action plan - ESRD Network 17
advertisement

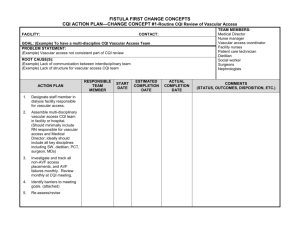
NETWORK 17 CQI ACTION PLAN-CHANGE CONCEPT #1: Routine CQI Review of Vascular Access FACILITY: TEAM MEMBERS: Medical Director / Nephrologist CONTACT: Nurse Department Manager (NDM) GOAL: Asst. Nurse Dept. Manager (ADM) 1. To designate a Vascular Access Coordinator who will have allocated time to focus on Vascular Access Clinical Educator tracking. PI Representatives 2. To create/revise a form that contains all the necessary information and can be utilized by all dialysis staff to Vascular Access Coordinator (VAC) investigate and track all non-AVF access placements and AVF failures Facility Nurses PROBLEM STATEMENT: Patient Care Technicians 1. The PI Representatives are not solely the Vascular Access Coordinators. Dietitian 2. There is no complete form that contains all the necessary information that the CQI team as well as the Social Worker dialysis staff can input information as pertinent information arise for the investigation and tracking of all nonAVF access placements and AVF failures. ROOT CAUSE(S): 1. Lack of personnel for the amount of work present. 2. Lack of structure for the vascular access CQI team. 3. Lack of communication between dialysis staff and interdisciplinary team. ESTIMATED ACTUAL RESPONSIBLE START COMMENTS ACTION PLAN COMPLETION COMPLETION TEAM MEMBER DATE (STATUS, OUTCOMES, EVALUATION, ETC.) DATE DATE 1. Designate a staff member in the dialysis facility responsible for vascular access and allocate time to focus on vascular access CQI. NDM ADM Clin. Educ. PI Rep. 12/28/09 1/22/10 2. Review current form being used to track vascular access. NDM ADM PI Rep. 12/18/09 12/28/09 12/18/09 12/28/09 3. Determine the need for a NDM new form that contains all ADM the necessary information and can be utilized by all dialysis staff to investigate and track all non-AVF access placements and AVF failures. NETWORK 17 1. A Staff Nurse 5 Clinical Educator position has been approved. The DM and ADM are waiting for a list of applicants to begin the interview process. The SN V Clin. Educ. will be the Vascular Access Coordinator. 2. There are two vascular access forms currently being utilized to track permanent vascular access placement. 3. Determine if PCTs are reporting fistula/graft problems to the team leaders. Determine if the team leaders in return are following through and taking appropriate steps to correct or prevent future fistula/graft problems. CQI ACTION PLAN – CHANGE CONCEPT #2 – Timely Referral to Nephrologist FACILITY: CONTACT: GOAL: 1. Patients needing pre-ESRD care are referred to the Nephrologist in a timely manner. PROBLEM STATEMENT: 1. Patients are not referred timely to the Nephrologist for pre-ESRD care. ROOT CAUSE(S): 1. Lack of compliance with education material provided to primary care physicians and clinicians by the nephrologist. 2. Limited multi-disciplinary approach to pre-ESRD care. ACTION PLAN RESPONSIBLE TEAM MEMBER START DATE ESTIMATED COMPLETION DATE ACTUAL COMPLETION DATE TEAM MEMBERS: Hospital Medical Director Primary Care Physicians Physician Extenders (NP, PA) Medical Director / Nephrologist CKD Clinic Nurse CKD Clinic Medical Assistant Nurse Department Manager (NDM) Asst. Nurse Dept. Manager (ADM) PI Representatives Vascular Access Coordinator (VAC) COMMENTS (STATUS, OUTCOMES, DISPOSITION, ETC.) 1. Encourage PCPs to utilize ESRD/CKD referral criteria to ensure timely referral of patients to the nephrologist. 2. CKD clinic RN/MA to support nephrologist to document AVF plan for all patients expected to require renal replacement therapy. Hosp. Medical Director Nephrologist 1/4/10 2/26/10 1. Hospital Medical Director and Nephrologist to present the importance of early referral to various committees where PCPs, house staff and attending physicians are in attendance. 2. NDM to meet with Ambulatory Care Services (ACS) Director to discuss CKD Clinic RN and/or MA responsibility. Nephrologist NP, PA ACS Director CKD Clinic RN CKD Clinic MA NDM ADM PI Rep. VAC 1/7/10 1/22/10 3. Coordinate with CKD clinic RN/MA to educate patients and family on benefits of AVF and to protect vessels. NDM ADM PI Rep. VAC Clin. Educ. 1/7/10 1/22/10 3. NDM to meet with Ambulatory Care Services (ACS) Director to discuss CKD Clinic RN and/or MA responsibility. 