombinex and FFP) Cross match, FBC, aPTT, PT, fibrinogen level Blood transfusion as required Cryopreciptate 10 units IVI repeat until fibrinogen >100 mg/dL If ongoing bleeding: FFP 2U IVI If ongoing bleeding: tranexamic acid 10mg/kg q6-8 hrly If ongoing bleeding: consider: rVIIa 30-100mcg/kg IVI or angiographic embolisation Review This policy should be reviewed by a multi-disciplinary team (cardiology, emergency and nursing) in 48 months or sooner if significant evidence becomes available SAQ 007 With regard to defibrillation: Outline the principle underlying its action List the complications Outline the features you would look for when choosing a new defibrillator/monitor for your ED. Defibrillation action Transient delivery of electrical current causes a momentary depolarization of most cardiac cells. This allows the sinus node to resume normal pacemaker activity. In the presence of reentrantinduced dysrhythmia, such as paroxysmal supraventricular tachycardia (PSVT) and ventricular tachycardia (VT), electrical cardioversion interrupts the self-perpetuating circuit and restores a sinus rhythm. Electrical cardioversion is much less effective in treating arrhythmia caused by increased automaticity Complications Failure to revert rhythm Burns to skin and muscle Pain Dysrhythmia Hypotension Pulmonary oedema Post cardioversion VF Staff – accidental shock Anaesthetic risks – hypoxia, hypotension FEATURES Specifications Battery – SLA vs NiCD Types – monophasic vs biphasic Multifunction devices – integrated NIBP, IABP, PR, Sats, ETCO2 plus trends Ability to pace Pacing options Pad options – paediatric vs adult Weight AC Power adapter and charge times Dual battery capability LCD display – channel option, able to be customised, Ease of use in transfers – how it hangs of bed etc Synchronisation Ancillary Costs Consumables ECG dots ECG paper System issues Hospital wide consistency Integration with ambulance services Integration with current technology Education and support Support – out of hours, maintenance Eduction support and tools Data Management Ability to record events Data transfer capabilities and cables Price Bulk purchase discount with other departments Cost comparisons Warranty – some only have 30day warranties SAQ 314 As the Director of your Emergency Department, one of your emergency registrars enquires of the possibility of purchasing an ultrasound scan machine for the department. Outline the considerations that will need to be addressed in deciding on this acquisition (100%) • NEED – Is there a need? – Define a need / benefit. o Reasons for acquiring it: provided? ternative / addition to existing practices? o Specific clinical indications in question: o What are the alternate options? o Is it justifiable? • RESEARCHING – Check it out. o Types of machines o Properties of each ease of use, quality of images etc o Other practical considerations – size, storage, portability, durability, electrical safety • CONSULTING – asking and benchmarking. o With other departments – ED’s, radiology, cardiology etc o Own ED staff – ED consultants and nursing staff • COSTING. o Purchase costs v Leasing costs? o Running costs? o Maintenance costs? o Cost-effectiveness? o Predicted lives saved / decrease in morbidity? o Funding sources? o Staff training expenses? • ADMINISTRATION. o Quality assurance / auditing issues o Medicolegal / accountability issues o Protocols for use • TRAINING. o Who should be trained? Everyone v dedicated staff o Who will use it? o How will they be trained? By whom? o Skill maintenance o Ongoing education and certification o Guidelines on training – minimal standards • TRIALLING. o Choose machine – set time period o Audit and feedback SAQ 311 Your hospital executive has decided to introduce a new patient database management system. This will replace the current separate systems for clinical, administrative, radiology and pathology data. It will include a completely paperless electronic medical record. (a) Outline the features that will be important for this system to possess in your emergency department (50%) (b) Describe the potential problems involved in implementing such a system (50%) (a) Features of the system • Reliability: o Clinical and medico-legal implications of computing error. o Need for minimal downtime for maintaining system. o Reliable back-up provisions for system failure. • Compatibility: o With institution’s legacy systems (ie: existing IT systems). o With existing hardware capabilities. o With other hospitals / institutions – need for data sharing. Including capacity for networking (local and wide area). • Accessibility: o Multiple hardware access points. o Capacity for simultaneous access. o Remote access by clinicians at home. • Technical: o Hypermedia capabilities ie: capable of supporting graphics, text, video, scanned data all in one patient record. o End-user friendliness – minimal time spent at terminal versus the bedside. • Reporting capabilities: o Need for analysis of data / generation of reports from queries. o For – research, budgeting, audit, quality assurance processes. • Security: o Need to comply with provisions of Commonwealth Privacy Act. o Ability to use password / firewalls to allow levels of access to parts of system. o Security from viruses, criminal activity. (b) Barriers to implementation Recognise that these will be more organisational / managerial than technical. • Cost of implementation: • Research into most appropriate systems. • Cost of actual hardware and software. • Cost of reliable back-up systems. • Cost