A RARE CASE OF CARPAL MELORHEOSTOSIS ABSTRACT
advertisement

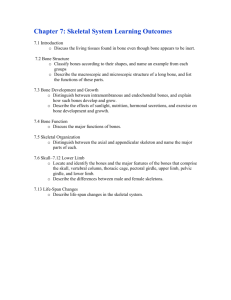
A RARE CASE OF CARPAL MELORHEOSTOSIS ABSTRACT Melorheostosis is a rare, non-inheritable sclerotic bone dysplasia. We report a rare case of melorheostosis involving the carpal bones of a 9 years old male who presented with pain in right wrist joint on palmar flexion. Plain radiograph and CT performed revealed characteristic appearance of melorheostosis involving the scaphoid, lunate and trapezium. CASE REPORT A 9 Years old male child presented with complaints of persistent pain in right wrist joint over 1 month with limitation palmar flexion of the wrist. On physical examination the terminal extenet of palmar and dorsi flexion of the right wrist joint were restricted. Grip strength of right wrist is maintained. There was no significant limitation of daily activities. Plain radiographs revealed hyperostosis of the scaphoid,lunate and trapezium involving both the cortex and medulla. There was no significant periosteal reaction. The carpal joint spaces were maintained. No obvious erosions / lytic lesions were noted. Computed tomography (CT) scans showed a high attenuation involving cortical hyperostosis. Biochemical analysis including serum calcium, phosphorus, alkaline phosphatase, C-reactive protein and erythrocyte sedimentation rate revealed no significant abnormality. A core biopsy was taken form the scaphoid and histopathological analysis revealed nonspecific, dense cortical bone replacing the trabacular system. DISCUSSION: Melorheostosis is a rare non hereditary sclerosing bone dysplasia first described by the two French neurologists Leri and Joanny in 1922 (1). The origin of the word melorheostosis is from a combination of the Greek words ‘melo’ meaning 'limb', ‘rheos’ meaning 'flow' and ‘osteon’ meaning 'bone' (2). This was in reference to the classic appearance on plain radiographs where the sclerosis appears to flow along the long axis of the bone, akin to candle wax dripping down one side of a candle. Pathologically, this condition comprises of new bone formation on the periosteal and endosteal layers of the diaphyseal cortical bone. Typically, this is seen as irregular sclerosis olong one side of a long bone. This condition most often affects the long bones of both the upper and lower extremities but may rarely affect small bones of the hands and feet or even the axial skeleton (3). Within the hand, the short long bones like phalanges and metacarpals are usually involved and isolated involvement of the carpal bones is very rare. The exact cause of this condition is yet unknown. However, several theories have been proposed including a genetic mutation involving the LEMD3 gene , an embryonal mesodermal disorder, a vascular abnormaltiy and even infection of associated nerve roots (4). The last theory was probably proposed to explain the common occurrence of this disorder in particular sclerotomes. Several patterns of melorheostosis have been described including the monostotic (involving one bone), polysototic (involving multiple bones) and the most common monomelic (involving one limb). Within a limb, melorheostosis is usually confined to a single sclerotome and even within a particular sclerotome, the lesions may cross the joint space to involve bones on either side but the intervening joint is usually not involved (5). Melorheostosis is often associated with various cutaneous manifestations overlying the involved bones including focal scleroderma, neurofibromatosis, various vascular and lymphatic malformations including telengiectasias. These skin changes usualllly parallel the bone involvement and are often restricted to the involved sclerotome (6). Clinically, melorheostosis is a chronic disorder with slow progression of symptoms. The usual presentation is with pain, joint stiffness, muscle contracture, limitation of motion, soft tissue abnormalities or progressive deformity (7). It has no sex prediliction and over 50% of the patients are diagnosed before the age of 20 years (8). The diagnosis of melorheostosis is usually based on classical imaging findings alone and a biopsy is usally not required. Also, histopathological