4. Consider using a Hospital 1/4/10 2/26/10 4. Hospital Medical Director and physician extender (NP, PA) to provide vascular access education, referral, and support in the CKD clinic. Medical Director Nephrologist ACS Director NDM ADM PI Rep. VAC Clin. Educ. Nephrologist will meet with ACS Director to discuss physician extender responsibility. NETWORK 17 CQI ACTION PLAN – CHANGE CONCEPT #3 – Early Referral to Surgeon for “AVF only” Evaluation and Timely Placement FACILITY: CONTACT: GOAL: 1. Patients needing pre-ESRD care are referred to the Nephrologist in a timely manner. PROBLEM STATEMENT: 1. Patient not referred to surgeon timely for “AVF only” evaluation and placement. ROOT CAUSE(S): 1. Limited or no patient pre-ESRD care. 2. Lack of structured referral system. 3. Lack of nephrologist-surgeon partnership. ACTION PLAN RESPONSIBLE TEAM MEMBER START DATE ESTIMATED COMPLETION DATE 1. Support nephrologist / nurse to perform appropriate evaluation and exam prior to surgeon referral before dialysis or within 90 days of HD start. Nephrologist ACS Director NDM ADM CKD Clinic RN CKD Clinic MA VAC Clin. Educ. 1/7/10 1/22/10 2. Support nephrologist to refer patient for vessel mapping prior to surgeon referral before dialysis or within 90 days of HD start. 3. Support nephrologist to refer to surgeon for “AVF only” no later than Stage IV, GFR <30. 4. Support nephrologist to define expectations to surgeon, including vessel mapping. 2-4. Nephrologist NDM ADM VAC Clin. Educ. Social Worker 1/7/10 1/22/10 5. If pre-dialysis AVF Hospital 1/4/10 ACTUAL COMPLETION DATE TEAM MEMBERS: Hospital Medical Director Physician Extenders (NP, PA) Medical Director / Nephrologist CKD Clinic Nurse CKD Clinic Medical Assistant Nurse Department Manager (NDM) Asst. Nurse Dept. Manager (ADM) PI Representatives Vascular Access Coordinator (VAC) Social Worker COMMENTS (STATUS, OUTCOMES, DISPOSITION, ETC.) 1. NDM to meet with Ambulatory Care Services (ACS) Director to discuss CKD Clinic RN and/or MA responsibility. 3-4. Customize referral letters to surgeons for “AVF only “evaluation and placement. 2/26/10 5. Hospital Medical Director and placement does not occur, support nephrologist and/or house staff to order AVF evaluation and placement at initial hospitalization for HD start. Medical Director Nephrologist NDM ADM VAC Clin. Educ. Social Worker Nephrologist to present AVF evaluation and placement to various committees where house staff and attending physicians are in attendance. NETWORK 17 CQI ACTION PLAN – CHANGE CONCEPT # 4 -Surgeon selection based on best outcomes, willingness, and ability to provide access services FACILITY: CONTACT: GOAL: 1. Patients are referred to surgeons with best outcomes for AVF placement. PROBLEM STATEMENT: 1. Surgeon referral and selection not based on best AVF outcomes. ROOT CAUSE(S): 1. Limited surgeon referral sources. 2. Limited surgeon education and/or experience with AVF procedures. 3. Surgeon referral based upon facility preferences. ACTION PLAN RESPONSIBLE TEAM MEMBER START DATE ESTIMATED COMPLETION DATE 1. Support nephrologist to Hospital communicate Medical expectations to surgeons Director performing vascular Nephrologist access. ACS Director NDM ADM CKD Clinic RN CKD Clinic MA VAC Social Worker 1/4/10 2/26/10 2. Support nephrologist to refer to surgeons willing and able to meet the standards and expectations. 1/7/10 1/22/10 Nephrologist NDM ADM Clin. Educ. VAC PI Reps. TEAM MEMBERS: Hospital Medical Director Vascular Surgeons Medical Director / Nephrologist CKD Clinic Nurse CKD Clinic Medical Assistant Nurse Department Manager (NDM) Asst. Nurse Dept. Manager (ADM) PI Representatives Vascular Access Coordinator (VAC) Social Worker ACTUAL COMPLETION DATE COMMENTS (STATUS, OUTCOMES, DISPOSITION, ETC.) 1. Hospital Medical Director and Nephrologist to present AVF evaluation and placement to various committees where house staff and attending physicians are in attendance. Customize referral letters to surgeons for “AVF only “evaluation and placement. Hospital Medical Director and Nephrologist to present AVF evaluation and placement to various committees where surgeons are in attendance. NDM to meet with Ambulatory Care Services (ACS) Director to discuss CKD Clinic RN and/or MA responsibility. 