of time required for hardware installation. • Establishment of evaluation process: • Initial costs will be large and up-front, whereas benefits likely to be intangible and delayed. • Staff satisfaction. • Consumer satisfaction. • Staff training: • Expensive. • May lengthen period of orientation for all new staff. • Will need to be ongoing. • Organisational resistance to change: • Need for informal and formal communication and information sharing. • Consideration of employment of ‘change management consultants’. • Power shifts as different groups are given different levels of access. • Stakeholder consultation: • Government, consumers, users. • Especially with respect to access, privacy issues. • Management decisions: • IT support on contractual basis or full time hospital employment. • Decisions regarding access to information by outside groups eg: clinicians from other hospitals etc. • Method of transition – overlapping systems in operation, introduction by department etc. SAQ 097 List the features which would lead you to suspect a patient of being a drug-seeker. Outline how you would deal with such a patient. Signs that increase suspicion of drug seeking Multiple allergies to non-narcotic medications Stated diagnosis difficult to confirm (radio-opaque renal stones) Vague pains - back, pelvis, headache, dental, abdominal - with minimal clinical signs Carrying letter stating need for narcotics Unknown in hospital/region Presenting out of hours Age >12 Using an alias Asking for specific narcotic by name and dose Requests specific doctor Concurrent alcohol or drug abuse Premature requests for refills Reports lost/damaged/stolen medication Third party requests Therapeutic dependence with true chronic problems Known to Medicare Prescription Shopping Information Service Known to local drug management program Management 1. Manage the Patient * At the initial instance take claims at face value and offer complete assessment with physical examination and investigations. * Provide non-narcotic analgesia - NSAIDS, paracetamol, buscopan, hot packs, TCA, (ensure alternatives are non-addictive) * See further information - other hospital presentations, prescription shopping hotline, hospital medical chart, GP, pharmacy * Consider underlying social issues * Consider undiagnosed organic cause * If narcotic seeking cannot be confirmed give narcotics to alleviate distress with clear end-points and limits on doses. A script for a limited supply (48 hours) until patient can return to normal GP. If ongoing opiate need inpatient assessment should be offered. * For multiple drug allergies consider drugs that don't release histamine: fentanyl, oxycodone * For chronic pain ensure patient has had appropriate investigations have been done to exclude organic causes of pain. * If you are confident the patient is opiate seeking expect a loud outburst and threats when opiate is denied. Avoid confrontation in public places (eg corridor, waiting room) and do this in a private area. Have security staff near. * Listen to concerns/threats and then give a calm explanation as to - why you are concerned and refusing opiates - department policy that supports the refusal - offer alternative management - offer admission/referral for further investigation - offer support/referral for drug rehab, pain clinic - offer withdrawal support - Do not provide a script for opiates. Any scripts that are given should be tamper proof - Notify GP of presentation. * Document carefully in patients chart. 2. Management for Emergency Department doctors * stay up to date in acute and chronic pain management techniques * be aware of where to refer for chronic pain management clinics and drug rehab (inpt vs outpatient) 3. Management of Emergency Department * consider written guidelines re the use of opiates in migraines/chronic LBP, * audit the 'frequent flyers' and develop individual pain management plans * education sessions for staff * clear protocols to contact security if patient becomes aggressive 4. Management of your community * know where drug rehab is available and provide support/referral as needed * notify to medical board if an individual community doctor seems to be over-prescribing opiates SAQ 105 A woman presents to your Emergency Department with multiple injuries sustained in a "fall" at home a week earlier. What features of the history and examination would lead you to suspect domestic violence as the cause of her injuries ? She admits that she sustained her injuries during a beating by her husband. What is your management ? Outline your management of the social issues pertaining to this case. Medical Mx Life threats – strangulation, blunt injury, HI Associated injuries – bruises, wound Tetanus prophylaxis Pregnant ?check fetus Social Accommodation - safe house - offer hospital admission Children ?safe, previous DOF involvement Safety of patient and family Mobilise support network – friends, family, religious DV support groups Support with notifying police Support if returns to partner Drug and alcohol abuse Financial issues Educate/provide information in writing Follow-up phone call Psychiatric illness - depression - suicide risk Pregnancy increased risk Environment in ED Same sex nurse Try to interview alone Support ++ Establish trust and show empathy Social Work involvement Ensure privacy SAQ 226 Outline the ACEM clinical indicators used in measuring Emergency Department performance. Also briefly outline strategies to maintain performance according to these indicators (100%). Clinical indicators are a