Supplementary Information (doc 2119K)
advertisement
")
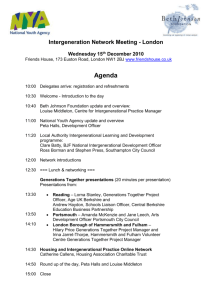
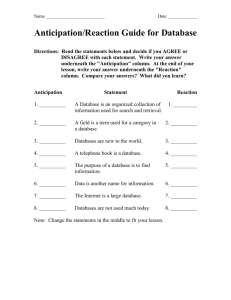
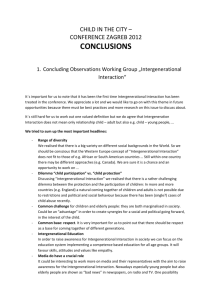
Supplementary information for Parental age effects, but no evidence for an intrauterine effect in the transmission of myotonic dystrophy type 1 Fernando Morales1,2,3, Melissa Vásquez1,3, Patricia Cuenca1,2,3, Domingo Campos4, Carolina Santamaría1,5, Gerardo del Valle6, Roberto Brian7, Mauricio Sittenfeld8 and Darren G. Monckton9 1 Instituto de Investigaciones en Salud (INISA), 2Escuela de Medicina, 3Centro de Investigaciones en Neurociencias, 4Instituto de Investigaciones Psicológicas (IIP), 5Escuela de Nutrición, Universidad de Costa Rica, San José, Costa Rica 6 Laboratorio de Neurofisiología (Neurolab), Curridabat, San José, Costa Rica 7 Servicio de Neurología, Hospital Nacional de Niños, Costa Rica 8 Servicio de Neurología, Hospital San Juan de Dios, Costa Rica 9 Institute of Molecular, Cell and Systems Biology, College of Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow G12 8QQ, UK Corresponding author: Dr. Fernando Morales Cuidad Universitaria Rodrigo Facio Instituto de Investigaciones en Salud Universidad de Costa Rica San Pedro de Montes de Oca San Jose, Costa Rica Tel: +506 2511 3289 E-mail: fernando.moralesmontero@ucr.ac.cr Running title: Intergenerational dynamics in DM1 Morales et al., Intergenerational dynamics in DM1 Supplementary information Page 1 Genealogical studies in Costa Rican DM1 families In order to understand the broad sex-dependent nature of disease transmission and age at onset in DM1, we undertook a genealogical analysis of 41 three generation Costa Rican pedigrees. As expected,1 we observed high levels of anticipation with generation one typically presenting with mild late onset symptoms; generation two usually presenting with the classic adult onset form of the disease; and generation three generally presenting with either juvenile or congenital DM1. Unexpectedly, we observed overall more affected males carrying the DM1 mutation than females (137 males versus 105 females, X2 = 4.23, p = 0.040, Supplementary Figure S1a). Breaking this down further, this appeared to be mostly attributable to an excess of males in generation one: 35 affected males and 14 affected females (X2 = 9.00, p = 0.003). No deviation was observed in generation two (67 affected males, 70 affected females, X2 = 0.07, p = 0.791); but, although not significant an excess of males was also observed in generation three (35 affected males and 21 affected females, X2 = 3.5, p = 0.061). After correction for multiple testing,2 the overall deviation did not remain significant, but the male excess observed in generation one remained significant at the p < 0.04 level. These data are consistent with the previously observed excess of transmitting grandfathers in classic three generation DM1 families.3-9 Some previous investigations have reported apparent preferential transmission of the mutant DM1 allele from DM1 carriers10,11 and apparent preferential transmission of the longer allele from unaffected heterozygous parents in the general population.12,13 In the Costa Rican pedigrees, we found no evidence overall for preferential transmission with the mutant allele inherited by 179 of 367 offspring (48.8%, X2 = 0.22, p = 0.639, Supplementary Figure S1B). However, when we split the data between generations and sex of the transmitting parent, we noted that males in generation two appeared to under-transmit the DM1 mutation to their offspring; 9 offspring inherited the mutation versus 35 who did not (20.5%, X2 = 15.36, p < 0.0001). No such under-transmission was observed in generation one to generation two; males transmitted the DM1 mutation to 96 offspring versus 77 offspring who did not inherit the DM1 mutation (X2 = 2.09, p = 0.148). Likewise, when we combined the male transmission data from generations one and two, no significant deviation from the expected 50:50 ratio was observed (48.4:51.6%, X2 = 0.23, p = 0.632). In the case of female parents, they transmitted the DM1 mutation following the expected pattern irrespective of if they were situated in the first generation (44.6:55.4%, X2 = 0.75, p = 0.387) or the second generation (52.9:47.1%, X2 = 0.29, p = 0.590) (Supplementary Figure 1b). The apparent undertransmission of the DM1 mutation from males in generation two remains significant at the p < 0.002 even