analysis is most often not diagnostic. On plain radiographs, there is increased bone density and the hyperostosis is classically present along the cortical aspect of one side of bone resembling flowing candle wax – the 'dripping candle wax' sign (9). In carpal and tarsal bones and in the epiphysis of long bones, the hyperostosis maybe round or irregular, as in our case. The CT appearance is similar to the typical undulating hyperostosis seen on radiographs (10). These lesions appear well demarcated from the normal bone. On MR examination, sclerosis appears of low in signal intensity on both T1 and T2 wighted images. CT and MRI further help in delineating the soft tissue changes. The radiological differential disgnoses include osteopoikilosis, osteopetrosis, arthrogryposis multiplex congenita, and osteopathia striata (11). Radionuclide bone scan maybe useful in differentiating melorheostosis from its mimics by demonstrating increased radiotracer uptake in the involved bones on blood pool as well as delayed phases in this condition (12). When it affects the carpal bones, as in our case, the differential diagnosis would broaden to include other causes of carpal boen sclerosis including kienbock's disease, rhematoid arthritis, chronic infections like tuberculosis, etc and often histopathology maybe required to rule out these conditions. Melorheostosis is a benign condition and usually does not need treatment. However, bisphosphonates have been reported to provide significant symptomatic relief by decreasing the bone turnover (13). CONCLUSION Although melorheostosis is a relatively easy diagnosis to make radiologically when it involves long bones, it maybe very difficult to diagnose involevement of small bones of the hands and feet. It is very important for radiologists and clinicians to be aware of this condition and its radiological appearance so as to maek an early diagnosis and avoid unecessary intervention. REFERENCES: 1) Ethunandan M, Khosla N, Tilley E, Webb A. Bone dysplasia series. Melorheostosis: review and update. J Craniofac Surg. 2004 Nov;15(6):1062-5. PMID: 15547407. 2) van Durme CM, Starmans-Kool MJ, Peeters HR. Dripping candle wax. Neth J Med. 2012 Apr;70(3):140, 143. PMID: 22516580. 3) Greenspan A, Azouz EM. Bone dysplasia series. Melorheostosis: review and update. Can Assoc Radiol J. 1999 Oct;50(5):324-30. PMID: 10555508. 4) Al Kaisii A, Skoumal M, Roetzer K, Grill F, Klaushofer K. A patient with melorheostosis manifesting with features similar to tricho-dento-osseous syndrome: a case report. J Med Case Rep. 2008 Feb 19;2:51. PMID: 18284671. 5) Hai-Tao Long MD, Kang-Hua Li MD,Yong Zhu MD Severe Melorheostosis Involving the Ipsilateral Extremities Clin Orthop Relat Res (2009) 467:2738–2743. 6) Kim J, Cho SB, Cho S, Bang D. Unilateral nevoid telangiectasia associated with ipsilateral melorheostosis. Ann Dermatol. 2012 May;24(2):206-8. PMID: 22577274. 7) Saadallaoui Ben Hamida K, Ksontini I, Rahali H, Mourali S, Fejraoui N, Bouhaouala H, Charfi MR, Dougui MH. Atypical form of melorheostosis improved by pamidronate. Tunis Med. 2009 Mar;87(3):204-6. PMID: 19537015. 8) Masquijo JJ, Allende V. Melorheostosis of the hand in a pediatric patient. Arch Argent Pediatr. 2010 Dec;108(6):e121-5. PMID: 21132236. 9) Bansal A. The Dripping Candle Wax Sign. Radiology 2008 Feb;246(2):638-40. PMID: 18227553. 10) Motimaya AM, Meyers SP. Melorheostosis involving the cervical and upper thoracic spine: radiographic, CT, and MR imaging findings. AJNR Am J Neuroradiol. 2006 Jun-Jul;27(6):1198-200. PMID: 16775263. 11) Schreck MA. Melorheostosis in a pediatric patient. J Podiatr Med Assoc. 2005 MarApr;95(2):167-70. PMID: 15778476. 12) Izadyar S, Gholamrezanezhad A. Bone scintigraphy elucidates different metabolic stages of melorheostosis. Pan Afr Med J. 2012;11:21. PMID: 22514755. 13) Hollick RJ, Black A, Reid D. Melorheostosis and its treatment with intravenous zoledronic acid. BMJ Case Rep. 2010;2010. PMID: 22479293. FIGURE LEGEND: CT Scan of right wrist joint of 9 year old male child showing hyperostosis of the scaphoid, lunate and trapezium. A – Scout (AP), B – VRT, C – CT sagittal, D – CT axial and E – CT coronal.