measure of the clinical management and outcome of care within the Emergency Department. ED clinical indicators should be measurable, achievable, relevant to the clinical practice of emergency medicine and acceptable to emergency physicians as a reasonable measure of performance. ED clinical indicators are a part of overall quality management in Emergency Medicine. Others features of quality systems include risk management; consumer participation; complaint analysis and resolution; clinical audit and review; occupational health and safety; and human resource development. Current ACEM recommended clinical indicators for Emergency Departments: • Access: o Indicators – waiting time; access block. • Safety: o Indicators – lost time to work related injury; body fluid exposures; patient falls. • Acceptability: o Indicators – patient satisfaction survey ratings; written complaint rate. • Effectiveness: o Indicator - admission rate by triage category; time to thrombolysis; unplanned representation within 48hrs. • Efficiency: o Indicator – waiting time by Australasian Triage Scale. • Continuity: o Indicator – provision of written health information for sentinel conditions (eg: asthma, wound care; provision of discharge summary. Strategies to maintain performance: Generally: • Utilise clinical indicators as part of overall quality management within the ED. • Strive for accurate data collection / performance measures. • Education of staff as to what specific clinical indicators are. Specifically: • Waiting time: ensure adequate staffing levels; ensure accurate data collection; review of work practices / time-management / triage practices. • Access block: multi-faceted problem involving whole hospital systems; requires review of systems within ED and whole of hospital regarding usage of in-patient beds. • Safety indicators – staff education, ensure protocols regarding safe use and disposal of sharps and adequate receptacles present, protocols for patient lifts, and protocols regarding use of rails on beds and escorting mobilizing patients. • Acceptability indicators – publicise to ED staff patient satisfaction survey results to highlight good and bad aspects. • Admission rate by triage category – ensure accurate data collection; protocols in place regarding senior review prior to any discharge from ED; ED right of admission with in-patient units. • Time to thrombolysis – staff education regarding indications / contraindications for lysis; review of work practices – ECG and ECG review by senior staff within 10min of arrival; ensure availability of thrombolytics within the ED. • Unplanned representations - protocols in place regarding senior review prior to any discharge from ED; medical staff education programs esp.: commonly missed injuries. • Waiting time – as previous. • Provision of written information / discharge summaries – letter templates on computer terminals; pre-formatted patient information sheets. SAQ 313 You receive a letter from your hospital administration informing you that the Director of Cardiology has made a complaint regarding times to thrombolysis for acute myocardial infarction in your emergency department. They request a response. (a) How would you approach this situation? (50%) (b) What strategies could you implement to improve your times to thrombolysis? (50%) Complaint from Cardiology to administration regarding ED ‘times to thrombolysis’ Response required back to the hospital administration. (a) Approach: • Express initial concern regarding lines of communication between ED and Cardiology. Given that Director of Cardiology didn’t raise this matter directly with ED. • Verify and validate the data being used to show that there are delays in time to thrombolysis – esp: ensure that problems are not due to incorrect data entry. • If data correct and delays are occurring – • Analyse the three issues with this ED system – process, information and decision-making. • Analyse the cases where delays have occurred looking for common issues that have lead to delays eg: • Process problems: appropriate triage of patients with chest pain, adequate nursing and medical staff to manage case-mix / case-load (benchmark to ACEM standards), systems for early ECG, adequate clinical areas (monitored) to manage the case-load of chest pain patients (benchmark to ACEM standards), adequate equipment – enough ECG machines, thrombolytics within ED etc. • Information problems – notification of chest pain patients into ED, is the information (ie: ECG) getting to the appropriate medical staff. • Decision making problems – information reaching the appropriate people who can make a decision regarding lysis, educational issues regarding lysis – inability to make decisions, other systems interfering / delaying lysis ie: PTCA access system, patient decision making regarding consent to lysis • Where problems identified – redesign system, with assistance of other stakeholders ie: cardiology, hospital administration where appropriate • Plan for audit of any new system / changes and report back – to close quality improvement loop (b) Strategies to improve time to thrombolysis: • Process: • Ensure rapid, accurate and efficient triage process for chest pain patients eg: Category 2 NTC • Chest pain patients triaged to dedicated monitored area for rapid processing • ECG performed and sighted by senior medical staff member within 10 minutes of arrival • Dedicated nursing and medical staff (with ability to make decisions on lysis) to manage all chest pain patients • Information: • Relevant staff