ADIS DRUG EVALUATION
Drugs 1998 Sep; 56 (3): 429-445
0012-6667/98/0009-0429/$17,00/0
Adis International Limited. All rights reserved.
Domperidone
A Review of its Use in Diabetic Gastropathy
Amitabh Prakash and Antona J. Wagstaff
Adis International Limited, Auckland, New Zealand
Various sections of the manuscript reviewed by:
A.P. Braun, Diabetes Center of New Jersey, Muhlenberg Regional Medical Center, University of Medicine
and Dentistry of New Jersey, Rutgers, New Jersey, USA; U. Bonucceli and P. Del Dotto, Dipartimento di
Neuroscienze Dell'Universita' di Pisa, Pisa, Italy; M. Hongo, Department of Comprehensive Medicine,
Tokohu University School of Medicine, Sendai, Japan; M. Horowitz, Department of Medicine, Royal
Adelaide Hospital, Adelaide, South Australia, Australia; K.L. Koch, Department of Medicine, Section of
Gastroenterology and Hepatology, The Milton S. Hershey Medical Center, Hershey, Pennsylvania, USA; R.A.
Kozarek, Department of Medicine, Section of Gastroenterology, Virginia Mason Medical Center, University
of Washington, Seattle, Washington, USA; P-H. Nilsson, Department of Internal Medicine, Central Hospital,
Växjö, Sweden; D.K, Sommers, Department of Pharmacology, University of Pretoria, Pretoria, South Africa;
M. Velasco, Clinical Pharmacology Unit, Vargas Medical School and Vargas Hospital, Caracas, Venezuela;
J.W. Wiley, Department of Internal Med'cine, Division of Gastroenterology and Gastroenterology Research
Unit, The University of Michigan Medical Center, Ann Arbor, Michigan, USA.
Data Selection
Sources: Medical literature published since 1966 on domperidone, identified using AdisBase (property database of Adis
International, Auckland, New Zealand), Medline and EMBASE. Additional references were identified from the reference lists of published
articles. Bibliographical information, including contributory unpublished data, was also requested from the company developing the drug.
Search strategy: AdisBase search term were 'domperidone', 'gastrokinetics', 'diabetes mellitus', 'diabetic complications' and 'gatroparesis'
Medline and EMBASE search terms were 'domperidone' ‘diabetes’, ‘gastroparesis or stomach-disease’ and ‘domperidone –pharmacodynamic and – pharmacokinetic’. Searches were updated 17 Jul 1998.
Selection: Studies
in patiets with diabetes mellitus with gastropathy who received domperidone. Inclusion of studies was based
mainly on the methods section of the trials. When available, large, well controlled trials with appropriate statistical methodology were preferred.
Relevant pharmacodynamic and pharrnacokinetic data were also included.
Index terms: Domperidone, diabetic complications, gastroparesis, pharmacokinetics, pharmacodynamics, therapeutic use, tolerability, drug
interactions, dosage and administration and quality of life.
Contents
Abstract
..................................................................................................................................... 430
1. Diabetic Gastropathy .................................................................................................................... 431
2. Pharmacodynarnic Properties ....................................................................................................... 432
2.1 Mechanism of Action ................................... . .......................................................................432
2.2 Gastrointestinal Effects ............................................................................................................432
2.2.1 Effects on the Stomach and Duodenum .......................................................................432
2.3 Endocrine Effects .....................................................................................................................434
2.3.1 Plasma Prolactin Levels ....................... ..........................................................................434
2.3.2 Plasma Insulin Levels ........................................... . ......................................................... 434
2.3.3 Effects on Other Hormones ............................................................................................ 434
2.4 Other Effects ............................................................................................................................ 435
3. Pharmacokinetic Properties ........................................................................................................... 435
3.1 Absorption and Distribution ...................................................................................................... 435
430
4.
5.
6.
7.
Prakash & Wagstaff
3.2 Metabolism and Excretion ................................................................................................. .... 435
3.3 Drug Interactions ...................................................................................................................... 436
Clinical Efficacy .............................................................................................................................. 436
4.1 Symptomatic Improvement ................................. .................................................................. 436
4.1.1 Short Term Trials .............................................................................................................. 436
4.1.2 Long Term Trials .............................................................................................................. 439
4.1.3 Trials in Patients with Symptomatic Gastropathy Refractory to Other Agents ............... 439
4.2 Effects on Quality of Life .......................................................................................................... 439
4.3 Other End-points .............................................................................. ...................................... ..440
Tolerability ....................................................................................................................................... 440
Dosage and Administration .......................................................................................................... ...441
Place of Domperidone in the Management of Diabetic Gastropathy ......................................... 441
Abstract
Domperidone is a selective antagonist at peripheral dopamine D2 receptors,
with gastroprokinetic and antiemetic properties. It increases the frequency and
duration of antral and duodenal contractions, thus decreasing/improving transit time
of food through the gastrointestinal tract. Gastric emptying of liquids and solids
is significantly improved with oral domperidone 40 to 120 mg/day in patients
with diabetic gastropathy.
Oral domperidone 40 to 80 mg/day significantly decreased the severity of
symptoms of gastropathy from baselim values in 66 to 88% of patients with type
1 (insulin-dependent) or insulin-requiring diabetets mellitus, Double-blind withdrawal of domperidone from patients who had responded previously led to greater
deterioration of symptoms in patients with delayed gastric emptying than in those
who continued receiving the drug. Quality of life was significantly improved in
patients who showed a symptomatic response to domperidone. The administration of domperidone 40 to 120 mg/day significantly reduced hospitalisation rates
in patients with gastropathy. The symptomatic improvement with domperidone
80 mg/day was similar to that seen with cisapride 40 rng/day or metoclopramide
40 mg/day, and therapeutic benefits seen in symptoms of .gastropathy were maintained with domperidone for up to 12 year:-. Domperidone 40 to 80.mg/day may
be effective in patients who are refractory to metoclopramide, and a combination
of domperidone 80 mg/day with cisapride 80 mg/day may improve some symptoms in patients who do not respond to either agent alone.
Domperidone 40 to 120 mg/day was well tolerated for periods up to 12 years
in trials in patients with diabetic gastropathy. Adverse events with domperidone
80 mg/day were similar to those seen in placebo recipients and significantly fewer
than in patients receiving metoclopramide 40 mg/day. Although significant elevation of plasma prolaclin levels (unrelated to dosage and. duration of treatment)
occurred in all domperidone recipients, prolacUn-related adverse events were
observed in only 10 to 20% of patients.
Conclusions: The available data suggest that domperidone 40 to 80 mg/day
is an effective agent for the management of symptoms of gastropathy in patients
with type 1 diabetes mellitus. In addition, it may provide symptom improvement
in patients with gastropathy refractory to other gastroprokinetic agents.
Domperidone maintains efficacy in the long term (up to 12 years) and appears to
have a better tolerability profile than metoclopramide 40 mg/day.
© Adis International Limited. All rights reserved.
Drugs 1998 Sep; 56 (3)
Doperidone: A Review
1. Diabetic Gastropathy
The term 'gastroparesis diabeticorum' was coined
by Kassander 40 years ago to describe asymptomatic gastric retention in patients with diabetes mellitus; delayed gastric emptying of solids and liquids
may occur in 50% of diabetic patients.[1] Gastric
emptying was studied in 12 patients with type 1
diabetes mellitus and in 22 healthy volunteers.[2]
All the evaluated parameters, including solid lag
phase (57 vs 35 min, p < 0.001), solid retention at
100 min (79 vs 29%, p < 0.001) and liquid 50%
emptying time (50 vs 18 min, p < 0.001), showed
significant impairment of gastric emptying in diabetic patients compared with volunteers.
However, the presence of delayed gastric emptying or gastroparesis has shown poor correlation
with the prevalence of upper gastrointestinal symptoms in patients with diabetes mellitus. A metaanalysis of trials in patients with gastropathy who
had been treated with oral prokinetic agents found
no association between symptomatic improvement
and accelerated gastric emptying.[3] In view of the
fact that many diabetic patients with symptoms of
'gastroparesis' have normal gastric emptying[4] and
that up to 50% of diabetic patients with marked
delay in gastric emptying may have few or no
symptoms,[5] terms such as 'diabetic dyspepsia'[6] or
'diabetic gastropathy' [7,8] have been favoured to
describe the clinical syndrome.
