NEW PATIENT HEALTH QUESTIONNAIRE
advertisement

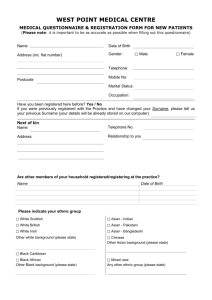
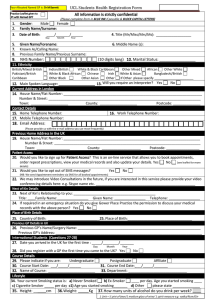
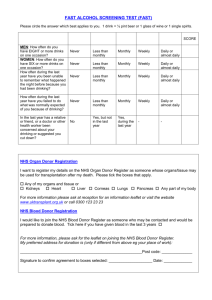
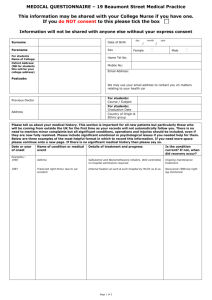
NEW PATIENT HEALTH QUESTIONNAIRE Surname: …………………………………………… First Names: …………………..………………………………………… Address: …………………………………………………………………………………………………………………………………………. Postcode: …………………………………………… Tel. No.: …………………………………………………………..……… Mobile No.: ………………………………………… Date of Birth: …………………………..………… Height: ……………….………. Weight: ……………….…………… Waist Measurement: …………….…..……….. Occupation: …………………………………..…………….………….. Please state your ethnic origin: Date of Entry Into Country (if applicable): ………………….………………. First Language: ………………….…………………. White British Irish Any other white background Mixed White and Black Caribbean White and Black African Any other mixed background Asian or Asian British Indian Pakistani Bangladeshi Any other Asian background Black or British Black Caribbean African Any other black b/ground Other Chinese Any other ethnic group Smoking History (have you ever smoked, if so how much, if stopped when) ……………………………………………………………………………………………………………………………… Operations or Serious Illnesses …………………………………………………………………………………………………. Family History of Diseases: (especially – Heart Disease, Blood Pressure, Chest Disease, Eye Problems and Diabetes): …………………………………………………………………………………..……………………………………………........ Are you on any regular medication from your last doctor or bought over the counter by yourself? If so, what? ......................................................................................................................... Any Known Allergies: ……………………………………………………………….………………………………………. Do you exercise regularly? …………………………. Are you a carer? YES / NO Immunisations (for children only) – Please attach a copy of immunisations to date. SMOKER? NON SMOKER? Please help us to bring your records up to date and complete the following: If you are certain of the smoking status of other family members [age 14-90] please complete a separate form for them. Name: …………………………………………… Date of Birth: ……………………………….… NON SMOKERS Never smoked Ex trivial < 1/day Ex light < 10/day Ex moderate 10-20/day Ex heavy 20-39/day Ex very heavy >40/day [ [ [ [ [ [ ] ] ] ] ] ] [ [ [ [ [ [ [ ] ] ] ] ] SMOKERS Trivial <1/day Light 1-10/day Moderate 10-20/day Heavy 20-39/day Very Heavy >40/day Pipe smoker - number/day Roll ups - ounces/day ] ] PLEASE RETURN TO RECEPTIONIST Tear off if desired If you would like help trying to give up, please contact the Stop Smoking Service on 0845 602 3608 or speak to one of our nursing staff. New Patient Alcohol Questionnaire Name: _______________________________________ DOB: ______________ QUESTION 1.Women: How often do you have 6 or more alcoholic drinks on the same occasion? Men: How often do you have 8 or more alcoholic drinks on the same occasion? 2. In the last year, how often have you been unable to remember what happened when you were drinking the night before? 3. In the last year, how often have you failed to do what was expected of you due to drinking? 4. Has any one ever expressed concern about your drinking or advised you to cut down? SCORE 0 1 2 3 4 Never Less than monthly Monthly Weekly Daily or almost daily Never Less than monthly Less than monthly Monthly Weekly Monthly Weekly Daily or almost daily Daily or almost daily Yes, during the last year Never No Yes, but not in the last year Your Score If you scored 3 or more, please answer the following questions: Question 5. How often do you have a drink that contains alcohol? 6. When you are drinking, on average how many standard alcoholic drinks do you have? 7. In the last year, how often have you found yourself unable to stop drinking once you have started? 8. In the last year, how often have you needed an alcoholic drink to get you going in the morning? 9. In the last year, how often have you experienced guilt or regret after drinking? 