2. Create referral letter. 3. Evaluate surgeon selection on frequency, quality and patency of access placement. 4. Conduct data collection ongoing at dialysis facility on surgeon procedures performed and results. Report data monthly at CQI meeting. VAC PI Reps. 1/4/10 Ongoing 3. Create audit tool. VAC PI Reps. 1/4/10 Ongoing 4. Create audit tool and include data in monthly CQI meeting. NETWORK 17 CQI ACTION PLAN – CHANGE CONCEPT # 5 - Full range of appropriate surgical approaches to AVF evaluation and placement FACILITY: TEAM MEMBERS: Vascular Surgeons CONTACT: Medical Director / Nephrologist GOAL: Nurse Department Manager (NDM) 1. All attempts/approaches to AVF evaluation and placement are made. Asst. Nurse Dept. Manager (ADM) PROBLEM STATEMENT: 1. Surgical approaches offered by surgeon/dialysis facility are limited; patients are not considered candidates for PI Representatives Vascular Access Coordinator (VAC) AVF Hospital Unit Clerk ROOT CAUSE(S): 1. Limited education/experience of surgeon 2. Limited surgeon referral source. 3. Limited resources/locations for surgeon to expand techniques offered. ESTIMATED ACTUAL RESPONSIBLE START COMMENTS ACTION PLAN COMPLETION COMPLETION TEAM MEMBER DATE (STATUS, OUTCOMES, DISPOSITION, ETC.) DATE DATE 1. Provide education to surgeon through CD/DVD and/or mentorship available from network, i.e. expanded surgical procedures and patient criteria eligible for AVF. 2. Ensure venous mapping is completed for all patients needing permanent vascular access. Nephrologist Vascular Access Coordinator Clin. Educ. PI Reps. 1/4/10 2/26/10 1. Obtain and reproduce educational material. Nephrologist NDM ADM Clin. Educ. Vascular Access Coordinator PI Reps. HUC 3. Partner nephrologist, Nephrologist facility vascular access Surgeon coordinator, and surgeon VAC to evaluate current AVG PI Reps. patients for secondary AVF. 4. Send facility comparative VAC 1/4/10 Ongoing 2. Review records of all patients still needing permanent vascular access. 1/4/10 Ongoing 3. Review of patients who currently have AVG. 1/4/10 Ongoing surgeon data to surgeons not performing expanded techniques. (i.e. vein transposition). PI Reps. NETWORK 17 CQI ACTION PLAN – CHANGE CONCEPT # 6 – Secondary AVF placement in patients with AV Grafts FACILITY: CONTACT: GOAL: 1. Patients with AVG are identified for potential placement of AVF. PROBLEM STATEMENT: 1. Patients are not properly evaluated for possible secondary AVF. ROOT CAUSE(S): 1. Higher successful placement of AVG. 2. Surgeon preference for placing AVG. ACTION PLAN 1. Support nephrologist and vascular access coordinator to evaluate every AVG patient for possible secondary AVG placement. 2. Educate dialysis staff and vascular access coordinator to examine outflow vein of all AVG patients during dialysis treatments at least monthly. Identify patients who may be suitable for elective secondary AVG conversion in upper arm and notify nephrologist of patient list. 3. Support nephrologist to refer eligible patients to surgeon before AVG failure. 4. Document vascular access plan of care for all patients currently using a graft for dialysis. RESPONSIBLE TEAM MEMBER Nephrologist Vascular Access Coordinator Primary RNs Clin. Educ. Vascular Access Coordinator PI Reps. Nephrologist Vascular Access Coordinator Primary RNs Primary RNs VAC START DATE TEAM MEMBERS: Medical Director / Nephrologist PI Representatives Vascular Access Coordinator (VAC) Primary Nurses ESTIMATED COMPLETION DATE 1/4/10 Ongoing 1/4/10 Ongoing 1/4/10 Ongoing 1/4/10 Ongoing ACTUAL COMPLETION DATE COMMENTS (STATUS, OUTCOMES, DISPOSITION, ETC.) 1-3. Ongoing assessment of patients with AVG. 4. Monthly Primary Nurse responsibility. NETWORK 17 CQI ACTION PLAN – CHANGE CONCEPT # 7 – AVF Placement in Patients with Catheters where Indicated FACILITY: TEAM MEMBERS: Medical Director / Nephrologist CONTACT: PI Representatives GOAL: Vascular Access Coordinator (VAC) 1. Decrease the occurrence of patients with catheters and facilitate the placement of AVFs in this population. Primary Nurses PROBLEM STATEMENT: Clinical Educator 1. Facility has high occurrence of catheters. Hospital Registration ROOT CAUSE(S): 1. High catheter placement for prevalent and/or incident patients. 