notified of arrival of chest pain patient • ECG sighted by medical staff who can make decisions on lysis • Thrombolysis indications / contraindications readily accessible in treating area for reference • Decision-making: • Education of nursing and medical staff of system (care-tracks) for managing chest pain patients • Education of medical staff making decisions regarding lysis – regarding indications, contraindications etc • Simple to follow consent forms / procedure for patients • Ensure care-track streamlines with any care-track for primary PTCA access • Continual quality improvement – audit what you do SAQ 312 You are a newly appointed consultant at a major referral hospital. The director asks you work on a solution to the "access block" problem that exists in your department. Outline your approach to this problem. Definition: Access block has been defined by the ACHS and ACEM as the percentage of all patients admitted, transferred or dying in the ED where their total ED time exceeds 8 hours. Approach to working on a solution: 1. Gather information: • From director - regarding what they see as the problem / any historical background local and elsewhere / solutions already tried. • Information from other hospitals / literature as to initiatives which have worked on this problem. 2. Determine immediate stakeholders: • Inpatient medical teams, bed managers, nurses on wards, directors of nursing, medical administrators 3. Determine potential fixers: • divisional directors, medical administrators, district manager, health minister 4. Define the problem: • Waiting times in all categories, number of admitted patients waiting for beds, time from patient ready to bed ready, times of ward patient discharges, numbers of patients in ED corridors • Document and graph - actual times, trends from previous years, seasonal variation 5. Make “fixers” aware there is a problem: • Invite them to meet with you. • Present your data including graphs, photos of trolleys in corridors etc • Indicate that such a workplace is “unsafe” for patients, for staff liability, even as a fire hazard. • Indicate that working under conditions of access block is undermining staff morale (sick leave stats / resignations may support this) and impairing patient care (adverse events / critical incidents occurring to patients with prolonged stays in ED) • Make them aware that this is a hospital problem, not just an ED one, as evidenced by its presence in many larger Australian hospitals, and all large US hospitals. 6. Suggest solutions: • A commitment required from management that long term (eg: work practices) and short term strategies (eg: beds reopened and staffed) will be needed, and met. • That “root causes” in your hospital need to be addressed with the immediate stakeholders (from admission process to discharge process). • Other healthcare delivery systems (eg: medihotels, day of surgery admission, short stay wards, chest pain units) will also need consideration to change ED work load. • Develop a policy re: ambulance diversion and a system for going on “alert” prior to access block. 7. Agree to a timetable of implementing changes. 8. Plan to measure the impact of any changes to processes. • Follow up with statistics to show whether real changes have occurred and feedback to administrators. 9. Consider raising profile of this issue • Eg: via occupational health & safety, specialty colleges, AMA, media with director’s guidance / consent. SAQ 154 A 25 year old woman is brought to your Emergency Department after being raped What is your management ? Outline your history, examination and investigations Outline your forensic examination ALTERNATIVE QUESTION A 22yo woman presents following an alleged assault. She is withdrawn and will not discuss the details of the incident. On examination, she has multiple bruises of varying appearance over her body and face. The nursing staff report blood on her underpants while undressing. Describe your assessment of this woman. Exam Q Also see SAQ 155, 175, 369, 442, 482 ISSUES Extreme Sensitivity Open support approach Quiet and private room with no interruptions Same sex nurse/SW (chaperone) Support person to stay with patient throughout - never leave alone Meticulous documentation Don’t shower, change clothes or wash teeth Mx 1. Life Threats 2. Assess physical injury 3. Assess genital injury 4. Psychological support 5. STD prophylaxis 6. Pregnancy prophylaxis 7. Tetanus prophylaxis 8. Gathering of forensic evidence 9. Support contacting Police 10. Ensure safety of patient and children on discharge ASSESSMENT Hx Event, when/where/how/by whom, nature of rape (vaginal/oral/anal), other injuries (head/face/trunk extremeties), alcohol or drug intoxication Forensic hx – showering since ? Changed clothes since ? time of rape O&G Hx – pregnancies, LNMP, last intercourse, contraception PMHx, Meds, Allergies, ADT status ? hx – depression Social hx – DV, dependents safe Except for serious injury, be careful the Ex and Ix do not compromise forensic assessment. Ex Life threats – strangulation, HI, haemoperitoneum, haemothorax General exam – ass inj – defence wounds, bruises O&G exam – injuries – vaginal/anal/oral (abrasions, lacerations, bruises, discharge) Ix For trauma as indicated Bedside BSL, urinalysis (UTI, hematuria) Lab Bloods FBE (Hb) if blood loss Beta-HCG LFT baseline U&E, Cr Coags, G&H if bleeding Check blood type (?anti-D) Serology Hep B&C, HIV, VDRL Baseline, need to rpt inn 3 and 6/12 Swabs high vaginal, cervical (?STD) Imaging as indicated FORENSIC EXAMINATION