10. Have you or someone else ever been injured as a result of your drinking? Total Score 0 1 2 3 4 Never Monthly or less 3-4 2-4 times per month 5-6 2-3 times per week 7-8 4+ times per week 10+ Less than monthly Less than monthly Less than monthly Monthly Weekly Monthly Weekly Monthly Weekly Daily, or almost daily Daily, or almost daily Daily, or almost daily Yes, in the last year 1-2 Never Never Never No Yes, but not in the last year Your Score E-MAIL SERVICE FOR PATIENTS An email service is in place to provide better contact access for patients. This is designed to be a non–urgent service. Urgent problems will still need to be dealt with over the telephone. Hopefully, this will reduce the need for telephone calls which will free receptionists’ time and will mean that patients will not need to wait to get through. If you wish to use this service, the email address is: Contacts.chiddingfold@nhs.net Emails will be collected daily and responses will be actioned by the doctors and receptionists. Replies can be made by email if you wish. To access this part of the service, you will need to sign a consent form allowing us to reply to a secure email address. If this is not signed, the reply will be by telephone or letter. Examples of email requests may be: Were my blood results normal? When does a doctor need to see me for a review? Was my X ray normal? Has my referral letter been sent? Have you had the letter from outpatients clinic yet? Are the results through from the hospital? Please DO NOT email requests for appointments or ask for specific symptom advice. Prescription requests are available through our website: www.chiddsurg.co.uk ……………………………………………………………………………………………………………………………. CONSENT FOR CHIDDINGFOLD SURGERY TO USE A SECURE E-MAIL ADDRESS I …………………………………………….consent to the staff of Chiddingfold Surgery being able to use the Email address below to contact me. I have informed them that this is a secure Email address. E mail address: ……………………………………………………………………………………….I am aware that this email address will be entered onto my medical records but will not be passed to any other person or persons and will not be used for any other purpose than the above. Signed: …………………………………………………. Date: …………………………………….. Witness: ……………………………………………….. Date: ..………………………………… This practice has joined the national Summary Care Record programme which enables each patient to have a summary of their key medical information held securely on the NHS central database, known as the NHS Spine. This summary record could be used in an emergency if you needed treatment when access to the medical record held by your GP was not available; for example if you call the doctor out of hours. You will always be asked to give permission for this record to be viewed and you have the right to decline. Please indicate below whether you would like to have your own Summary Care record by indicating your decision below. A full explanation of each choice follows. 1. 2. 3. 1. My decision I wish to have a Summary Care record containing my medications, allergies and adverse reactions or sensitivities to medications I wish to have a Summary Care record with the above plus additional important medical information held on my record I do not wish to have a Summary Care record Tick ONE A Summary Care record will be created for you from your the details held on our GP clinical system and will contain: a. any record we have of your current repeat medication, any acute medication (one-offs e.g. antibiotics) and any recently discontinued medication b. any record we have of adverse reactions to medication c. any record we have of your allergies 2. A Summary Care Record will be created for you containing the details itemised above in 1, PLUS important additional information you and your GP agree would be useful. (e.g. Diagnoses Asthma, Diabetes etc.; Pacemaker, End of life care etc.) Please discuss this with your GP at your next visit. 3. A note will be made in your records that you do not wish to have a Summary Care Record. Please note that if you attend A&E or if you need emergency treatment when the GP Practice is closed the clinicians treating you may not have access to key information to help them give you the most appropriate treatment. Surname First names Signature Date of birth Today’s date Hand this form to reception at your GP Practice. For further information contact the Summary Care Record Information Line: 0300 123 3020