Notes
advertisement

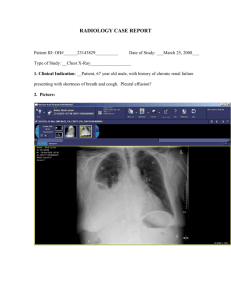
Flail Chest and Pleural Effusion A. Etiology/Pathophysiology of Flail Chest and Pleural Effusion 1. Normal physiology a. Flail Chest 1) Results from multiple rib fractures. 2) Chest wall unstable 3) Diagnosis of flail chest is made on the basis of fracture of two or more ribs, in two or more separate locations, causing an unstable segment. b. Pleural Effusion is a collection of fluid in the pleural space. It is not a disease but rather a sign of serious disease 1) Collection of fluid or air in pleural space 2) Not a disease – sign of serious disease 2. Etiologya. Flail Chest 1) Trauma with impact to fracture ribs b. Pleural effusion is frequently classified as: 1) Transudate occurs primarily in non inflammatory conditions and is an accumulation of protein poor, cell poor fluid 2) Exudates effusion is an accumulation of fluid and cells in an area of inflammation 3) Empyema is a pleural effusion that contains pus. 3. Pathophysiology a. Flail Chest 1) Chest will move paradoxically with respect to the intact portion of the chest 2) Paradoxical movement results in inadequate ventilation and increased work of breathing 3) Underlying lung may have contusions 4) Paradoxical movement and contusions result in increased hypoxemia 5) Apparent on visual examination 6) Shallow rapid respirations and tachycardia 7) Palpation of crepitus near fractured ribs 8) Signs and symptoms of pneumothorax or hemothorax b. Pleural Effusion type depends on the sample of pleural fluid obtained via thoracentesis (a procedure done to remove fluid from the pleural space). The main goal of management of pleural effusions is to treat the underlying cause. 1) Transudative a) Primarily non inflammatory conditions b) Accumulation of protein poor and cell poor fluid c) Increased hydrostatic pressure found in heart failure, most common cause d) Decreased oncotic pressure as result of hypoalbuminemia (found in chronic liver or renal disease) (1) Fluid movement is facilitated out of the capillaries andinto the pleural space 2) Exudative a) Accumulation of fluid and cells in an area of inflammation b) Results from increased capillary permeability – inflammatory reaction c) Secondary to pulmonary malignancies, pulmonary infections, pulmonary embolization and GI disease B. Clinical Manifestations/Complications of Flail Chest and Pleural Effusion 1. Flail Chest a. Dyspnea b. Chest pain on inspiration at site of injury c. Client splints affected area d. Palpable crepitus e. Decreased breath sounds f. Unequal chest expansion g. Shallow breaths to decrease pain h. Atelectasis may develop with decrease ventilation 2. Pleural Effusion a. Dyspnea b. Decreased movement of chest wall on affected side c. Pleurisy d. Dullness on percussion e. Absent or diminished breath sounds over affected area C. Collaborative Care for Flail Chest and Pleural Effusion 1. Diagnostic tests a. Labs 1) Flail Chest a) ABGs 2) Pleural Effusion a) Thoracentesis (1) Excudate has high protein content and generally dark yellow (2) Transudate has low protein and generally clear or pale yellow (3) Empyema contains pus as result of pneumonia, TB, lung abcess and infection b) ABGs b. X-rays 1) Flail Chest a) Chest x-ray 2) Pleural Effusion a) Chest x- ray – if effusion is greater than 250ml b) CT scan 2. Drug Therapy a. Flail Chest initial therapy consists of airway management, adequate ventilation, supplemental oxygen therapy, careful administration of IV solutions and pain control. b. Definitive therapy is to reexpand the lung and ensure adequate oxygenation 1) Opioid used with caution 2) Supplemental oxygen 3) Intercostal nerve block 4) Epidural analgesia 5) Suction 6) Mechanical ventilation c. Pleural Effusion 1) Doxycycline (Vibramycin) 2) Bleomycin (Blenoxane) 3) Talc 4) Antibiotic if infection 3. Diet changes a. Flail Chest and Pleural Effusion 1) As tolerated 4. etc. a. Flail Chest 1) Airway management 2) Adequate ventilation 3) Elevate the head of the bed 4) Chest tube if pneumothorax develops a) The purpose of chest tubes and pleural drainage is to remove the air and fluid from the pleural space and to restore normal intrapleaural pressure so that the lungs can reexpand. b) Chest tube malposition is the most common complication c) Routine monitoring is done by the nurse to evaluate if the chest drainage is successful by observing for tidaling in the water seal chamber, listening for breath sounds over the lung fields, and measuring the amount of fluid drainage. b. Pleural Effusion 1) Treat the underlying cause 2) Pleurodesis 3) Chest tube 4) Therapeutic D. Nursing Assessment Specific for Flail Chest and Pleural Effusion 1. Subjective Data a. Flail Chest 1) Shortness of breath 2) Intercostals pain, even after chest healed b. Pleural Effusion 1) Shortness of breath 2) Pain on inspiration 2. Objective Data a. Flail Chest and Pleural Effusion 1) Vital signs 2) Oxygen saturation 3) Pain E. Pertinent Nursing Problems and Intervention for Flail Chest and Pleural Effusion 1. Nursing Diagnosis a. Ineffective breathing pattern related to pain and position as evidenced by shortness of breath, shallow respirations 1) Demonstrate and effective respiratory rate, rhythm and depth of respirations 2. Health Promotion a. Flail Chest and Pleural Effusion 1) Correct the underlying problem 3. Nursing Interventions a. Flail Chest 1) Decrease pain main goal 2) Promote adequate chest expansion b. Pleural Effusion 1) Decrease pain 2) Promote adequate ventilation 4. Rehabilitation and Home Care a. Flail Chest and Pleural Effusion 1) Correct underlying cause