Should be done by government medical officer (GMO) or experienced forensic doctor Objectives: Proof of sexual contact Consent vs use of foce Identity of assailant External Collect all clothing as evidence Skin any marks including evidence of restraints Loose hair, nail trimmings, skin scrapings, dried blood Comb pubic hair Internal Swabs (vaginal, cervical, +/- rectal, buccal) For sperm: vaginal aspirate – wet mount within 72h Wood light for semen PSA, acid phosphatase within 48h Serology Scrupulous documentation MANAGEMENT 1. Resus/Stabilisation ABC Check obs IV access if needed Injuries: external, genital 2. Specific Treatment Treat external injuries starting with life-threatening (external or internal hemorrhage) IV antibiotics if indicated ADT a. Prevent pregnancy (risk 1%) check beta-HCG (?already pregnant) post-coital contraception within 72h levonogestrel 75mg q12h x 2tabs SE – nausea, vomiting, dizziness, fatigue Prophylactic metoclopramide Advise: will get withdrawal bleed, next period will be late, check beta-HCG in 2/52 b. Prevent local STDs (risk 5%) N. gonorrhea ceftriaxone im 250mg stat Chlamydia doxycycline po 100mg bd 7d Erythromycin if ?pregnant c. Prevent blood-borne STDs HIV discuss starter pack 2 x antiretroviral agents SE – GI, hepatic, cutaneous, heatologic 2/52 course, then FU at ID clinic weigh risk of infection vs risk of treatment HBV if never immunised/sAb levels low: Hep B Ig + commence course of Hep B s Ag x 3 HCV ?interferon (seek advice from ID) 3. Supportive care Analgesia, antiemetic Psychosocial input: social worker, rape counsellor, psyc service, legal services/police Forensic assessment: GMO Family support 4. Disposal Depends on injuries – gynae, medical, surgical, ortho If sent home, ensure tight follow up: LMO – check test results, follow up tests O&G – STDs, pregnancy SW, counsellor SAQ 285 Discuss the advantages and disadvantages of having a chest pain unit Start with general concept For risk stratification using Hx/ECG/pathology TNI and stress testing Advantages Decreased length of stay Decrease in bed days Discharge planning Stress test Managed care plan PR aspect Initiative Disadvantages Set up costs Ownership Poor pt selection Undifferentiated pts being put through a differentiated system will result in stuff-ups (Eg PEs or aneurysms) Variation on question would be setting up a chest pain unit OVERVIEW Used for risk stratification Danger of undifferentiated patient in differentiated system NEEDS Demographics Numbers presenting, admissions, etc LIAISON With Cardiology, Physicians PROTOCOLS Use of TnI & ECG EDUCATION Medical staff Nursing staff STAFFING After hours coverage An 82 year old lady returns to your department 3 days after a fall, comDlaining of ongoing shoulder Dam and bruising. She was seen in your ED soon after the fall by p junior resident. who diagnosed a soft tissue injury after viewing this Xrav, and gave her a broad-arm sling. a) Describe this Xray. b?~ Outline your management. ~.) R shoulder x-ray single view A-P 2 part SNOH fracture with impaction, 50% medial displacement and approx 30 degrees lateral angulation Soft tissue swelling No obvious dislocation on single view (needs nd to exclude posterior). 2 bin) Manaaement issues Patient care and safe disposition Harm minimisation including potential complaint Resident education and supervision Assess x-ray R/V process — missed fracture not detected Documentation. Patient care Full reassessment including 2 view re-xray, extent of bruising. Analgesia. Paracetamol/codeine or morphine titrate to response Collar and cuff u-slab for additional traction patient/relative education reassurance and apology (“miss” will not affect prognosis, broad arm sling appropriate) Discharge home only if safe: “Non-pathological” cause of fall (eg. No syncope) Pain controlled on oral medication Able to cope at home with likely dominant arm in sling Support including additional organised through ED (multidisciplinary) Patient/relatives happy for discharge Follow-up home visit/GP and fracture clinic 1/52. Falls/geriatric clinic as appropriate Otherwise admit ortho/aged care team. Missed fracture Educate (sensitively) resident and assess need for further ortho/ radiology education for individual and group Assess supervision levels and address staffing levels and skill-mix as appropriate Clinical indicator: add to audit. Assess reporting and recall procedures (as 3/7 and patient selfpresented) with aid of radiologists. Institute changes and reassess as quality improvement program Full documentation, including of apologies, to anticipate potential complaint/medico-legal. Discuss your steps in introducing emergency department ultrasound to your department. General comments: This question has a generic component and one specific to ultrasound. It asks what arc thc gcneral principles into introducing and integrating any new technological skill into a department and what that entails As well as what you know about the role of ultrasound in the department. Scoring: 1 point for each major point below. Depending on detail will establish mark out of 10. ., General template of introducing new technology: 1. Establish need and scope- it is assumed that this has been addressed 2. Establish lead person 3. Canvass support from your department 4. Canvass support from other affected departments 5. Purchase of equipment 6. Credentialing and accreditation 7. Education and ongoing skill acquisition g~ Quality assurance and appraisal Specific to EDU (emergency department ultrasound) Recognise that FACEM