after correction for multiple testing. However, it should be noted that of the 35 apparently unaffected offspring only 11 have been confirmed as negative using molecular testing. Of the other 24 individuals, 19 remain below the age of onset of the affected parent and may still develop the symptoms at a later date. Reflecting the previously observed bias,14,15 all 16 of the congenitally affected children in the Costa Rican families were born to affected mothers in generation two. Also consistent with previous observations,3-9 where it could be determined, the transmitting grandparent was more often than not a male (9/12, 75%). In the thirteen pedigrees with at least one congenitally affected child born to an affected mother, there were three families with two congenital cases and 10 families with one case. In theses families there were six pairs of transmitting sisters with at least one sister transmitting CDM. In three of these cases, both sisters transmitted CDM, whereas in the other three families only one sister transmitted CDM and the other sister transmitted a less severe form of the disease. Nonetheless, even in the cases where the sister did not transmit CDM, all the children were affected with the juvenile form of the disease. These families are too small to determine if the previously reported4 familial predisposition for transmitting CDM could be detected. Morales et al., Intergenerational dynamics in DM1 Supplementary information Page 2 Intergenerational expansions and anticipation – atypical cases As described in the main text, clinical anticipation was observed in most maternal transmissions (~85%, (n = 44/52, CI = 0.72 - 0.92) (Figure 2a), and was accompanied by intergenerational expansion in the vast majority of these (~95% (n = 42/44, CI = 0.85 – 0.99). In one maternal transmission striking anticipation (32 years), was associated with an apparent small decrease in repeat length (449 to 421 repeats). Both patients displayed a high degree of somatic mosaicism and somatic mosaicism possibly masked a repeat expansion. However, any intergenerational repeat expansion is likely to be relatively small and would not obviously account for the prominent anticipation. Similarly, in the other case a convincing intergenerational contraction (395 to 229) was still nonetheless accompanied by a 20 year decrease in the age at onset. Of the eight cases in which clinical anticipation was not observed, in four pairs an intergenerational expansion was observed, but both mother and offspring remain asymptomatic. In three cases, the child inherited an expansion and remains currently asymptomatic, but below the age at which the mother developed symptoms. In only one case was an apparent intergenerational expansion accompanied by apparent reverse anticipation (9 years). However, in this case the intergenerational expansion was very small (+6 repeats). Clinical anticipation was also observed in most paternal transmissions (~87% (n = 47/54, CI = 0.76 – 0.94)) (Figure 2a), and was accompanied by intergenerational expansion in the vast majority of these (~96% (n = 45/47, CI = 0.86 – 0.99)). In one paternal transmission a fairly large degree of anticipation (15 years), was associated with an apparent small decrease in repeat length (541 to 536 repeats). Both patients displayed a high degree of somatic mosaicism and it is likely that somatic mosaicism has masked a repeat expansion. In the other case demonstrating apparent anticipation, the intergenerational length change appeared as a convincing contraction of ~92 repeats from 352 to 260 repeats. However, the degree of anticipation observed was relatively modest (4 years) and probably within the bounds of reliability for determining age at onset. Of the seven cases in which clinical anticipation was not observed, in two pairs an intergenerational expansion was observed, but both father and offspring remain asymptomatic. In two cases, the child inherited an expansion and remains currently asymptomatic, but below the age at which the father developed symptoms. In one case, the child inherited a convincing contraction of 77 repeats from 175 to 98 repeats accompanied by apparent reverse anticipation (the child remains asymptomatic, but is now 6 years older than the age at onset of the father). In a similar case of convincing contraction, the child remains asymptomatic but is still 4 years younger than the father’s age at onset. In only one