The precise prevalence of symptomatic gastropathy in patients with diabetes mellitus is unknown
but 76% of 136 diabetic patients reported gastrointestinal symptoms on being specifically questioned.[9]
The symptoms of gastropathy in patients with
diabetes mellitus appear to be multifactorial in
origin. The various pathophysiological changes
such as decreased motor activity of the stomach
(fundic or antral activity, phase three interdigestive
motor activity, migrating motor complex or pylorospasm) have been reviewed elsewhere, as have the
underlying pathogenetic mechanisms such as autonomic neuropathy, abnormalities in gut hormone
levels, hyperglycaemia, electrolyte imbalances,
changes in secretion of insulin and glucagon, and
© Adis International Limited. All rights reserved.
431
micro- and macroangiopathy of the stomach.[10,11]
Recent studies have highlighted the importance of
blood glucose levels in the modulation of gastric
electrical and motor activity, as well as in the causation of upper gastrointestinal symptoms in patients with type 1 diabetes mellitus.[12-17] Symptoms of gastropathy include nausea and vomiting,
epigastric burning, early satiety, belching, regurgitation, postprandial fullness, brittle diabetes, malnutrition, weight loss and symptoms related to
erratic drug absorption.[1] Diabetic gastropathy is a
chronic condition and despite glycaemic control
and dietary manipulation, it has been estimated that
80% of patients require long term maintenance therapy with prokinetic and/or antiemetic agents.[18]
Domperidone (fig. 1) is a benzimidazole which
is structurally related to the butyrophenones. Oral
domperidone is effective in the management of
emesis due to a wide variety of causes, including
that induced by anticancer agents. [19] Recently,
domperidone has also been found to be effective in
the treatment of patients with idiopathic dyspepsia. [20-22] Although the prevalence of symptomatic
gastropathy in patients with type 1 (insulin dependent) diabetes mellitus may be similar to that in
patients with type 2 (non-insulin-dependent) diabetes mellitus,[5] almost all published trials involving domperidone have evaluated the efficacy of the
drug in patients with type 1 diabetes mellitus with
symptoms of gastropathy (section 4). The focus of
this review, therefore, will be on the efficacy of
domperidone in the management of patients with
diabetes mellitus and gastropathy.
Drugs 1998 Sep; 56 (3)
432
Prakash & Wagstaff
2. Pharmacodynamic Properties
2..1 Mechanism of Action
The primary mechanism by which domperidone
exerts its pharmacological actions is believed to be
selective antagonism of peripheral dopaminergic
D2 receptors.[23] Other suggested mechanisms include increased acetyicholine release[24] and inhibition of cholinesterase activity[25] Table I provides an overview of studies investigating these
effects.
2.2 Gastrointestinal Effects
A single oral close of domperidone 30mg significantly reduced the mouth to caecum transit time
(from 89 to 63 min, p < 0,01) as measured by a
breath H2 test in 6 healthy volunteers.[31] The effects of oral domperidone on lower oesophageal
sphincter pressure (LOSP) are equivocal and may
be dose-dependent. LOSP was increased, by about
15mm Hg over placebo values, after 40 to 90 minutes in 9 patients receiving a single high dose of
domperidone l00mg[32] A significant (p < 0.01)
increase in LOSP from baseline values was also
reported in healthy volunteers (numbers not stated)
and 47 patients with gastro-oesophageal reflux disease receiving domperidone (dose not stated).[33]
However, in 2 other studies in 10 healthy volunteers receiving a single dose of domperidone
20mg[34] or 22 patients with reflux oesophagitis
receiving domperidone 20 mg/day for 14 days in
addition to antacids and alginate,[35] no change in
LOSP from placebo values was seen.
Furthermore, in contrast to its inhibitory effect
on upper gastrointestinal motility, dopamine has a
stimulatory effect on colonic motor activity.[36] Intravenous domperidone 0.4 mg/kg significantly
inhibited increased rectosigimoid colon motor activity after intravenous dopamine 50 g/kg and the
early and late increase in motor activity occurring
postprandially in 12 healthy volunteers.[36] Oral
domperidone l00mg, administered as 5 doses over
36 hours, did not alter the stress-induced inhibition
of fasting migrating motor complexes in the small
bowel in 7 healthy volunteers.[37]
© Adis International Limited. All rights reserved.
2.2.1 Effects or the Stomach and Duodenum
Effects or Pressure Waves
Two early trials midied the effect of domperidone on gastric and duodenal molility by measuring intraluminal pressure waves.[38,39] Intravenous
domperidone 8mg increased the duration of contractions (from 3.6 to 9.4 seconds) in the distal part
of the stomach (antrum) in 10 healthy volunteers,[38] and 20mg increased the duration and frequency of antral contractions in 30 patients with
dyspepsia.[39]
Intravenous domperidone 8mg also increased
the frequency (from 1.0 to 3.2 per minute), amplitude (from 9.0 to 16.0mm Hg) and duration (from
3.0 to 4.5 seconds) of duodenal contractions in 10
healthy volunteers.[38] However, there appeared to be
no effect on the overall frequency of duodenal
contractions in 30 patients with dyspepsia after
intravenous domperidone 20mg, despite decreases
in the number of isolated duodenal contractions in
those patients with spontaneous duodenal activity
(>5 contractions per 10 min).[39]
Effects on Gastric Emptying
A review of early studies concluded that intravenous domperidone 20mg appeared to increase
gastric emptying in both healthy volunteers and patients with dyspepsia or delayed gastric emptying
from other causes.[19] Single oral doses of domperidone 30mg, but not 1.5mg, increased gastric
emptying of liquids in patients with delayed emptying and slowed emptying in those in whom it was
Drugs 1998 Sep; 56 (3)
Domperidone: A Review
pathologically accelerated. [14] Similarly, single doses
of domperidone 40mg significantly increased solid
emptying rates in patients with diabetic gastropathy.[2] However, in patients with diabetic gastropathy who had been receiving domperidone 60
ing/day for up to 51 days, the mean gastric emptying rate of solids after a single dose of domperidone 40mg was similar to that with placebo.[2]
Patients with diabetic gastropathy receiving oral
domperidone 40 to 120 mg/day for 1 to 31 months.
had improved solid gastric emptying rates (9 to
34%) [table II]. Improvements in gastric emptying
reached statistical significance in only 2 studies,
but this may be a result of small patient numbers
in most trials. After 4 weeks, domperidone 80
mg/day and cisapride 40 mg/day decreased gastric
emptying time to a similar extent (from 146 to 83
min vs from 105 to 79 min) in patients with diabetic
(n = 9) or idiopathic (n = 1) gastroparesis in an
open-label trial.[45]
Electrogastrographic Effects
Surface recording of myoelectrical activity of the
stomach can be used to evaluate patients with
symptoms of gastropathy.[11] Electrogastrographic
(EGG) studies in patients with diabetes mellitus
with symptoms of gastropathy showed abnormalities of gastric electrical rhythms irrespective
of the presence or absence of delayed gastric empThe EGG recordings from 23 patients
© Adis International Limited. All rights reserved.