has policy statements on minimum standards and credentialing. FACEM also has a subcommittee on US Currently US knowledge on syllabus but not essential skill but highly recommended 1. Establish need and scope- it is assumed that this has been addressed Discuss scope of EDU eg FAST, AAA Brief comment on other EDU procedures that are currently not accredited by FACEM eg. DVT, Pelvic, Renal, Biliary, Foreign body but have been performed by United states ED physicians Assess your own department’s needs and whether it will be cost effective i.e. improve length of stay, improve education, trainees satisfaction, reduction in reliance on radiology 2. Establish lead person credentialing Delineate role Adequate expertise and enthusiasm 3. Canvass support from your department Departmental heads Colleagues Nursing staff as they have to work around equipment 4.Canvass support from other affected departments May need close liaison with radiology for further Avoid turf battles and clearly delineate limited role of EDU (not taking over) Support from surgical, o and g services. May share equipment Hospital may have credentialing committee 5. Purchase of equipment Establish needs Address type of probes required, need for Doppler Peripherals eg printer, video Warranty and service agreements Costs and financing (may need to share or borrow equipment initially) Compare companies and involve radiology in examining equipment 6. Credentialing and accreditation Establish minimum requirements for people to use machine i. Often a system of levels /grades DOCUMENTATION of examinations Develop protocols for specific examinations 8. 7. Education and ongoing skill acquisition Establish programs that meet FACEM standards Integrate education component to trainees Establish minimum hours of US performed exams to maintain skills Quality assurance and appraisal Require proctoring of examinations by radiology initially and then accredited emergency physician Address studies and audit program on cost effectiveness and effects on patient Comparison of studies to gold standards eg operations, radiology performed US, post mortems SAQ 7. You are asked to write guidelines to help fast —track the ED care of women in l~ trimester PV bleeding. a) Outline these guidelines b) How would you track the effectiveness of the new guidelines? In general, this question was poorly answered as I think most ofyou ran out of time. Firstly, afew general comments on writing guidelines.’ has to be simple, clear, concise... .for idiots must have strict criteria to rule out certain conditions that are potentially fatal.. in this case, ectopic pregnancy (previous ectopic, previous tubal ligation, shoulder tip pain, unilateral abdo pain, JUD, PID) and cvical shock in incomplete aborts) emphasise that it ‘s a guide to patient management and not a directive, does NOT replace good clinical judgement (for e.g in my head injury guideline I have a waive out clause at the end of the Hlform ~fyou want to go out of guideline) No one mentioned patient advice for patients to return ~f symptoms got worse, or LMO follow up, this should be standard in all patient discharge plans. - - - - Tracking the effectiveness of the guideline really depends on why you created it in the first place. to decrease waiting times to improve safety and reduce adverse events to improve discharge plannng to improve patient satisfaction reduce pathology ordering You monitor the outcomes of whatever you set out the guideline for. Need some sort of comparison, so, have a historical control prior to guideline and a prospective audit post guideline. Need to also measure compliance rate of guideline i.e how many doctors and nurses are using it and ~f they are using it correctly. - - - - - a) Guideline for 1st trimester PV bleeding includes: 1. TRIAGE and GP REFERRALS Confirm pregnancy if not already done with blood / urine test. Normal triage procedure with assessment of vital signs and degree of pain and bleeding. Triage catergory assigned BUT should be highlighted as 1St trimester PV bleeding for possible fast tracking if resources allow. Relevant blood tests performed pHCG, blood group (fFBE I personally don ‘tfind this useful, but it is in MMC ‘s guideline) - - - - 2. MEDICAL ASSESSMENT Directed O&G history in particular past pregnancies, miscarriages, ectopics, gynaecological procedures, contraception, ectopic risk factors (previous ectopic, PD, IUID, tubal ligation, any unilateral pain) has an intrauterine pregnancy been confirmed for this pregnancy on US? assess severity of bleeding and or pain. Examine patient, check vital signs, abdo and pelvic exam. Suspect ectopic if unilateral pain, adnexal tenderness (or mass) and cervical motion tenderness. Check for POC at os. (assessing wheteher the os is opened or closed is useless) - - - - 3. MANAGEMENT (i) Unstable resuscitate, (ii) In pain: analgesia (iii) Suspect ectopic : refer to O&G first then US if patient stable otherwise to OR. (iv) Ideally, all should have US to check viability of foetus, retained products or missed abortion. This can be done non-urgently and arranged for the next day and the patient to be followed up in EPB (Early pregnancy bleeding) clinic. If the patient needs admission for pain, bleeding or surgery, then an urgent US may need to be done. (v) Unstable patients : referred to O&G and admitted. (vi) All discharged patients should be given advice and follow up instructions on when to return if symptoms worsen. (vii) Anti-D in Rh (-)ve patients. (viii) Counselling re miscarriages. b) Tracking the effectiveness of the new guideline 1. Historical control / retrospective chart review of patients pre guideline. 