2. Limited time prior to dialysis for nephrologist and/or surgeon referral. 3. Patient preference. 4. Patient insurance coverage/status. 5. Lack of patient education. ESTIMATED ACTUAL RESPONSIBLE START COMMENTS ACTION PLAN COMPLETION COMPLETION TEAM MEMBER DATE (STATUS, OUTCOMES, DISPOSITION, ETC.) DATE DATE 1. Evaluate all catheter patients for AVF, regardless of previous access. Include vein mapping in evaluation. 2. Implement protocol to track all catheter patients for removal of catheter. 3. Investigate and track all catheter placements monthly and report to QI team. 4. Document vascular access plan of care for all patients currently using a catheter. 5. Educate and follow up with catheter patients monthly to support placement of permanent vascular access. Nephrologist VAC PI Reps. Primary RNs Ongoing Ongoing 1. Primary RNs to include evaluation in monthly progress notes. VAC PI Reps. Primary RNs 1/18/10 2/1/10 2. Create protocol to track all catheter patients for removal of catheter. VAC PI Reps. Ongoing Ongoing VAC Primary RNs Ongoing Ongoing 3. Utilize Fistula First Data Collection Tool to track catheter placements and report to QI team. 4. Primary RNs to document vascular access plan of care in the monthly progress notes. Clin. Educator VAC PI Reps. Primary RNs 1/18/10 Ongoing 5. Schedule monthly classes to educate patients and provide support for placement of vascular access. 6. Track insurance VAC 1/18/10 Ongoing 6. Hospital registration to provide coverage/status and PI Reps. determine steps needed Social Worker to obtain full scope Hospital coverage. Registration dialysis unit with an updated list of insurance coverage. NETWORK 17 CQI ACTION PLAN – CHANGE CONCEPT # 8 – Cannulation Training for AV Fistulas FACILITY: TEAM MEMBERS: Medical Director / Nephrologist CONTACT: PI Representatives GOAL: Vascular Access Coordinator (VAC) 1. More training on AVF and AVG cannulation will be provided to the staff. Clinical Educator PROBLEM STATEMENT: Charge Nurses 1. Staff has limited continuous cannulation training and the best teaching tools are not used/available. Social Worker ROOT CAUSE(S): 1. There is no consistent scheduling of best cannulators on both patient shifts. 2. Staff has limited exposure to AVG or AVF cannulation needs due to high occurrence of catheters. 3. Limited or sub-optimal surgical technique. ESTIMATED ACTUAL RESPONSIBLE START COMMENTS ACTION PLAN COMPLETION COMPLETION TEAM MEMBER DATE (STATUS, OUTCOMES, DISPOSITION, ETC.) DATE DATE 1. Identify and use the best cannulators and best teaching tools (e.g. videos, dummy fistula arm) to teach AVF cannulation to all appropriate dialysis staff. Provide cannulation training on a continuous basis. 2. Implement protocol for initial dialysis treatments for new AVFs and assign the most skilled staff to such patients. 3. Create a selfcannulation program and offer the option of self-cannulation to patients who are interested and able. NDM ADM Clin. Educ. VAC 2/1/10 Ongoing 1. Obtain best teaching tools and schedule cannulation training on a regular basis. NDM ADM Clin. Educ. VAC Charge Nurses 2/1/10 Ongoing 2. Review protocol for initiating dialysis treatment on new AVFs. Adjust schedule as necessary to schedule skilled staff on the shift of patients with new AVFs. NDM ADM Clin. Educ. VAC Social Worker 2/1/10 2/22/10 3. Create a course outline for a self-cannulation program. NETWORK 17 CQI ACTION PLAN – CHANGE CONCEPT # 9 – Monitoring and Maintenance to Ensure Adequate Access Function FACILITY: CONTACT: GOAL: 1. More training on AVF and AVG cannulation will be provided to the staff. PROBLEM STATEMENT: 1. Inadequate monitoring and surveillance to ensure adequate vascular access function. ROOT CAUSE(S): 1. Limited staff experience and/or knowledge with vascular access monitoring technique. 2. Lack of protocols in place for monitoring and surveillance of vascular access. 3. Lack of appropriate use of data collected from vascular access surveillance. 