433
with type 1 diabetes mellitus and symptoms of gastropathy (14 with and 9 without delayed gastric
emptying) showed a higher proportion of waves
with a frequency of 1 to 2 cycles per minute (cpm)
and a lower proportion with a frequency of 3 cpm
than seen in 12 healthy controls.[48]
The results of 2 small trials suggest that domperidone is effective in converting the disturbed
gastric myoelectrical rhythm towards normal EGG
wave patterns in patients with type 1 diabetes
mellitus.[41,49] After a 4-week single-blind administration of domperidone (dosage not stated) to 23
patients with type 1 diabetes mellitus and gastropathy, 16 symptomatic responders (9 with delayed
and 7 with normal gastric emptying) were randomised to receive either domperidone or placebo
(domperidone withdrawal) for a further 4 weeks.[49]
Among patients with delayed gastric emptying,
EGG recordings from those who continued to receive domperidone (n = 5) showed significantly
increased 3 cpm waves (p < 0.05) and significantly
decreased 1 to 2 cpm waves (p < 0.01) compared
with those who received placebo (n = 4).[49] EGG
recordings from patients with normal gastric emptying receiving domperidone (n = 4) showed a significant decrease in 4 to 9 cpm waves (p < 0.01)
and a nonsignificant increase in 3 cpm waves
compared with those receiving placebo (n = 3).[49]
After 6 months, 4 of 6 patients with type 1 diabetes
Drugs 1998 Sep; 66 (3)
Prakash & Wagstaff
434
mellitus and symptoms of gastropathy (refractory
to other prokinetic and antiemetic agents) receiving domperidone 80 mg/day showed normal 3 cpm
EGG wave patterns in an open-label trial.[41]
2.3 Endocrine Effects
2.3.1 Plasma Prolactin Levels
Administered orally or intravenously, domperidone is a potent stimulant of prolactin release, although peak prolactin levels are consistently
higher in females than in males.[19] The administration of a single oral or intravenous dose of domperidone 10 or 20mg significantly increased plasma
and serum prolactin levels from pretreatment values (from 2.5 to 9,5 g/L to 19 to 125 g/L) in
small numbers (n = 5 to 17 per group) of healthy
volunteers, or patients with type 1 diabetes mellitus
or acute or chronic schizophrenia.[150-55] Serum prolactin levels peaked 30 minutes after intravenous
administration and 60 minutes after intramuscular
or oral administration of domperidone; prolactin
levels returned to baseline values after 8 hours.[51]
Oral domperidone 60 mg/day for 4 weeks also
resulted in 5-fold increases in prolactin levels over
baseline values in 4 patients with gastro-oesophageal
reflux disease[51] and in 49 patients (diagnoses not
provided).[56] There appears to be no relationship
between the dosage of domperidone or the duration
of treatment and the increase in plasma prolactin
levels.[51,56] However, the duration of type 1 diabetes mellitus may influence the prolactin response
to domperidone. The increase in prolactin levels
after intravenous domperidone l0mg was significantly lower in 8 patients with type 1 diabetes mellitus of 11 to 18 years' duration (3.5 times baseline
values) than in 7 healthy controls or 8 patients with
type 1 diabetes mellitus of 1 to 9 years' duration
(both about 5 times baseline values).[52] The investigators suggest that reserves of prolactin which are
available for acute release are reduced in patients
with long-standing type 1 diabetes mellitus.[52]
Age of the recipient may also affect the prolactin response to a single oral dose of domperidone. The prolactin response in elderly healthy
volunteers receiving domperidone 20mg was sig© Adis international Limited. Aii rights reserved.
nificantly lower than in young healthy volunteers,
but the response was similar in young patients with
acute schizophrenia and elderly patients with chronic
schizophrenia receiving domperidone 20mg.[54]
2.3.2 Plasma Insulin Levels
Although some investigators have suggested a
role of dopamine and its receptor subtypes in regulating insulin secretion,[57] available data are inconclusive. Intravenous infusion of dopamine 0.5
to 3 g/kg min for 30 minutes did not alter the
blood glucose or plasma insulin levels in 7 healthy
volunteers.[58] However, a similar infusion of
dopamine significantly increased the plasma insulin levels from baseline values (86.74 vs 59.48
pmol/L, p < 0.01) in 19 hypertensive patients who
had been pretreated with labetalol 0.8 to 1.2 g/day
for 7 days.[57] A dopamine-induced rise in plasma
insulin levels was not observed in these patients
after pretreatment with domperidone 40 mg/day
for 7 days.[57]
The effects of domperidone on glucose-induced
insulin secretion are equivocal. While increases in
plasma insulin levels after an oral glucose load of
75g were similar after a single oral dose of domperidone 10mg or placebo in 9 volunteers (330 to
373 pmol/L, approximate values from graph),[55]
plasma insulin levels after intravenous glucose 0.5
mg/kg were higher in 8 volunteers who received
oral domperidone l00mg 90 minutes beforehand
than in 8 volunteers who received placebo (244
vs 172 pmol/L after 10 minutes, values from
graph).[59]
2.3.3 Effects on Other Hormones
The effects of domperidone on plasma aldosterone levels have been investigated in several trials
involving small groups (6 to 10 per trial) of healthy
volunteers[50,60,61] or in 5 patients with essential
hypertension.[50] While intravenous domperidone
l0mg appeared to have little effect on plasma aldosterone levels in one trial,[50] an intravenous dose of
40mg and an oral dose of 20mg in two further
trials decreased the plasma levels of aldosterone
from baseline values by about 15%.[60,6l]
Administration of oral domperidone 20mg or
intravenous domperidone 10 to 20mg did not apDrugs 1998 Sep; 56 (3)
Domperidone: A Review
435
Table III. Overview of the pharmacokinetic properties of oral domperidone in healthy volunteers
Domperidone
10mgsd
60mga sd
60mgb sd
No. of volunteers
5
7
4
F(%)
Mean Cmax (g/L)
17.6
12.7
23
80
23.6
65
12-18
tmax (h)
0.5
0.5
2
AUC (g/L • h)
t½ (h)
58
249
463
0.5-1.0
10mgqid
10mg qidc
20mg qidc
24
11.35
1.14
24
13.86
1.09
157.36
163.81
40mg qidc
24
14.13
1.23
181.26*
Reference
67
67
67
7-16
68
69
69
69
a Tablet administered to fasting volunteers.
b Tablet administered 90 minutes after a standard meal.
c After 5 days and normalisation of individual values to the 40mg dose.
AUC = area under the plasma concentration-time curve; Cmax = peak plasma concentration; F = systemic bioavailability; qid = 4 times daily;
sd = single dose; t½ = elimination half-life; tmax = time to Cmax; * indicates significantly higher value than with 10 and 20 mg qid (p < 0.05).
pear to affect plasma rcnin activity,[50,60,61] mealstimulated serum gastrin levels, [62] plasma levels of
basal[63] or hypoglycaemia-stimulated[64] argininevasopressin, or plasma levels of adrenocorticotrophin or cortisol[50] in groups of 6 to 16 healthy
volunteers or 5 patients with essential hypertension.[50] Oral domperidone 60 mg/day for 4 weeks
significantly decreased plasma testosterone levels
(855 vs 301 g/L, p < 0.05) but did not affect the
levels of follicle-stimulating hormone or luteinising hormone in 49 male patients (diagnoses not
stated).[56] The plasma levels of testosterone were
similar to pretreatmerit values 2 weeks after
domperidone withdrawal.[56]
2.4 Other Effects
Domperidone, lOmg intravenously[50] or orally
as a single close of 20mg'[61] or as 40 mg/day for 7
days[65] did not affect blood pressure or heart rate in
healthy volunteers (n = 7 to 10 per trial)[50,61,65]
or in 5 patients with essential hypertension.[50] A
single oral dose of domperidone 60mg led to a
small but significant increase in mean arterial pressure (92 vs 96mm Hg) in 6 healthy volunteers.[66]
A single oral dose of domperidone 20 [61] or
60mg[66] or a total intravenous dose of 40mg'60' did
not affect renal function in healthy volunteers.[60,61,66]
3. Pharmacokinetic Properties
Since the publication of the previous review of
domperidone in Drugs,[19] very few additional data
have been published regarding the pharmacoki© Adis International Limited. All rights reserved.
netic properties of domperidone in healthy volunteers (table III). The pharmacokinetic properties of
the oral formulation of domperidone are overviewed in this section. There are no available data
on the pharmacokinetic properties of domperidone
in patients with type 1 diabetes mellitus with delayed gastric emptying, in whom drug absorption
may be disturbed.
3.1 Absorption and Distribution
In healthy volunteers, peak plasma domperidone concentrations (Cmax) were reached within 2
hours (tmax) after a single oral dose (table III). The
systemic bioavailability of domperidone administered on an empty stomach was 12 to 18% and was
increased to 23.6% in 1 study by administering the
drug 90 minutes after a meal. Domperidone appears to undergo rapid 'first-pass' metabolism either
in the gut wall or in the liver, as only 7% of the
administered drug is excreted unchanged in the faeces.[70] About 92 to 93% of domperidone has been
estimated to be bound to plasma proteins.[67]
Animal data indicate that orally administered
domperidone is widely distributed in the body.[7l]
However, studies in healthy volunteers indicate
that domperidone is unable to cross the blood-brain
barrier.[50,62,63]
3.2 Metabolism and Excretion
Oxidative N-dealkylation and hydroxylation
to 2 major metabolites, neither of which has significant activity, seem to be the most important
Drugs 1998 Sep; 56 (3)
436
Prakash & Wagstaff
pathways for the metabolism of domperidone in
humans.[70] Although the steady-stale pharmacokinetics (Cmax and tmax) were proportional to dos-age
after domperidone 10, 20 and 40mg 4 times daily
for 5 days, the highest dosage led to a signif-icantly
higher area under the plasma concentration-time
curve than the 2 lower dosages in a random-ised,
double-blind, crossover trial in 24 healthy
volunteers[69] (table III).