2. Prospective audit of guideline compliance rate and correct use of guideline. 3. Monitor outcome measures of interest: waiting times adverse events or missed diagnosis -patient satisfaction amount of pathology ordered time effectiveness of triage-treatment-discharge times feedback from O&G, GP, radiology and ED doctors and nurses - - - - - You are the director of a tertiary level ED. You receive a complaint from a patient who states he is making legal enquiries regarding a bad experience he had in your department. He states he heard a doctor informing other doctors about his condition. During the conversation there was laughing and giggling at his expense. He felt embarrassed and was ashamed to discuss his condition any further with anybody else. Priorities 1. 2. 3. 4. 5. 6. Ensure safety with possible incomplete assessment apologise investigate discipline staff as necessary inform hospital insurer and complaints department take steps to prevent recurrence education re confidentiality/privacy department layout cultural change 7. ensure that this process is agreed to by the patient and does not lead to further embarrassing disclosure (letter opened by wife.. .We apologise for the incident, it was just the buzzing sound that set us all of) Response to complaint Recognise as serious legitimate complaint with privacy and confidentiality issues Rapid initial contact. Apologise without admitting guilt Establish rapport Non judgemental approach Obtain more info regarding events Ask for complaint in writing. Document all conversations Interview staff Offer patient his own advocate/ access to complaints department. State that you would like to properly investigate the matter and that you will make contact with responce After investigation take steps as indicated. Inform hospital insurer Discipline staff Formal apology after liason with legal staff Ask what steps the patient fells he would like taken (may or may not be reasonable. Steps to prevent recurrence Consider a committee approach Medical Nursing Legal or privacy officer Administration Define the problem eg. Breach of confidentiality in the ED Investigate the causes and possible remedies Literature search Visit other departments Hospital insurers max have resources Enquire as to whether there is funding to tackle the problem (eg. The insurer may be a sponser) Collect data on confidentiality issues/breaches in the department Note other areas of potential breaches eg. Pt information displayed on “whiteboards”. Look into underlying causes of problems e.g. Cynicism or black humour reflecting poor morale! burnout poor rostering, work load or supervision. Institute changes Eg. Department layout with tea rooms separate from patient areas Hand-over areas Screening of phone conversations. You are a consultant in a tertiary hospital emergency department. The director asks you to assess means by which departmental investigation costs might be reduced. Discuss your approach. Answer provided by Graeme Thompson: TEAM APPROACH The first thing to do is to assemble a multi-disciplinary team. Select team members who are: Available to give some time, Able to mtluence others Include representatives from diagnostic imaging and laboratory medicine Have an interest in the problem The team should be small enough to be cohesive and manageable. Set up smaller teams with tasks. Enquire if a budget is available (e.g. for external help) MEETINGS Arrange tbr regular meetings Keep good records including attendance records Set out clear goals Ensure that minutes are circulated Decide on a timeframe and try to adhere to it APPROACH TO PROBLEM Assemble information on current activity and costs, broken down in detail to give an accurate picture of individual test ordering Try to ascertain who orders tests Find out if current test ordering is protocol driven or left to individuals. Ascertain ‘best practice’ Literature search Visits, discussions with people from other hospitals where it is thought that costs have been well contained. Find money for site visits Using a Delphi approach discuss the various aspects of best practice that may be useful in your situation -some aspects may be impractical -using the same approach decide on the individual tests that you will target. These may be the most common, or the most expensive or the most inappropriately ordered. Decide if you want to reduce overall demand by having tests ordered elsewhere. For example have woman needing non urgent ultrasounds go back to GP’s to have them ordered or have many of the tests ordered after patients are admitted, not from ED These approaches will need wider consultation and dissemination of information to inpatient units andior GPts. IMPLEMENTATION Once your approach is decided upon, tell everyone concerned what you are planning to do Use non-threatening ways including lunches, teaching sessions and posters. Implement changes and monitor compliance, progress and actual savings Gather feedback from staff and other users Modify your approach based on progress and feedback 6. In response to a high level of sick leave taken by medical staff in your ED, consultant staff decide to look at strategies to reduce the level and impact of sick leave. Describe the issues involved. 5) The CEO of your tertiary ED states an intention to have ED consultants work night shifts and requests your opinion. Outline your response. 