case was an intergenerational expansion accompanied by apparent reverse anticipation (the child remains asymptomatic, but is 8 years older than the father at age at onset). However, in this case the intergenerational expansion was relatively modest (+40 repeats). Morales et al., Intergenerational dynamics in DM1 Supplementary information Page 3 Estimated risk for the transmission of juvenile/CDM from an affected mother In addition to the ROC analysis (main text, Supplementary Figure S4) we also performed logistic regression using maternal ePAL and age at conception as predictive variables and CDM as the dependent variable. The model revealed a determination coefficient of Nagelkerke r2 = 0.39 (p < 0.001) and a predictive capacity of 79%. The Hosmer-Lemeshow test revealed the model was well calibrated with no significant difference between the observed and expected event rates (X2 = 4.77, d.f. = 8, p = 0.782). The maternal ePAL was the main risk factor for CDM (odds ratio = 1.009 (p < 0.001, I.C. 95%, 1.004 – 1.014), but a significant role for age at conception was not detected (odds ratio = 1.057 (p = 0.396, CI = 0.930 - 1.201)). Under this model, a one repeat increase in maternal ePAL increases the odds of transmitting CDM by 1.009 times. Morales et al., Intergenerational dynamics in DM1 Supplementary information Page 4 Supplementary Figure S1. Sex-dependent incidence and transmission of the disease in Costa Rican myotonic dystrophy type 1 pedigrees. (a) Relative sex-dependent incidence of clinically confirmed disease in Costa Rican myotonic dystrophy type 1 pedigrees. The actual numbers of observations are presented within the symbols and the relative percentages below the symbols (males are depicted as squares and females as circles). The statistical significance of any sexdependent difference in relative ratio of male to female patients was determined using a X2-analysis under the null hypothesis of 1:1 incidence. Data are presented for all patients and for cohorts assigned to each of the three generations. (b) Relative sex-dependent transmission of clinically confirmed disease in Costa Rican myotonic dystrophy type 1 pedigrees. The actual numbers of observations are presented within the symbols and the relative percentages below the symbols (males are depicted as squares, females as circles, and parents/offspring of either sex as diamonds). The statistical significance of any sex-dependent difference in the relative ratio of affected to unaffected offspring was determined using a X2 analysis under the null hypothesis of 1:1 transmission. Data are presented for all transmissions and for transmissions from generation one to generation two, and from generation two to generation three. Morales et al., Intergenerational dynamics in DM1 Supplementary information Page 5 Supplementary Figure S2. The intergenerational length change is dependent on the sex of the parent and correlated with the parent’s progenitor allele length. The scatter plots shows the relationship between parental ePAL and the intergenerational length change for female transmissions (circles) and male transmission (squares). Cases with congenital onset in the child are shaded black and cases with juvenile onset in the child are shaded grey. The faint dotted line shows the zero length change line (i.e. points above the line are expansions, and points below are contractions). The line of best fit under linear regression (dotted line female transmission, solid line male transmissions) and relevant statistics are shown. Data are split according to sex of parent (females top, males bottom). Left panels show data over the whole range, whilst the right panels show the data split according to parental ePAL (males </> 80 repeats, females </> 250 repeats). Morales et al., Intergenerational dynamics in DM1 Supplementary information Page 6 Supplementary Figure S3. The degree of anticipation is inversely correlated with the parental age at onset. The scatter plots shows the relationship between the degree of anticipation and the age at onset of the parents symptoms for female transmissions (circles) and male transmission (squares). Cases with congenital onset in the child are shaded black and cases with juvenile onset in the child are shaded grey. The faint dotted line shows the zero change in age at onset (i.e. points below the line demonstrate anticipation). The line of best fit under linear regression (dotted line