The plasma elimination half-life (t½) of domperidone ranged from 7 to 16 hours after oral administration of 10mg 4 times daily.[68] The t½ is
prolonged to up to 20.8 hours in patients with severe renal dysfunction (serum creatinine >530
mol/L).[19] However, since renal clearance is low
compared with total plasma clearance (42 L/h),
domperidone is unlikely to accumulate in patients
with renal dysfunction.[19] After oral administration of 14C-domperidone 40mg to healthy volunteers, 31% of the radioactivity was excreted in
urine (mostly within 24 hours) with only 0.43% of
the administered dose present as unchanged drug;
66% of the radioactivity was excreted in the faeces
over 4 days (6% of the administered dose as unchanged drug).[70]
3.3 Drug Interactions
The tmax of pramipexole 0.25mg was significantly reduced with concomitant administration
of domperidone 30mg in 12 healthy volunteers.[72]
However, the pharmacokinetic disposition of aspirin 350mg was not altered by the addition of domperidone l0mg in a randomised, crossover trial in
6 healthy volunteers.[73] Similarly, pretreatment
with domperidone 20mg did not alter any of the
pharmacokinetic parameters of ropinirole 0.8mg in
9 healthy volunteers.[74]
4. Clinical Efficacy
The efficacy of oral domperidone has been investigated in double-blind, single-blind and nonblind trials of 1 to 48 months' duration in patients
with type 1 diabetes mellitus and symptoms of
gastropathy. Domperidone 20mg 4 times daily appears to be effective in these patients and in patients
© Adis international Limited. AH rights reserved.
whose symptoms of gastropathy are unresponsive
to other prokinetic or antiemetic agents.
Much of the data discussed in this section are
available only in abstract reports (see table IV).
Also, many of the trials in patients with symptoms
of gastropathy who had been treated with oral prokinetic agents have methodological limitations such
as inadequate numbers of patients, lack of randomisation, lack of placebo control or poor definition of inclusion and exclusion criteria for patient
selection.[3] Most of the trials were conducted in
small numbers of patients with type 1 diabetes
mellitus in whom blood glucose levels were not
reported.
The most common method of evaluating the
efficacy of domperidone treatment was assessment
of symptomatic improvement. This was achieved
by measuring the reduction in total symptom score,
reduction in intensity and frequency scores of
symptoms, change in symptom score on a visual
analogue scale, or physician- and/or patient-rated
global evaluation. Although all trials evaluated
severity of symptoms on an ordinal scale from 0
(absent) to 3 (severe), there were minor differences
in the symptoms selected for evaluation (see table
IV). Other efficacy parameters included hospitalisation rale, and improvement in quality of life,
measured on the physical and mental component
summary scores of the Medical Outcomes 36-item
Short Form Health Survey (SF-36), compared with
pretreatment values.
4.1 Symptomatic Improvement
Most trials with symptomatic improvement as
an end-point (table IV) included patients with
type 1 diabetes mellitus who presented with
symptoms
of anorexia, early satiety, nausea, vomiting, abdominal distension/bloatedness and abdominal
pain.
4.1.1 Short Term Trials
As it is difficult to demonstrate the efficacy of
prokinetic agents in patients with symptoms of
gastropathy, the US Food and Drug Administration
recommended an 'enriched' design for domperidone trials to identify treatment responders.[79]
Drugs 1998 Sep; 56 (3)
Domperidone: A Review
Adis International Limited. All rights reserved.
437
Drugs! 098 Sep; 56 (3)
438
Following an initial nonblind or single-blind phase
where all patients received domperidone, 4 trials
compared the effects of domperidone with placebo
(domperidone withdrawal) in a subsequent randomised single-blind or double-blind phase (table
IV). In these trials, 66 to 88% of patients responded
(good or excellent improvement in global assessment of symptoms or significant reduction in total
symptom score) to domperidone 40 to 80 mg/day
in the noncomparative phase. Those responding were
randomly assigned to either continue domperidone
40 to 80 mg/day or receive placebo for a further
period of 1 month in a randomised, single-blind or
double-blind fashion (extended phase).
Patients in whom domperidone was withdrawn
in the extended trial phase (placebo-control) had a
significant increase in median total symptom
scores and a deterioration in global assessment rating compared with patients who continued to receive domperidone 40 to 80 mg/day (table JV).
Prakash & Wagstaff
Patients with delayed gastric emptying in whom
domperidone was withdrawn in the extended phase
deteriorated to a greater extent than those continuing with domperidone (p < 0.05) in 2 studies.[4,77]
However, this effect was not observed in patients
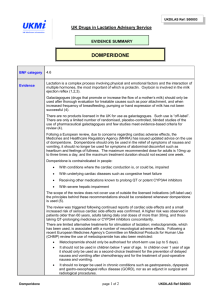
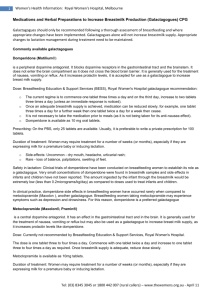
with normal gastric emptying (fig. 2).
In a double-blind trial (n = 93), domperidone 80
mg/day and metoclopramide 40 mg/day improved
total symptom scores to a similar extent and were
considered equivalent in global evaluations.[78]
Similarly, in a small open-label crossover trial, [45]
domperidone 80 mg/day appeared to be equivalent
to cisapride 40 mg/day in reducing total symptom
score in 10 patients with diabetic gastropathy (ta-ble
IV).
Preservation of autonomic function in patient5
with type 1 diabetes mellitus with gastropathy may
indicate a greater likelihood of sump improvement
with domperidone. One small trial (n = 16) found
that patients with type 1 diabetes mellitus with gastropathy who improved with dom-
Fig. 2. Effect of domperidone (DOM) on symptoms of gastropathy in patients with insulin-requiring diabetes mellitus. Mean total
symptom scores (TSS) were significantly decreased after DOM 80 mg/day for 4 weeks, in 208 of 269 patients with insulin-requiring
diabetes mellitus with delayed or normal gastric emptying, in a single-blind enrichment phase. Treatment responders were
randomised to either continue DOM or receive placebo for a further 4 weeks in a double-blind fashion.[4,75] * p < 0.05 vs placebo; **
p < 0.001 vs baseline.
© Adis International Limited. All rights reserved.
Drugs 1998 Sep; 56 (3)
Domperidone: A Review
peridone had better autonomic function than patients who did not respond to domperidone.[80] The
investigators suggested that prior autonomic function testing in patients with diabetic gastropathy
may be useful in defining patients whose symptoms are more likely to respond to domperidone.
4.1.2 Long Term Trials
A sustained improvement in symptoms of
gastropathy has been shown in groups of patients (n = 5 to 66 per trial) receiving domperidone for up to 12 years in several small, nonblind
trials. [42-44,76,81,82]
In 14 of 24 patients with diabetes mellitus,
domperidone 80 mg/day significantly reduced the
total symptom score at 12 months by 58.5% from
baseline values (from 10.6 to 4.4, p < 0.0001).[8] In
2 trials which included 10[43] and 17144] patients with
symptoms of gastropathy associated with
diabetes, surgical procedure, scleroderma or unknown (idiopathic) aetiology,'43'44^ domperidone
40 to 120 mg/day over 21 and 48 months led to
sustained, significant decreases in total symptom
scores from baseline values, i.e. by 75% (from 8.4
to 2.1,. p < 0.05), and by 68% (from 4.1 to 1.3, p<
0.05), respectively. Domperidone 80 mg/day administered for an average of 1.73 years (range 0.3
to 8 years) improved symptoms of gastropathy in
63 of 66 patients (95%) with type 1 diabetes mellitus (patient-rated symptom response was excellent in 33, good in 25 and fair in 5 patients).[42]
4.1.3 Trials in Patients with Symptomatic
Gastropathy Refractory to Other Agents
The results of small, nonblind trials suggest that
domperidone may also be effective in patients with
symptomatic gastropathy unresponsive to other
prokinetic and autiemetic agents.