2. What features would you want in a patient trolley (bed) for a resuscitation area? Justify your answer. 1. Strong – up to 180kg patient, able to withstand CPR 2. Mobile – multidirectional wheels with unidirectional lock capability (+ all lock) rubber fenders 3. Adjustable – patient sitting, 0-90O all positions Trendelenburg and head up Height of bed Hydraulic assistance so easy to adjust, ergonomic issues to prevent staff injury 4. Compatible – with resusc, ICU, CT areas, easy to manoeuvre, light Xray – space for film cartridges for trauma and other views 5. Attachments – drip pole at 4 corners Equipment tray at foot end Extendable for tall patients Removable bed ends O2 cylinders Tray underneath for clothes, notes etc 6. Cost effective 1. Your department receives a series of complaints from relatives of patients who die in the ED regarding the care and information offered to them. Outline the way in which you would improve the standard of care offered to relatives of these patients in your department. ‘ 2.) You are appointed as a fellow with a non-clinical role in a large academic emergency department. Outline methods by which you could increase the use of evidence in clinical decision making within your department. 7.) Diseu.ss the role of emergency (lepartment short-stay wards. i. You wish to implement the use of bedside ultrasound by Emergency staff in your department. Outline the process of implementation. 2.) A 75 year old lady is brought in from home having fallen. An x-ray ordered by the triage nurse shows a fractured neck of femur. She refuses to be admitted saying that she just wants to go home and that it will heal eventually. 2.) You are the director of a tertiary hospital Emergency Department. You receive a complaint from a patient who states he is making legal enquiries regarding a bad experience he had in your department. He states that he heard a doctor informing other doctors about his condition. During the conversation there was laughing and giggling at his expense. He felt embarrassed and was ashamed to discuss his condition any further with anybody else. Outline your response. 5.) You are the director of a rural department. Your registrar asks that the department stock a new drug, B, in preference to the existing drug A, for the treatment of myocardial infarction. She states that she has read an article in which the use of drug B is associated with a statistically better outcome than A, and that the p value is less than 0.05 The cost of drug A is $50 and that of B is $300. SAQ1. Thomas Chan Discuss your steps in introducing emergency department ultrasound to your department. General comments : This question has a generic component and one specific to ultrasound. It asks what are the general principles into introducing and integrating any new technological skill into a department and what that entails As well as what you know about the role of ultrasound in the department. Scoring : 1 point for each major point below. Depending on detail , will establish mark out of 10. General template of introducing new technology: 1. Establish need and scope- it is assumed that this has been addressed 2. Establish lead person 3. 4. 5. 6. 7. 8. Canvass support from your department Canvass support from other affected departments Purchase of equipment Credentialing and accreditation Education and ongoing skill acquisition Quality assurance and appraisal Specific to EDU (emergency department ultrasound) Recognise that FACEM has policy statements on minimum standards and credentialing. FACEM also has a subcommittee on US Currently US knowledge on syllabus but not essential skill but highly recommended 1. Establish need and scope- it is assumed that this has been addressed Discuss scope of EDU eg FAST, AAA Brief comment on other EDU procedures that are currently not accredited by FACEM eg. DVT, Pelvic, Renal, Biliary, Foreign body but have been performed by United states ED physicians Assess your own department’s needs and whether it will be cost effective i.e. improve length of stay, improve education, trainees satisfaction, reduction in reliance on radiology 2. Establish lead person Delineate role Adequate expertise and enthusiasm 3. Canvass support from your department Departmental heads Colleagues Nursing staff as they have to work around equipment 4. Canvass support from other affected departments May need close liaison with radiology for further credentialing Avoid turf battles and clearly delineate limited role of EDU (not taking over ) Support from surgical, o and g services. May share equipment Hospital may have credentialing committee 5. Purchase of equipment Establish needs Address type of probes required, need for Doppler Peripherals eg printer, video Warranty and service agreements Costs and financing (may need to share or borrow equipment initially) Compare companies and involve radiology in examining equipment 6. Credentialing and accreditation Establish minimum requirements for people to use machine i. Often a system of levels /grades DOCUMENTATION of examinations Develop protocols for specific examinations 7. Education and ongoing skill acquisition Establish programs that meet FACEM standards Integrate education component to trainees Establish minimum hours of US performed exams to maintain skills 8. Quality assurance and appraisal Require proctoring of examinations by radiology initially and then accredited emergency physician Address studies and audit program on cost effectiveness and effects on patient Comparison of studies to gold standards eg operations, radiology performed US, post mortems.