Title : Isolated duodenal metastasis of hepatocellular carcinoma
advertisement

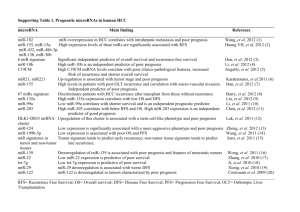
Title : Isolated duodenal metastasis of hepatocellular carcinoma- a rare presentation Abstract: Hematogenous metastasis to the duodenum from any primary tumor is rare. Hepatocellular carcinoma[HCC] frequently metastasizes to lung and regional lymph nodes. Involvement of small intestines by HCC is mostly via direct invasion of the contiguous neoplasm. We report a case of isolated non contiguous duodenal metastasis of hepatocellular carcinoma because of its rarity. Introduction: Hepatocellular carcinoma is the most common primary tumor of the liver. Metastasis is frequent in these aggressive tumors and is commonly to the lungs, regional lymph nodes and or bones. Involvement of small intestine is generally by direct invasion and spread. Isolated non contiguous metastatic involvement of the duodenum is very rare. Case report: A 52 year old male presented to the out patient department with icterus, pallor, pedal edema, abdominal distension, hepatomegaly upto 8cm below the costal margin and splenomegaly. He had been a chronic alcoholic and smoker for the past 15 years. Laboratory investigations revealed a raised bilirubin level [3.15mg/dl] and SGOT level[89U/l]. His viral markers were negative. Alfa feto protein[AFP] level was high[ 5225.9ng/ml, normal value being<20ng/ml]. Ultrasound abdomen done showed cirrhosis of liver with portal vein thrombosis, ascites and splenomeagaly. Upper gastrointestinal endoscopy revealed grade I oesophageal varices with an ulcer at D1D2 junction. Biopsy from the duodenal ulcer showed small intestinal mucosa with sub mucosal collection of tumour cells arranged in a sinusoidal pattern. The tumor cells were large with abundant granular eosinophilic cytoplasm with vesicular mildly pleomorphic nuclei .[Fig.1,2,3]. There was no evidence of mitosis or necrosis. The overlying small intestinal mucosa was ulcerated and the adjacent mucosa was free of dysplasia or carcinoma. The differential diagnosis considered by H&E features were, Neuroendocrine tumors (Carcinoid) and metastatic HCC. By immunohistochemistry the sinusoidal pattern was highlighted by CD34 [fig.4]. Stains for S100,synaptophysin and chromogranin were negative. Histopathological and immunohistochemical features with the markedly elevated levels of AFP in a cirrhotic patient were in favour of duodenal metastasis of hepatocellular carcinoma. Further radiological investigation was suggested. A contrast enhancing computer tomography[CECT] abdomen showed multiple hypodense lesions in both lobes of liver showing enhancement in arterial phase with early washout in the venous phase[fig.5]. The portal vein was dilated at the hilum and showed echogenic thrombus within. There was mild splenomegaly, moderate ascites and multiple splenorenal, perigastric and gall bladder collaterals. The radiological features were that of multicentric hepatocellular carcinoma. There was no direct invasion of the small intestine by the lesion. No other primary lesion was identified on thorough endoscopic and radiological investigations. Since the patient had portal vein thrombosis chemoembolisation was not recommended and the patient was put on palliative chemotherapy with cisplatin and 5 fluorouracil. He responded to the treatment and the first follow up radiological investigation showed reduction in the size of hepatic lesions. Discussion: Hematogenous metastasis to the duodenum from any primary malignancy is rare. The usual primary tumours include carcinoma of the lung, breast and malignant melanoma.[1-3] However most of these cases had metastatic deposits in other sites also. Hepatocellular carcinoma is the most common primary tumor of the liver worldwide. This aggressive neoplasm frequently metastasizes to lungs and regional lymphnodes. Involvement of the small intestine is usually by direct invasion and spread by the primary tumour.[4-8] Hematogenous or lymphatic metastasis is very rare. Even among those rare instances of isolated metastatic lesions of duodenum the primary origin from liver appears to be exceedingly rare. [9] With the histopathological picture of sub mucosal collection of tumor cells in nests, a differential diagnosis of carcinoid tumor was considered. The immunohistochemical markers for the neuroendocrine neoplasm, namely synaptophysin, chromogranin and S100 were negative. The sinusoidal pattern highlighted by CD34 by immunohistochemistry, raised AFP levels and radiological picture of hepatic lesions in a cirrhotic back ground favors the diagnosis of duodenal metastasis of hepatocellular carcinoma. With no involvement of other organs by radiological study this is a unique presentation of HCC with isolated non contiguous duodenal metastasis. Involvement of the duodenum indicates advanced nature of the disease with a very grave prognosis. Conclusion: Isolated non contiguous duodenal metastasis of HCC is rare and an unique presentation. This condition poses differential diagnostic problems and should be kept in mind. Close clinical and radiological correlation is very essential for the correct diagnosis of this rare presentation. References: 1. Bender GN, Maglinte DD, McLarney JH, Rex D, Kelvin FM. Malignant melanoma: patterns of metastasis to the small bowel, reliability of imaging studies, and clinical relevance.Am J Gastroenterol 2001; 96(8):2392-00. 2. Hashimoto M, Miura Y, Matsuda M, Watanabe G.Concomitant duodenal and pancreatic metastases from renal cell carcinoma. Surg Today 2001; 31(2):180-83. 3. Houghton AD, Pheils P. Isolated duodenal metastasis from breast carcinoma. Eur J Surg Oncol 1987;13(4):367-69. 4. Chen LT, Chen CY, Jan CM, Wang WM, Lan TS, Hsieh MY et al: Gastrointestinal tract involvement in hepatocellular carcinoma: clinical, radiological and endoscopic studies. Endoscopy 1990, 22(3):11823. 5. Del Natale M, Druez P, Brenard R: Images in hepatology. Fistulization of a hepatocellular carcinoma into the duodenum. J Hepatol 2001; 34(1):172. 6. Hatano E, Ikai I, Shimizu M, Maetani Y, Konda Y, Chiba T et al : Resection for hepatocellular carcinoma with duodenal invasion: Hepatogastroenterology 2003; 50(52):1034-36. 7. Lin CP, Cheng JS, Lai KH, Lo GH, Hsu PI, Chan HH et al. Gastrointestinal metastasis in hepatocellular carcinoma: radiological and endoscopic studies of 11 cases. J Gastroenterol Hepatol 2000;15(5):53641. 8. Mohamed AO, Joshi S, Czechowski J, Branicki F. Hepatocellular carcinoma directly invading the duodenum. Saudi Medical Journal 2005; 26(3):478-80. 9. Caroline Chung, Jaber Al Ali, David A Owen, Alan A Weiss, Eric M Yoshida,Isabella T Tai. A rare case of isolated duodenal metastases from hepatocellular carcinoma associated with p53 and ki-67 expression. Cases Journal 2009; 2:9344. Legends: Figure1: Figure1: Shows small intestinal mucosa with sub mucosal collection of tumour cells. H&E x100 Figure 2: Figure2: Tumour cells arranged in a sinusoidal pattern H&Ex100 Figure 3: Figure3:Tumour cells have abundant granular eosinophilic cytoplasm and vesicular mildly pleomorphic nuclei .H&E x400 Figure 4: Figure4: IHC for CD34 highlights the sinusoidal pattern IHC x100 Figure 5: Figure 5: CECT Abdomen shows multiple hypodense lesions in both lobes of liver