Domperidone 80 mg/day for 6 months reduced
the mean symptom score from 17.8 (of a total
possible 33) to 3.7 (79% decrease, p < 0.01) in 6
diabetic patients with nausea and vomiting who
failed to improve with metoclopramide, prochlorperazine, chlorpromazine or trimethobenzamide.[41]
A r Prospective trial in 57 patients with symptoms
of diabetic gastropathy, who had previously discontinued metoclopramide because of either lack
Adis International Limited. All rights reserved.
439
of efficacy or adverse events, also found that administration of domperidone 40 to 80 mg/day led
to a markedly or moderately favourable response
in 70% of patients, who successfully continued therapy with domperidone for a median of 377 days.[83]
Similarly, domperidone 40 to 80 mg/day for up
to 144 months significantly reduced the severity
scores for nausea, vomiting, early satiety and eructation in 5 patients with type 1 diabetes mellitus
whose symptoms of nausea and vomiting had not
responded to 'standard' antiemetic therapy.[82]
However, the severity of other symptoms such as
regurgitation, heartburn, distension and flatulence
did not improve with domperidone.
The efficacy of domperidone was similar to that
of cisapride (dosages not stated) in a nonblind trial
in 55 diabetic patients with gastropathy unresponsive to metoclopramide; in 29 patients the reduction of symptom severity peaked at 12 months [a
decrease in total symptom score from 9.3 (of total
possible 15) to 3.9, 58% decrease] and some benefit was sustained in 13 evaluable patients after
24 months (total symptom score of 6.0, a 35%
decrease from baseline). [84]
The addition of cisapride 80 mg/day to domperidone 80 mg/day for a mean of 9 months also
significantly improved the symptoms of gastropathy such as nausea, vomiting, satiety and bloating in 9 patients with type 1 diabetes mellitus who
had not shown an adequate response with either
agent alone; abdominal pain did not improve in
these patients.[85]
4.2 Effects on Quality of Life
Quality of life was assessed in patients with
insulin-requiring diabetes mellitus with symptoms
of gastropathy who underwent an 'enriched' trial[4,75]
with domperidone (efficacy reported in table IV).
Impairment of quality of life at baseline was demonstrated in 269 patients; scores on the SF-36 questionnaire were significantly lower than those in the
general population. [86,87] Evaluable patients (in the
single-blind enrichment phase), in whom the symptoms of gastropathy improved after domperidone
80 mg/day (n = 208), showed significant improve-
Drugs 1998 Sep; 56 (3)
Prakash & Wagstaff
440
ment in the physical and mental component summary scores of the SF-36 compared with those in
whom symptoms did not respond to treatment (n =
61) after 4 weeks. In the second (double-blind)
phase of the trial, responders to domperidone who
were randomised to continue active treatment for a
further 4 weeks (n = 104) continued to show improvement on the physical component summary
score, while placebo recipients (n = 99) showed
significant worsening. There was a significant difference in physical component summary scores between domperidone and placebo recipients at endpoint (+0.65 vs -1.77, p 0.05). The deterioration
in mental component summary scores was similar
in both groups.[86,87]
Several smaller trials also indicate improvement
in quality of life with domperidone treatment. The
administration of domperidone (dosage not stated)
for 12 months led to a significant symptomatic improvement (mean total symptom score decreased
from 9.5 to 4.87, p < 0.01) in 7 patients with diabetic gastropathy in a nonblind trial and the quality-of-life status, as measured by the Sickness Impact Profile, improved in 6 (median improvement
of 22%).[88] Similarly, 15 of 17 patients receiving
domperidone 80 mg/day for up to 48 months reported physical domains of quality of life as good
to excellent, and 13 rated their general health as
better than before treatment.[44]
istration of domperidone 40 to 120 mg/day for up
to 79 months led to an increase in weight of 5 to
7kg, compared with pretreatment values, in small
numbers of patients (n = 5 to 17 per trial) with
symptoms of diabetic, idiopathic, sclerodermal or
postsurgical gastropathy.[43,44,82]
5. Tolerability
Although there are no published data from trials
specifically designed to evaluate its tolerability,
oral domperidone 40 to 120 mg/day administered
from 1 month to 12 years was well tolerated in
clinical trials involving patients with type 1 diabetes mellitus and gastropathy (section 4), In fact,
the folerabilitv of domperidone 80 mg/day was
similar to that of placebo in a 4-week, randomisec
double-blind trial in 208 patients with type 1 diabetes mellitus and gastropathy.[89]
The most common adverse events appear to be
related to prolactin secretion. Breast symptoms,
such as enlargement, soreness, secretion or tenderness, related to elevated prolactin levels, have been
reported in 10 to 20% of patients.[43,77] However,
breast symptoms occurred in 3 of 13 patients receiving domperidone and in a similar number of
4.3 Other End-points
The effect of domperidone on the frequency of
hospital admission of patients with symptoms of
gastropathy has been evaluated in 5 small nonblind
trials. Domperidone 40 to 120 mg/day for up to 8
years significantly decreased the hospital admission rate from pretreatment values in patients with
gastropathy in 3 trials.[42-44] However, hospital admission rates remained unchanged in another trial
(from 1.1 to 1.0 per patient per year)[84] when domperidone (dosage not stated) was administered for
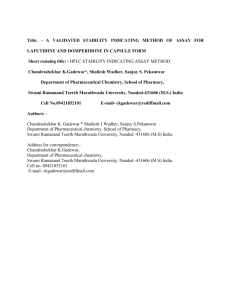
up to 36 months (fig. 3).
The symptoms of gastropathy may be severe
enough in some patients to cause nutritional deficiencies and weight loss.[ll] The nonblind admin-
© Adis International Limited. All rights reserved,
Fig. 3. Decrease in hospitalisation rates in patients with gastropathy receiving domperidone. Hospitalisation rates in patients
with diabetic, idiopathic, scleroderma! or postsurgica! gastropathy receiving domperidone 40 to 120 mg/day in open-label
trials of up to 3 years duration [42-44.84] * p < 0.05 vs baseline.
Drugs 1998 Sep; 56 (3)
Domperidone: A Review
patients receiving placebo in a small double-blind,
crossover trial.[76] These symptoms were mild to
moderately severe and did not necessitate withdrawal of drug therapy.
A retrospective analysis of data from 57 patients
with diabetes mellitus with symptoms of gastropathy treated with domperidone 40 (n = 4) or 80
(n = 53) mg/day for up to 3 years (median of 246
days) reported adverse events in 22 patients.[83]
Mild to moderate prolactin-related adverse events
(such as galactorrhoea, breast tenderness/fullness
and amenorrhoea) were observed n 16% of patients. Other adverse events reported by > 1 patient
were gastrointestinal symptoms (11%), itching or
rash (5%), muscle cramps (4%) and headache
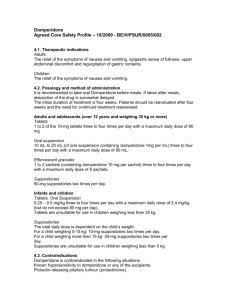
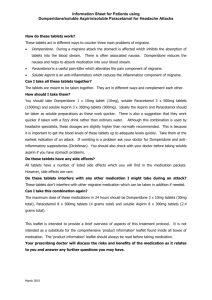
(4%)[83] (fig. 4).
After 4 weeks of treatment, the severity of adverse events [scored on a scale from 0 (absent) to
3 (severe); total possible score 18] with domperidone 80 mg/day was significantly less than that
with metoclopramide 40 nig/day (2.5 vs 4.5. p <
0.02) in 93 patients with type 1 diabetes mellitus
in a randomised, double-blind, multicentre trial.[78]
Domperidone recipients had a significantly lower
incidence of somnolence and reduced mental acuity than those receiving metoclopramide.[78]
Although CNS effects with oral domperidone
arc rare in (he presence of an intact blood-brain
barrier, acute dystonic reactions such as orolingual
dyskinesia, oculogyric crisis and opisthotonus
after oral domperidone 20 and 50mg have been
described in 2 women aged 16 and 28 years with
polycystic ovary syndrome.[90] The investigators
suggest that hyperestrogenism in these patients
may have increased the risk of acute dystonic reactions with domperidone. [90]
Because intravenous administration of domperidone has been associated with an increased risk
of cardiovascular events, such as cardiac arrest,[91,92] parenteral formulations of domperidone
are no longer available for clinical use.
6. Dosage and Administration
Domperidone is available as l0mg tablets, a 5
mg/ml oral suspension and 30mg suppositories.[93]
© Adis International Limited. All rights reserved.
441
Fig. 4. Adverse events (AE) in patients receiving domperidone.
