Supplementary Information (doc 623K)
advertisement
")
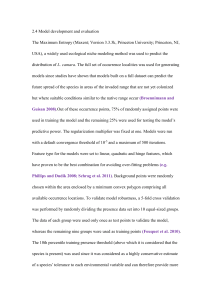
Supplementary Material: Clinical utility and implications of asparaginase antibodies in acute lymphoblastic leukemia Chengcheng Liu,1,5 Jitesh D. Kawedia, PhD1 Cheng Cheng, PhD2 Deqing Pei, 2 Christian A. Fernandez, PhD1 Xiangjun Cai, PhD1 Kristine R. Crews, PharmD1 Sue C. Kaste, DO3,5 John C. Panetta, PhD1 W. Paul Bowman, MD6 Sima Jeha, MD4 John T. Sandlund, MD4 William E. Evans, PharmD1 Ching-Hon Pui, MD4 and Mary V. Relling, PharmD1 From Departments of 1Pharmaceutical Sciences, 2Biostatistics, 3Radiological Sciences, and 4 Oncology, St Jude Children’s Research Hospital, Memphis, TN; 5University of Tennessee Health Science Center, Memphis, TN; and 6Cook Children’s Hospital, Fort Worth, TX. Correspondence: Mary V. Relling, St. Jude Children’s Research Hospital, 262 Danny Thomas Place, Memphis, TN 38105-2794, USA. Phone: 901-595-2348; Fax: 901-595-8869; e-mail: mary.relling@stjude.org 1 SUPPLEMENT Supplemental Methods Supplemental Tables Table S1. Clinical features of patients with and without samples evaluable for antiasparaginase antibodies. Table S2. Number of available blood samples at each time point. Table S3. Number of patients having allergic reaction to Elspar in different phases. Table S4. Clinical features and allergic reactions to Elspar. Table S5. Clinical features and anti-Elspar antibody status. Supplemental Figures Figure S1. Total XV asparaginase regimen and anti-asparaginase antibody measurements. Figure S2. Anti-Elspar antibody level relative to the time of clinical reaction to Elspar. Figure S3. ROC curves of the antibody tests. Figure S4. Association between Week 7 anti-Elspar antibody level and the proportion of patients reacted to Elspar around week 7. Figure S5. The frequency of hypersensitivity to Oncaspar and Erwinase. Supplemental References 2 Supplemental methods Anti-asparaginase antibodies A total of 2010 serum samples for antibodies to three forms of asparaginase (Elspar, Erwinase, and Oncaspar) were measured by ELISA. Of these, 471 samples were assayed at the University of Tennessee Health Science Center (UTHSC) and 1345 samples were assayed at St. Jude Children’s Research Hospital (SJCRH). The positive control reference pool was prepared from patients known to have received the specific form of asparaginase and who exhibited clinical signs of allergic reaction and had high titers of antibodies, represented by high optical density (OD) readings. The negative control reference pool was prepared from healthy volunteers who had never received asparaginase treatment. A sample assayed at SJCRH was considered positive if the natural log of its 1:400 OD reading was greater than 2.58 standard deviations above the negative control process mean. A sample assayed at UTHSC was considered positive if the natural log of its 1:3200 OD reading was greater than 2 standard deviations above the negative control process mean. Samples that were not positive were considered negative. Because the magnitudes of the scale of antibody OD readings obtained at the two facilities differed, we normalized the OD readings based on a comparison of 194 serum samples measured for antibody levels at both SJCRH and UTHSC. The normalization of UTHSC OD readings to the same scale was applicable to the SJCRH readings was described by an exponential model using equation 1 (Elspar), 2 (Erwinase), and 3 (Oncaspar) to maintain consistency of OD readings between UTHSC and SJCRH. All of the samples measured at UTHSC had their OD readings normalized to the scale of the readings obtained at SJCRH using the following equations. log (normalized OD) = -5.066 + 3.509 ∙ exp [0.526 × log (original OD)] [1] 3 log (normalized OD) = -4.360 + 3.518 ∙ exp [0.806 × log (original OD)] [2] log (normalized OD) = -5.280 + 3.684 ∙ exp [0.520 × log (original OD)] [3] Estimation of antibody area-under-the-curve (AUC) The area under the antibody-concentration-versus-time curve (AUC) was estimated using the method of trapezoids in the 360 patients who had at least four out of five scheduled antibody results (including week 7 and week 17 tests in the continuation phase and at least two antibody tests in the induction phase). Induction AUC (antibody AUC between day 5 and day 34) and continuation AUC (antibody AUC between week 7 and week 17) were estimated separately using OD readings for each patient’s serum tested against Elspar, the front-line asparaginase preparation (Supplemental Figure 1). Analyses were performed using the sum of the induction AUC and continuation AUC of antibodies to Elspar asparaginase. Asparaginase activity This assay was similar to a previously reported assay,1 with a faster and more controlled process as well as improved linearity range without sample pretreatments. The asparaginase activity in serum was measured by an enzymatically coupled oxidation of reduced nicotinamide adenine dinucleotide (NADH): L-Asparagine Asparaginase L-Aspartate + NH4 Glutamic oxalacetic transaminase L-Aspartate + α-Ketoglutarate Oxaloacetate + L-Glutamate 4 Oxaloacetate + NADH Malic dehydrogenase Malate + NAD+ When monitored by spectrophotometry, the oxidation of NADH leads to a corresponding decrease in absorbance at 340 nM. The rate of change of absorbance is directly proportional to asparaginase activity. The enzyme reaction mixture was prepared by combining 200 mL of 10x Tris-buffered saline, 400 mL of glycerol, 200 mg of α-ketoglutaric acid, 264 mg of asparagine, 200 mg of β-NADH, 400 µL of glutamic oxaloacetic transaminase, 200 µL of malic dehydrogenase, and 1400 mL distilled and deionized water, and stored at -80ºC. (All the reagents above were from SigmaAldrich, St. Louis, MO.) Before plate reading, the enzyme reaction mixture was incubated in a 37ºC water bath for 30 min. Then patient sera were added to 96-well UV-transparent plates (Corning. Inc, NY) in quadruplicate. The reaction was started by adding 190 µL of enzyme reaction mixture to each well. The enzyme reaction mixture was added one row at a time, with a 20 second interval between each addition. The plate was read using a BioTek ELx808IU Microplate Reader (BioTek, Winooski, VT) at 340 nm with a 20 second interval for 15 min. The activity was estimated by the slope of the change of optical density over time. The linearity range of this assay was 0.011-2.2 U/mL. Samples higher than 2.2 U/mL were diluted with sample dilution buffer (5% bovine serum albumin in deionized water). Calibrators were established with asparaginase standard solutions: 0.025-2.0 U/mL native E. coli asparaginase (BioVendor Laboratory Medicine. Inc, Czech Republic) in sample dilution buffer. Receiver-operator-characteristic (ROC) curves 5 The ROC curves of antibody tests were generated by plotting the true positive rate (sensitivity) and corresponding false positive rate (1-specificity) for every possible threshold OD value (to separate positive from negative samples; supplemental Figure 3). The area-under-the-curve (AUC) of the ROC curve is a relative measure of the diagnostic accuracy of a test. An AUC of 1.0 would indicate a perfect test (100% TP, 0% FP, 100% TN, 0% FN), whereas 0.5 would indicate a random classification. A value greater 0.9 represents a rather high accuracy, a value less than 0.7 represents a low accuracy, and a value in between would be considered fair to good.2 (TP, true positive; FP, false positive; TN, true negative; FN, false negative.) 6 Supplemental Tables. Table S1. Clinical features of patients with (n = 410) and without (n = 88) samples evaluable for anti-asparaginase antibodies. Patients with samples Patients without samples n (%) n (%) Less than 10 years 302 (81.2) 70 (18.8) Older than 10 years 108 (85.7) 18 (14.3) Male 228 (81.7) 51 (18.3) Female 182 (83.1) 37 (16.9) White 282 (88.4) 37 (11.6) Black 65 (91.5) 6 (8.5) Other 63 (58.3) 45 (41.7) B-lineage 345 (81.6) 78 (18.4) T-lineage 65 (86.7) 10 (13.3) Low-risk 197 (82.4) 42 (17.6) Standard/high-risk 213 (82.2) 46 (17.8) P Age 0.28 Sex 0.72 Racea 0.0001 Immunophenotypeb 0.33 Treatment arm 1.0 a = Genetically determined race as described;3 b = acute lymphoblastic leukemia immunophenotype. 