4. Lack of multi-disciplinary approach to vascular access surveillance and monitoring. ESTIMATED ACTUAL RESPONSIBLE START ACTION PLAN COMPLETION COMPLETION TEAM MEMBER DATE DATE DATE 1. Support nephrologist and surgeon to conduct post-operative exam of AVF at 4 weeks to detect early signs of failure and refer for interventions as needed. 2. Adopt standard procedures for monitoring, surveillance, and timely referral if indicated in the dialysis facility. 3. Support nephrologist and surgeons to adopt standard criteria to determine the appropriate extent of intervention on existing access before placing new access. 4. Develop vascular access plan of care for TEAM MEMBERS: Medical Director / Nephrologist Surgeon NDM ADM Clinical Educator PI Representatives Vascular Access Coordinator (VAC) Primary Nurses QI Team COMMENTS (STATUS, OUTCOMES, DISPOSITION, ETC.) Nephrologist Surgeon NDM ADM VAC PI Reps. 1/4/10 Ongoing Nephrologist NDM ADM Clin. Educ. VAC 1/4/10 Ongoing 2. Formulate monitoring procedures. Nephrologist Surgeon NDM ADM Clin. Educ. VAC 1/4/10 Ongoing 3. Create standard criteria. QI Team Primary RN Ongoing Ongoing 4. Primary RNs to document vascular access plan of care in every patient integrating facility, nephrologist, and surgeon. VAC monthly progress notes. NETWORK 17 CQI ACTION PLAN – CHANGE CONCEPT # 10 – Education for Care Givers and Patients FACILITY: CONTACT: GOAL: 1. Improve vascular access outcomes as a result of increased staff, patient and family knowledge on caring for access. PROBLEM STATEMENT: 1. Poor vascular access outcome due to lack of caregiver/patient knowledge on caring for access. ROOT CAUSE(S): 1. Limited pre-ESRD education 2. Limited patient education program in CKD clinic and/or dialysis facility. 3. Limited resources for patients and caregivers. ACTION PLAN 1. In-service facility staff regularly on vascular access and patient talking points. 2. Provide education to all caregivers pre-dialysis and after HD start, integrating the nephrologist and surgeon into education sessions. 3. Educate patients to improve the quality of their vascular access outcome through knowledge of prepping sites, applying pressure at sites, use of clamps, assisting staff to select sites, etc. RESPONSIBLE TEAM MEMBER START DATE ESTIMATED COMPLETION DATE ACTUAL COMPLETION DATE TEAM MEMBERS: Medical Director / Nephrologist Surgeon NDM ADM Clinical Educator PI Representatives Vascular Access Coordinator (VAC) Primary Nurses Facility Nurses Patient Care Technicians Dietitian Social Worker CKD Clinic Nurses/MA COMMENTS (STATUS, OUTCOMES, DISPOSITION, ETC.) Clin. Educ. PI Reps. Social Worker 2/15/10 Ongoing 1. Schedule monthly in-services for staff. Nephrologist Surgeon Clin. Educ. PI Reps. Social worker Dietitian 2/15/10 Ongoing 2. Schedule meetings with patients and caregivers before and after initial HD treatments. Nephrologist Clin. Educ. PI Reps. Social Worker Patient Care Technicians 2/15/10 Ongoing 3. Schedule regular educational opportunities to patients regarding vascular access. NETWORK 17 CQI ACTION PLAN – CHANGE CONCEPT # 11 – Outcomes Feedback to Guide Practice FACILITY: CONTACT: GOAL: 1. Implement the review of data monthly or quarterly in QI and staff meetings. PROBLEM STATEMENT: 1. Facility outcomes not used to guide future practice with vascular access. ROOT CAUSE(S): 1. Lack of structure to review outcomes and make system changes. 2. Lack of system to collect vascular access data. 3. Limited analysis of data collected. ESTIMATED RESPONSIBLE START ACTION PLAN COMPLETION TEAM MEMBER DATE DATE 1. Review quarterly vascular access data received from network and report at CQI meetings. 2. Collect and review surgeon vascular access placements, quality and quantity, and report at CQI meetings. 3. Report data at staff meetings routinely. 4. From analysis of data in CQI, document next steps to making changes in facility. Nephrologist NDM ADM PI Reps. VAC Nephrologist VAC PI Reps. NDM/ADM VAC/PI Reps. NDM ADM VAC PI Reps. Ongoing Ongoing Ongoing Ongoing 1/27/10 Ongoing 3/1/10 Ongoing TEAM MEMBERS: Medical Director / Nephrologist Surgeon NDM ADM Clinical Educator PI Representatives Vascular Access Coordinator (VAC) Primary Nurses ACTUAL COMPLETION DATE COMMENTS (STATUS, OUTCOMES, DISPOSITION, ETC.)