female transmission, solid line male transmissions) and relevant statistics are shown. Morales et al., Intergenerational dynamics in DM1 Supplementary information Page 7 predicting congenital DM1 predicting congenital/juvenile DM1 1.0 0.9 0.8 0.7 0.6 using maternal ePAL 164 CTG repeats 153 CTG repeats 0.5 0.4 0.3 0.2 sensitivity 0.1 0.0 1.0 0.9 0.8 284 CTG repeats 0.7 284 CTG repeats 0.6 using maternal modal allele length 0.5 0.4 0.3 0.2 0.1 0.0 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 false positive rate (1 - specificity) Supplementary Figure S4. Receiver operating characteristics (ROC) curve analysis for predicting the risk of congenital and/or juvenile DM1 from the affected mothers ePAL or modal allele length. For predicting the risk of congenital DM1 from affected mothers using the mothers ePAL the area under the ROC curve was 0.844 (CI = 0.73 – 0.96, n = 52) and the cut-off value which corresponds to the highest sensitivity and specificity was at 164 repeats. For predicting the risk of congenital DM1 from affected mothers using the mothers modal allele length the area under the ROC curve was ~83% (CI = 0.71 – 0.96, n = 52), and the cut-off value which corresponds to the highest sensitivity and specificity was at 284 repeats. For predicting the risk of juvenile or congenital DM1 from affected mothers using the mothers ePAL the area under the ROC curve was ~85% (CI = 0.74 – 0.96, n = 50) and the cut-off value which corresponds to the highest sensitivity and specificity was at 153 repeats. For predicting the risk of juvenile or congenital DM1 from affected mothers using the mothers modal allele length the area under the ROC curve was ~83% (CI = 0.71 – 0.95, n = 50), and the cut-off value which corresponds to the highest sensitivity and specificity was also at 284 repeats. Morales et al., Intergenerational dynamics in DM1 Supplementary information Page 8 Supplementary References 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Höweler CJ, Busch HFM, Geraedts JPM, Niermeijer MF, Staal A: Anticipation in myotonic dystrophy: fact or fiction? Brain 1989; 112: 779-797. Rice WR: Analyzing tables of statistical tests. Evolution 1989; 43: 223–225. Lopez de Munain A, Cobo AM, Poza JJ et al: Influence of the sex of the transmitting grandparent in congenital myotonic dystrophy. J Med Genet 1995; 32: 689-691. Lavedan C, Hofmann-Radvanyi H, Shelbourne P et al: Myotonic dystrophy: size- and sexdependent dynamics of CTG meiotic instability, and somatic mosaicism. Am J Hum Genet 1993; 52: 875-883. Brunner HG, Bruggenwirth HT, Nillesen W et al: Influence of sex of the transmitting parent as well as of parental allele size on the CTG expansion in myotonic dystrophy (DM). Am J Hum Genet 1993; 53: 1016-1023. Harley HG, Rundle SA, MacMillan JC et al: Size of the unstable CTG repeat sequence in relation to phenotype and parental transmission in myotonic dystrophy. Am J Hum Genet 1993; 52: 1164-1174. Ashizawa T, Dunne PW, Ward PA, Seltzer WK, Richards CS: Effects of sex of myotonic dystrophy patients on the unstable triplet repeat in their affected offspring. Neurology 1994; 44: 120-122. Barceló JM, Mahadevan MS, Tsilfidis C, Mackenzie AE, Korneluk RG: Intergenerational stability of the myotonic dystrophy protomutation. Hum Mol Genet 1993; 2: 705-709. Barceló JM, Pluscauskas M, MacKenzie AE, Tsilfidis C, Narang M, Korneluk RG: Additive influence of maternal and offspring DM-kinase gene CTG repeat lengths in the genesis of congenital myotonic dystrophy. Am J Hum Genet 1994; 54: 1124-1125. Gennarelli M, Dallapiccola B, Baiget M, Martorell L, Novelli G: Meiotic drive at the myotonic dystrophy locus. J Med Genet 1994; 31: 980. Zatz M, Cerqueira A, Vainzof M, Passos-Bueno MR: Segregation distortion of the CTG repeats at the myotonic dystrophy (DM) locus: new data from Brazilian DM families. J Med Genet 1997; 34: 790-791. Carey N, Johnson K, Nokelainen P et al: Meiotic drive at the myotonic dystrophy locus? Nat Genet 1994; 6: 117-118. Chakraborty R, Stivers DN, Deka R, Yu LM, Shriver MD, Ferrell RE: Segregation distortion of the CTG repeats at the myotonic dystrophy locus. Am J Hum Genet 1996; 59: 109-118. Vanier TM: Dystrophia myotonica in childhood. BMJ 1960; 2: 1284-1288. Harper PS, Dyken PR: Early-onset dystrophia myotonica. Evidence supporting a maternal environmental factor. Lancet 1972; 2: 53-55. Morales et al., Intergenerational dynamics in DM1 Supplementary information Page 9