Results of a retrospective study in 57 patients with type 1 diabetes mellitus with gastropathy who had discontinued metoclopramide because of adverse effects or lack of efficacy and who
then received domperidone 40 to 80 mg/day for 47 to 377
days.[83] Prolactin-related AE included galactorrhoea, breast
tenderness or fullness and amenorrhoea. Gastrointestinal (Gl)
symptoms were not defined.
The recommended dosages of domperidone in
adults and in children are shown in table V.
The most commonly used dosage of oral domperidone in clinical trials in patients with type 1
diabetes mellitus anda gastropathy (section 4) was
80 mg/day (range from 40 to 120 mg/day). Although domperidone is not recommended for long
term use and a course of treatment with domperidone for the management of patients with nausea
and vomiting should not exceed 12 weeks, [93] domperidone 40 to 80 mg/day has been used successfully for up to 8 to 12 years in long term trials in
patients with type 1 diabetes mellitus with symptoms of gastropathy.[42,82] Domperidone may be used
with caution in patients with renal impairment.1931
7. Place of Domperidone in the
Management of Diabetic Gastropathy
Symptoms of diabetic gastropathy are often
chronic and difficult to treat. Achieving glycaemic
control and modification of dietary intake such as
ingestion of small frequent meals with low fat and
fibre content may improve gastric emptying in
some patients with diabetes mellitus.[11,94] However, the rationale for pharmacotherapy of diabetic
Drugs 1998 Sep; 56 (3)
442
Table V. Recomme'nded dosage of domperidone for the
management of nausea and vomiting due to various causes[93]
patients with gastropathy is based on the occurrence of gastrointestinal symptoms, irrespective of
delayed or normal gastric emptying.[94] Surgical
procedures such as a venting gastrostomy for gastric decompression and a jejunostomy catheter for
enteral feeding are reserved for patients with severe gastroparesis.[8,11]
Drugs commonly used in the treatment of patients with diabetic gastropathy include metoclopramide, cisapride and domperidone. However,
there is a lack of quality data comparing these drugs.
The available data on the efficacy of domperidone
in the management of patients with diabetic gastropathy have several limitations: few trials have been
published in full, blood glucose levels were not
monitored in included patients, none of the fully
published trials compared the effects of domperidone with other gastrokinetic agents, and most
trials were nonblind and conducted in small numbers of patients.
Nonetheless, oral domperidone 40 to 80 mg/day
significantly reduced the intensity and frequency of
symptoms of gastropathy from baseline values in
all available trials. The efficacy of domperidone in
reducing the symptom severity of diabetic gastropathy was significantly greater than that of placebo
and similar to that of metoclopramide 40 mg/day
in double-blind trials and was similar to that of
cisapride 40 mg/day in nonblind trials. In 'enriched' trials, domperidone led to improvement in
the symptoms of 66 to 88% of patients in the initial
© Adis International Limited. All rights reserved.
Prakash & Wagstaff
nonblind or single-blind phase. In the subsequent
randomised single-blind or double-blind phase, the
subgroup of patients with delayed gastric emptying who continued with domperidone showed significantly less deterioration of symptoms after 4
weeks than did those receiving placebo. There was
a significant reduction in hospital admission rates
in patients with gastropathy receiving domperidone. Quality of life also improved in patients
whose symptoms responded with domperidone as
compared with placebo recipients.
The administration of domperidone has shown
sustained symptomatic benefit in patients with diabetic gastropathy for up to 12 years. Diabetic patients with preserved autonomic function and those
with delayed gastric emptying appear to respond
more favourably to domperidone than those in
whom autonomic function is damaged or those who
have normal gastric emptying. In addition, domperidone may be effective in patients who are refractory to other agents and the combination of
domperidone with gastrokinetic agents with a different mechanism of action, such as cisapride, may
improve symptoms of patients who do not show an
adequate response with domperidone alone.
The tolerability profile of domperidone 80
mg/day is significantly superior to that of metoclopramide 40 mg/day. Metoclopramide has been associated with adverse CNS effects in 20% of recipients.[10] Although domperidone administration
causes elevation of plasma prolactin levels, prolactin-related adverse events such as galactorrhoea,
breast tenderness and fullness and amenorrhoea
have been observed in only 16% of domperidone
recipients. No serious adverse events have been reported with the use of domperidone.
In conclusion, domperidone 40 to 80 mg/day
appears to be an effective and well tolerated agent
for the management of symptoms of gastropathy in
patients with type 1 diabetes mellitus. If is at least
as well tolerated as other treatment options. Symptoms of gastropathy which are refractory to other
gastrokinetic agents may respond to domperidone
and symptomatic relief is sustained over extended
periods.
Drugs 1998 Sep; 56
(3)
Domperidone: A Review
References
1. Horowitz, M, Fraser R. Disordered gastric motor function in
diabetes mellitus. Diabetologia 1994; 37 (6): 543-51
2. Horowitz M, Harding PE, Chatterton BE, et al. Acute and
chronic effects of domperidone on gastric emptying in diabetic autonomic neuropathy. Dig Dis Sci 1985 Jan; 30 : 1-9
3. Sturm A, Holtmann G, Goebell H. Treatment of patients with
gastroparesis: a meta-analysis of prokinetics [abstract]. Gastroenterology 1997 Apr; 112 Suppl.: A833
4. Patterson D, Silvers D, Kipnes M, et al. Does gastric emptying
status in patients with diabetes influence the effectiveness of
dompcridone? [abstract]. Gastroenterology 1997 Apr; 112
Suppl.: A804
5. Horowitz M, Maddox AF, Wishart JM, et al. Relationships between oesophageal transit and solid and liquid gastric emptying in diabetes mcllitus. Eur J Nucl Med 1991 18: 229-34
6. Mearin F, Malagelada J-R. Gastroparesis and dyspepsia in patients with diabetes mellitus. Eur J Gastroenterol
Hepatol 1995; 7 (8): 717-23
7. National Diabetes Data Group (U.S.). Digestive diseases and
diabetes. In: Diabetes in America. 2nd ed. Bethesda: National
Institute of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 1995: 464-6
8. Koch KL. Diabetic gastropathy: a clinical overview. Patient
Care 1998 Jan; Supp. I: 1-10
9. Feldman M, Schiller LR. Disorders of gastrointestinal motility
associated with diabetes mellitus. Ann Intern Med 1983; 98:
378-84
10. Drenth JPH. Engels LGJB. Diabetic gastroparesis: a critical
reappraisal of new treatment strategies. Drugs 1992 Oct; 44:
537-53
11. Nilsson P-H. Diabetic gastroparesis: a review. J Diabetes Complications 1996 Mar-Apr; 10: 113-22
12. Jones KL, Horowitz M, Berry M, et al. Blood glucose concentration influences postprandial fullness in IDDM. Diabetes
Care 1997; 20 (7): 1141-5
13. Schvarcz E, Palmer M, Aman J, et al. Physiological hypcrglycemia slows gastric emptying in normal subjects and patients
with insulin-dependent diabetes mellitus. Gastroenterology
1997:113:60-6
14. Samsom M, Akkermans LMA, Jebbink RJA, et al. Gastrointestinal motor mechanisms in hypcrglycacmia induced delayed
gastric emptying in type I diabetes mellitus. Gut 1997; 40:
641-6
15. Hebbard GS, Samsom M, Andrews JM, et al. Hyperglycemia
affects gastric electrical rhythm and nausea during intraduodenal triglyceride infusion. Dig Dis Sci 1997; 42 (3): 568-75
16. Schvarcz E, Palmer M, Ingberg CM,et al. Increased prevalence
of upper gastrointestinal symptoms in long-term type 1 diabetes mellitus. Diabetic Med 1996; 13: 478-81
17. Hebbard GS. Samsom M. Sun WM. et al. Hyperglycemia affects proximal gastric motor and sensory function during
small intestinal triglyceride infusion. Am J Physiol 1996; 271 :
G814-9
18. Kendall BJ, McCallum RW. Gastroparesis and the current use
of prokinetic drugs. Gastroenterologist 1993 Jun; 1: 107-14
19. Brogden RN, Carmine AA, Heel RC, et al. Domperidone: a
review of its pharmacological activity, pharmacokinetics and
therapeutic efficacy in the symptomatic treatment of chronic
dyspepsia and as an antiemetic. Drugs 1982 Nov: 24: 360-400
20. Corazza GR, Biagi F, Albano O, et al. Levosulpiride in functional dyspepsia: a multiccntric double-blind, controlled trial.