7 Table S2. Number of patients with evaluable blood samples at each time point. Number of patients Time point of antibody test (samples) Day 5 401 (420) Day 19 392 (396) Day 34 384 (399) Week 7 381 (408) Week 17 367 (387) 8 Table S3. Number of patients having allergic reaction to Elspar at each phase of therapy. Phase Low-risk Standard/high-risk Total Induction 2 3 5 Continuation weeks 1-6 0 54 54 Reinduction I 96 1 97 Continuation weeks 10-16 0 7 7 Reinduction II 2 0 2 Reintensification 0 4 4 Total 100 69 169 9 Table S4. Clinical features and allergic reactions to Elspar (n=410*) All patients Allergy Low-risk Arm No allergy n Allergy P n(%) No allergy n n(%) Standard/high-risk Arm P n(%) n(%) 183 94 (51.4) 89 (48.6) 14 6 (42.9) 8 (57.1) 93 53 (57.0) 40 (43.0) Allergy No allergy n(%) n(%) 119 35 (29.4) 84 (70.6) 94 34 (36.2) 60 (63.8) 135 43 (31.9) 92 (68.1) 78 26 (33.3) 52 (66.7) 136 53 (39.0) 83 (61.0) n P Age Less than 10 years 302 129 (42.7) 173 (57.3) 0.36 0.59 Older than 10 years 108 40 (37.0) 68 (63.0) Male 228 96 (42.1) 132 (57.9) Female 182 73 (40.1) 109 (59.9) 104 47 (45.2) 57 (54.8) White 282 128 (45.4) 154 (54.6) 0.037 146 75 (51.4) 71 (48.6) Black 65 20 (30.8) 45 (69.2) 24 15 (62.5) 9 (37.5) 41 5 (12.2) 36 (87.8) Other 63 21 (33.3) 42 (66.7) 27 10 (37.0) 17 (63.0) 36 11 (30.6) 25 (69.4) B-lineage 345 157 (45.5) 188 (54.5) .0001 197 100 (50.8) 97 (49.2) 148 57 (39.2) 91 (60.8) T-lineage 65 12 (18.5) 65 12 (18.5) 53 (81.5) 0.31 Sex 0.69 0.12 0.88 Racea 0.19 0.004 Immunophenotypeb 53 (81.5) 0 0 (0.0) 0 (0.0) NA 0.003 a = Genetically determined race as described;3 b = acute lymphoblastic leukemia immunophenotype; NA = not applicable. *Patients with serum samples evaluable for anti-asparaginase antibodies (n = 410). Analysis for all patients (n = 498) has been previously reported.4 10 Table S5. Clinical features and anti-Elspar antibody status (n=410) All patients Positive Low-risk Negative n Positive P n(%) Negative n n(%) Standard/high-risk P n(%) Positive Negative n(%) n(%) 119 53 (44.5) 66 (55.5) 94 47 (50.0) 47 (50.0) 135 65 (48.2) 70 (51.8) 78 35 (44.9) 43 (55.1) 136 71 (52.2) 65 (47.8) 0.013 n n(%) P Age Less than 10 years 302 182 (60.3) 120 (39.7) Older than 10 years 108 54 (50.0) 54 (50.0) Male 228 135 (59.2) 93 (40.8) Female 182 101 (55.5) 81 (44.5) White 282 Black Other 0.07 183 129 (70.5) 54 (29.5) 0.14 0.49 14 7 (50.0) 7 (50.0) 93 70 (75.3) 23 (24.7) 104 66 (63.5) 38 (36.5) 175 (62.1) 107 (37.9) 0.005 146 104 (71.2) 42 (28.8) 65 36 (55.4) 29 (44.6) 24 16 (66.7) 8 (33.3) 41 20 (48.8) 21 (51.2) 63 25 (39.7) 38 (60.3) 27 16 (59.3) 11 (40.7) 36 9 (25.0) 27 (75.0) B-lineage 345 213 (61.7) 132 (38.3) .0001 197 136 (69.0) 61 (31.0) 148 77 (52.0) 71 (48.0) 0.026 T-lineage 65 23 (35.4) 65 23 (35.4) 42 (64.6) Sex 0.48 0.09 0.67 Racea 0.40 Immunophenotypeb 42 (64.6) 0 0 (0.0) 0 (0.0) NA a = Genetically determined race as described;3 b = acute lymphoblastic leukemia immunophenotype; NA = not applicable. 11 Supplemental figure legends Figure S1. Total XV asparaginase regimen and anti-asparaginase antibody measurements. All patients received Elspar (ASP) at 10000 U/m2 per dose during remission induction; patients on the SHR arm received 25000 U/m2 per week at weeks 1-19; those on the LR arm received 10000 U/m2 thrice weekly at reinduction weeks 7-9 and 17-19. Serum samples for antiasparaginase antibodies (ANTI-ASP) were collected on days 5, 19, and 34 of remission induction and weeks 7 and 17 of continuation therapy. The area under the antibodyconcentration-versus-time curve (ANTI-ASP AUC) was estimated for induction (between day 5 and day 34) and continuation (between week 7 and week 17) using OD readings tested against Elspar. ASP (LR) ASP (SHR) ( ) ( ) 10000 U/m2 10000 U/m2 10000 U/m2 25000 U/m2 4 7 1 Weeks 1 Induction 4 Consolidation 7 1 4 Continuation 7 10 14 (Reinduction I) 17 20 47 (Reinduction II) ANTI-ASP Day 5 ANTI-ASP AUC 19 34 Induction AUC Week 7 Week 17 Continuation AUC 12 Figure S2. Anti-Elspar antibody level relative to the time of clinical reaction to Elspar. Anti-Elspar OD level in patient samples (dots) relative to the number of days elapsed before (negative) or after (positive) between sample collection and clinical reaction to Elspar. The trend lines of median (solid) and quartiles (dashed) are shown. 