Ital J Gastroenterol 1996; 28: 317-23
© Aclis International Limited. All rights reserved.
443
21. Gatto G, Ricca T, Randazzo MA, et al, Clinical efficacy and
safety of levosulpiride and domperidone in the management
of chronic functional dyspepsia: a double-blind, randomized
clinical trial. Curr Ther Res 1992 May; 51: 715-22
22. Halter F, Staub P. Hammer B, et al. Study with two prokinetics
in functional dyspepsia and GORD: domperidone vs cisapride. J Physiol Pharmacol 1997; 48 (2): 185-92
23. Kohli JD, Glock D, Goldberg LI. Selective DA2 versus DA1
antagonist activity of domperidone in the periphery. Eur J
Pharmacol 1983 Apr 22; 89: 137-41
24. Takahashi T, Kurosawa S, Wiley JW, et al. Mechanism for the
gastrokinetic action of domperidone. In vitro studies in guinea
pigs. Gastroenterology 1991 Sep; 101: 703-10
25. Nascllo AG, Gidali D, dc Sa-Rocha LC, et al. Differential
effects of bromopride and domperidone on cholinesterase
activity in rat tissues. Life Sci 1994 Dec 9; 56: 151-6
26. Kurosawa S, Owyang C. Characterizations of dopamine receptors on gastric smooth muscle and on postsynaptic cholinergic
neurons. Mechanism for the gastrokinetic action of domperidone [abstract]. Gastroenterol Jpn 1993 Aug; 28: 586
27. Sahyoun HA, Costall B, Naylor RJ. On the ability of domeridone to selectively inhibit catecholamine-induced relaxation of circular smooth muscle of guinea-pig stomach. J
Pharm Pharmacol 1982 Jan; 34: 27-33
28. Sahyoun HA, Costall B, Naylor RJ. Catecholamine-induced
relaxation and contraction of the lower oesophageal and pyloric
sphincters of guinea-pig stomach: modification by domperidone. J Pharm Pharmacol 1982 May; 34: 318-24
29. Schuurkes JA, Van Nueten JM. Domperidone improves myogenically transmitted antroduodenal coordination by blocking dopaminergic receptor sites. Scand J Gastroenterol 1984;
96 Suppl.: 101-10
30. Laduron PM, Lcyscn JB. Domperidone, a specific in vitro dopamine antagonist, devoid of in vivo central dopaminergic
activity. Biochem Pharmacol 1979; 28: 2161-5
31. Bero T, Javor T. The effect of loperamide and domperidone on
intestinal transit time measured by breath H2-test [abstract].
Dig Dis Sci 1990 Aug; 35: 1016
32. Weihrauch TR, Forstcr CRF, Krieglstein J. Evaluation of the
effect of domperidone on human oesophageal and gastroduodenal motility by intraluminal manometry. Postgrad Med
J 1979; 55 Suppl. 1:7-10
33. Ding Y-W, Yi S-Q, Ling Q-I. Effect of domperidone and nifedipine on esophageal motility of healthy subjects and several
esophageal diseases [abstract]. J Gastroenterol Hepatol 1993;
8 Suppl. 2: S206
34. Wall in L, Maclsen T, Boesby S. Effect of domperidone on gastro-ocsophageal function in normal human subjects. Scand J
Gastroenterol 1985 Mar; 20: 150-4
35. Blackwell JN, Heading RC, Fettes MR. Effects of domperidone
on lower oesophageal sphincter pressure and gastro-oexophageal reflux in patients with peptic ocsophagilis. Progress
with domperidone. Royal Society of Medicine International
Congress and Symposium Scries No. 36 (1981): 57
36. Wiley .1, Owyang C. Dopaminergic modulation of rcctosigmoid
motility: action of domperidone. J Pharmacol ExpTher 1987
Aug; 242: 548-51
37. Valori RM, Kumar D, Wingate DL. Effects of different types of
stress and of "prokinetic" drugs on the control of the fasting
motor complex in humans. Gastroenterology 1986 Jun; 90:
1890-900
38. Weihrauch TR, Ehl W. Effect of domperidone on the motility
of antrum, pylorus and duodenum in man. Scand J Gastroenlerol 1981; 67 Suppl.: 195-8
Drugs 1998 Sep; 56 (3)
Prakash & Wagsiaff
444
39. Eyre-Brook IA, Smallwood R, Johnson AG. Human antroduodenal motility, pyloric closure, and domperidone. Scand J
Gastroenterol 1984; Suppl. 92: 4-7
40. Harasawa S, Miwa T. Effect of domperidone on gastric emptying in man. Naika Hokan 1981; 28 (3): 67-75
41. Koch KL, Stern RM, Stewart WR, et al. Gastric emptying and
gastric myoelectrical activity in patients with diabetic gastroparesis: effect of long-term domperidone treatment. Am J
Gastroenterol 1989 Sep; 84: 1069-75
42. Patterson D, Meldrum N, Kozarek R, et al. Long-term efficacy
of domperidone in patients with diabetes and symptoms of
gastroparesis [abstract no. 0490]. Diabetes 1997 May; 46
Suppl. 1: 126A
43. Shifflett J, McCallum RW. Longterm efficacy, treatment
outcome and quality of life in patients receiving chronic domperidone therapy for gastroparesis [abstract]. Gastroenterology 1995 Apr; 108 Suppl.: A35
44. Soykan I, Sarosiek 1, McCallum RW. The effect of chronic oral
domperidone therapy on gastrointestinal symptoms, gastric
emptying, and quality of life in patients with gastroparesis.
Am J Gastroenterol 1997 Jun; 92: 976-80
45. Champion MC, Braaten J, Gulenchyn K. Domperidone (Motilium) compared to cisapride (Prepulsid) in the management of
gastroparesis [abstract]. 10th World Congress of Gasiroenteroiogy 1994: 1122P
46. Hongo M, Okuno Y. Diabetic gastropathy in patients with autonomic neuropathy. Diabetic Med 1993; 10 Suppl. 2: 79S-81S
47. Abell TL, Camilleri M, Malagelada J-R. High prevalence of
gastric electrical dysrhythmias in diabetic gastroparesis (abstract]. Gastroenterology 1985; 88: 1299
48. Koch KL, Bingaman S, Stern RM, et al. Gastric myoelectrical
activity in symptomatic diabetic patients with or without
gastroparesis [abstract]. Gastroenterology 1995; 108 (4
Suppl.): A630
49. Koch KL, Bingaman S, Stern RM. Withdrawal study of domperidone vs placebo in diabetic patients: effect on upper gastrointestinal symptoms and gastric myoelectrical a c t i v i t y
(abstract]. Gastroenterology 1995; 108 (4 Suppl.): A630
50. Bernini GP, Lucarini AR, Franchi F, et al. Humoral effects
of ineioclopramide and domperidone in normal subjects and
in hypertensive patients. J F.ndocrinol Invest 1988 Nov; M:
711-6
51. Brown GM, Verhaegan H, Van Wimersma Greidanus TB, et al.
Endocrine effects of domperidone: a peripheral dopamine
blocking agent. Clin Endocrinol Oxf 1981 Sep; 15: 275-82
52. Coiro V, Butturini U, Gnudi A, et al. TSH and PRL responses
to domperidone and TRH in men with insulin-dependent
diabetes mellitus of different duration. Horm Res 1987; 25:
206-14
53. Nerozzi D, Magnani A, Sforza V, et al. Plasma prolactin response to domperidone in acute schizophrenia and schizophreniform illness. Psychiatry Res 1990 Nov; 34: 139-47
54. Nerozzi D, Magnani A, Dastoli C, et al. Prolactin responses to
domperidone in chronic schizophrenia. Psychiatry Res 1992
May; 42: 159-69
55. Vigas M, Klimes I, Jurcovicova J, et al. Acute elevation of
endogenous prolactin does not influence glucose homeostasis
in healthy men. Physiol Res 1993; 42: 341-5
56. Huang X et al. Study of the effect of domperidone on sex hormones among males [abstract]. J Gastroenterol Hepatol 1995;
10 Suppl. 4: 154
57. Forte P, Martin G, Luchsinger A, et al. Effects of dopaminergic
antagonists on dopamine-induced cardiovascular and insulin
© Adis International Limited. All rights reserved.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
secretion actions in hypertensive patients. Int J Clin Pharmacol Ther Toxicoi 1993 Aug; 31: 404-6
Ensinger H, Lindner KH, Gocrtz A, et al. Metabolic and
haemodynamic effects of dopamine plus domperidone in voiunteers.'Res Exp Med 1993 Aug; 193: 241-54
Sommers DK, Vanwyk M, Snyman JR. Effects of pergolide and
dornperidone on insulin and glucose plasma levels after a glucose load. S Afr J Sci 1994 Nov-Dec; 90: 601-3
Worth DP, Harvey JN, Brown J, et al. Dornperidone treatment
in man inhibits the fall in plasma renin activity induced by
intravenous y-1-glutamyl-l-dopa. Br J Clin Pharmacol 1986
May; 21:. 497-502
MacDonald TM. Metoclopramide, domperidone and dopamine
in man: actions and interactions. Eur J Clin Pharmacol 1991
Mar; 40: 225,30
Masci E, Caldara R, Testoni PA, et al. Lack of effect of domperidone on gastrin release: evidence for a peripheral activity
of the drug. Br J Clin Pharmacol 1984 May; 17: 588-90
Chiodcra P, Volpi R, Dels ignore R, et al. Different effects of
metoclopramide and domperidone on arginine-vasopressin
secretion in man. Br J Clin Pharmacol 1986 Oct; 22: 479-82
Chiodera P, Coiro V. Lack of effect of bromocrip!.ine and dompeocione on arginine-vasoprcssm re-spouse to irisuiin-nuhiceu
hypo^lycemia in normal men. Psychoneuroen'Jocrinology
iye>7; 14'. z25-3G
Luehsinger A, Grilii M, Yelasco M. Metoclopramide and domperidone block the antihypertensive effect of bromocriptine
in hypertensive patients. Am J Ther 1998; 5: 81-8
Alien MJ, Ang VTY, Bennett ED. Dompendone, a D.-\2speeific oooamine anUigonist, has no effect on 'he renal <.>r
hac:»iOdyna;nic response to amal riutriuretic p.cr-tiuc m man.
Clin Sci'1988 Dec; 75: 569-75
jleykants j, llendriks R, Meuklernums W, et al. On she pharmacokinetics of domperidone in animals and man. IV. The
pharmacokinctics of-intravenous domperidonc- and its bioavailability following intramuscular, oral and recta! administration, l - u r J Drug Molab Phunnucokinci 1981; (>: 61-70
Reynolds JC, Putnam PE. Prokinetic agents. Gastroenteroi Clin
North Am 1992; 21 (3): 567-96
Raia JJ, Barone JA, Byerly WG, et al. Determination of steadystate dose proportionality ol domperidone in healthy volunteers [abstract!. Pharmacotherapy 1990; 10 (3): 253
Meuidermans W, Hurkmans R, Swysen E, etal. On the pharmacokinetics of domperidone in animals and man. i f f. Comparative study on the secretion and metabolism of clomperidonc
in rats, dogs and man. Eur J Drug Metab Pharmacokinei 1981;
6:49-60 "
Michiels M, Hendriks R, Heykants J. On the pharmacokinetics
of domperidone in animals and man. II. Tissue distribution,
placenta! and milk transfer of domperklone in Use Vistar nil.
Eur J Drug Melab Pharmacokinei 1981; 6: 37-4X
Donaldson KM, Blood P, Peters GR, et al. An evaluation of
some cardiovascular effects of prarnipexole in healthy volunteers and their antagonism by domperidone [abstract). Br j
Clin Pharmacol 1996; 42: 660P-1P
Garg SK, Dhaneria SP, Saha N, et al. Effect of domperidone on
acetyl salicylic acid pharmacokinetics in Indian healthy males
[abstract]. Can J Physio! Pharmacol 1994; 72 Suppl. 1: 308
de Mey C, Enterling D, Meineke I, et al. Interactions between
domperidone and ropinirole, a novel dopajnine Dj-recepior
antagonist. Br J Clin Pharmacol' i99i; 32: 483-8
Patterson D, Silvers D, Kipnes M, el al. Does gastric emptying
status in patients with diabetes influence the effectiveness of
Drugs 1998 Sep; 56 (3)
Domperidone: A Review
domperidone? Janssen Pharmaceutica (Titusville). May 1998
(Data on file)
76. Braun AP. Domperidone in the treatment of symptom of delayed gastric emptying in diabetic patients. Adv Ther 1989
Mar-Apr; 6: 51-62
77. Patterson D, Koch K, Abell T, et al. A multi-center placebocontrolled study of domperidone in diabetic gastroparesis
[abstract]. Gastroenterology 1993 Apr; 104 Suppl.: A564
78. Patterson D. Robin TN. Rothstein D, et al. A double-blind
multicenter comparison of domperidone and metoclopramide
in the treatment of symptomatic diabetic gastroparesis [abstract). Gastroenterology 1994 Apr; 106Suppl.: A554
79. J & J motilium amended NDA filing planned by year-end;
ulcerative colitis therapy ridogrcl is in phase III; HIV therapy
loviride development discontinued. FDC Rep Pink Sheet
1997 Sept 1: 17
80. Rashed H, Abell TL, Cardoso S, et al. Autonomic function
testing correlates with response to domperidone therapy in
patients with diabetes mcllitus and She symptoms of past roparesis [abstract no. 0599). Diabetes 1997 May; 46 Suppl. 1:
155 A
81. Patterson DJ, Botoman VA, Kozarek RA, et al. Domperidone
is effective long-term treatment for diabetic gastroparesis
[abstract]. Gastroenterology 1991 May; l00Suppl.: A137
82. Bingaman S, Koch K. Long-term domperidone treatment for
symptoms of gastroparesis in diabetic patients [abstract no.
1204]. Diabetes 1997 May; 46 Suppl. 1: 315A
83. Kozarek R. Domperidone for symptomatic management of
diabetic gastroparesis in metoclopramide treatment failures.
Adv Ther 1990 Mar-Apr; 7: 61-8
84. Miller M, Patterson D. Natural history of diabetic gastroparesis
treated with cisapride or domperidone [abstract]. Am J Gastroenterol 1991 Sep; 86: 1316
85. Lehmann KA, Patterson DJ. Does combination prokinetic therapy benefit patients with refractory diabetic gastroparesis
[abstract]? Gastroenterology 1995; 108 (4 Suppl.): A636
'§ Adis International Limited. All rights reserved.
445
86. Quigley E, Kline LN, Murray M, et al. Dompcridone improves
health-related quality of life in patients with gastrointestinal
symptoms associated with diabetic gastroparesis [abstract].
Gastroenterology 1997 Apr; 112 Suppl.: A36
87. Quigley E, Leidy NK, Murray M. et al. Domperidone improves
health-related quality of life in patients with gastrointestinal
symptoms associated with diabetic gastroparesis. Janssen
Pharmaceutica (Titusville). May 1998 (Data on file)
88. Abell TL, Rashed H, Cutts T, et al. Autonomic function is a
determinant of quality of life improvement in response to
domperidone therapy [abstract no. 1445]. Diabetes 1997
May; 46 Suppl. 1: 381A
89. Silvers D, Kipncs M, Broadstonc V, et al. Dompcridone significantly improves gastrointestinal symptoms associated with
diabetic gastroparesis (abstract). Gastroenterology 1997 Apr;
112 Suppl.: 826
90. Bonuccclli U, Nocchiero A, Napolitano A, et al. Domperidoneinduced acute dystonia and polycystic ovary syndrome. Mov
Disord 1991; 6(1): 79-81
91. Stern WR. Summary of the 34th Meeting of the Food and Drug
Administration Gastrointestinal Drugs Advisory Committee.
March 15 and 16, 1989 (omcprazolc and dompcridone). Am
J Gastroenterol 1989 Nov; 84: 1351-5
92. Roussak JB, Carey P, Parry H. Cardiac arrest after treatment
with intravenous domperidone [short report]. BMJ 1984; 289:
1579
93. British National Formulary. No. 35. London: The Pharmaceutical Press, 1998 Mar
94. Horowitz M, Fraser RJ. Gastroparesis: diagnosis and management. Scand J Gastroenterol 1995; 213 Suppl.: 7-16
Correspondence: Amitabh Prakash, Adis International Limited, 41 Centorian Drive, Private Bag 65901, Mairangi Bay,
Auckland 10, New Zealand. E-mail: demail@adis.co.nz
Drugs 1998 Sep; 56 (3)