13 Figure S3. ROC curves of the antibody tests. Receiver operating characteristic (ROC) curves of the antibody tests at day 34, week 7 and week 17, showing the true positive rates and respective false positive rates for predicting or confirming clinical allergic reactions. Each point on the curve corresponds to a specific threshold of anti-Elspar OD that putatively divides antibody-positive from antibody-negative samples. Right y-axis shows the color key that visualizes the mapping from the natural log of anti-Elspar OD to colors. The positive threshold dividing positive from negative samples for logOD is -3.2 (circles). The AUC of the ROC curves, which represents overall test performance on predictions, is shown in each graph. LR, low-risk; SHR, standard/high-risk; Ab, anti-Elspar antibody; Rxn, clinical reaction; AUC, area under the curve. Time of antibody tests: D34 = Day 34 of induction therapy; W7 = Week 7 of continuation therapy; and W17 = Week 17 of continuation therapy. AUC=0.857 False positive rate log(anti-Elspar OD) False positive rate W7 Ab vs. W1-6 Rxn (SHR) W17 Ab vs. W1-16 Rxn (SHR) AUC=0.870 False positive rate True positive rate log(anti-Elspar OD) False positive rate True positive rate True positive rate log(anti-Elspar OD) D34 Ab vs. W1-6 Rxn (SHR) AUC=0.908 log(anti-Elspar OD) False positive rate AUC=0.700 True positive rate True positive rate True positive rate AUC=0.782 W17 Ab vs. W7-9 Rxn (LR) log(anti-Elspar OD) W7 Ab vs. W7-9 Rxn (LR) log(anti-Elspar OD) D34 Ab vs. W7-9 Rxn (LR) AUC=0.867 False positive rate 14 Figure S4. Association between Week 7 anti-Elspar antibody level and the proportion of patients reacting to Elspar around week 7. Left panels: the distribution of patients with (solid bars) and without (open bars) clinical reactions by their anti-Elspar OD at week 7. (a) Patients on the LR arm (n = 195) with and without reactions during weeks 7-9. (c) Patients on the SHR arm (n = 175) with and without reactions during weeks 1-6. Right panels: the positive correlation between week 7 anti-Elspar OD and the proportion of patients having clinical reaction at (b) weeks 7-9 (LR) and (d) weeks 1-6 (SHR). Trend lines are shown. LR, low-risk; SHR, standard/high-risk. 15 Figure S5. The frequency of hypersensitivity to Oncaspar and Erwinase. The proportion of patients exhibiting secondary allergic reactions and antibody positivity among the patients who had samples tested for anti-Oncaspar (n = 85) or anti-Erwinase (n = 63) after they received Oncaspar or Erwinase. Ab, antibody against Oncaspar (left) or Erwinase (right). Erwinase (n=63) Oncaspar (n=85) Ab-negative No reaction 15 (18%) Ab-positive Reaction 20 (23%) Ab-negative Reaction 3 (4%) Ab-positive No reaction 47 (55%) Ab-positive Reaction 4 (6%) Ab-positive No reaction 8 (13%) Ab-negative No reaction 46 (73%) Ab-negative Reaction 5 (8%) 16 References 1. Asselin BL, Whitin JC, Coppola DJ, Rupp IP, Sallan SE, Cohen HJ. Comparative pharmacokinetic studies of three asparaginase preparations. J Clin Oncol 1993; 11: 1780-1786. 2. Swets JA. Measuring the accuracy of diagnostic systems. Science 1988; 240: 1285-1293. 3. Yang JJ, Cheng C, Devidas M, Cao X, Fan Y, Campana D, et al. Ancestry and pharmacogenomics of relapse in acute lymphoblastic leukemia. Nat Genet 2011; 43: 237-241. 4. Chen SH, Pei D, Yang W, Cheng C, Jeha S, Cox NJ, et al. Genetic variations in GRIA1 on chromosome 5q33 related to asparaginase hypersensitivity. Clin Pharmacol Ther 2010; 88: 191196. 17