Immunotherapy Consent Form
advertisement

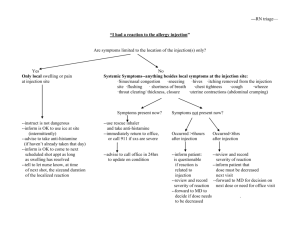
TO PATIENTS RECEIVING DESENSITIZATION INJECTIONS IN OUR OFFICE The following guidelines are very important for the safe and effective administration of allergy desensitization treatment and should be followed carefully: 1. Any injection can cause a reaction of (increased) wheezing, hives, nasal congestion, runny nose, vomiting or significantly increased shortness of breath. If this occurs as a result of an allergy injection, it will generally occur within two hours of the injection. If one of these reactions occurs, or if you feel that you have become ill as a result of an allergy injection, you must contact one of our doctors immediately. This can be done by calling any one of our offices or our home. In addition, if this occurs, you must see one of the doctors before your next injection. 2. Any injection can cause a reaction of redness or swelling or pain on your arm where you receive the injection. If this occurs the day of the injection, it is a normal reaction. If it lasts until the day after the injection, this should be reported to one of the nurses prior to your next injection. 3. TO PATIENTS WITH HIGH BLOOD PRESSURE, GLAUCOMA OR HEADACHE: Please notify our office if your primary care physician gives you a drug called a beta blocker for control of your high blood pressure, glaucoma or headache. 4. IF YOU HAVE BEEN STARTED ON ANY NEW MEDICINE/DRUG SINCE YOUR LAST VISIT, PLEASE INFORM THE NURSE OR DOCTOR BEFORE YOUR INJECTION. 5. If you are feeling well, you may receive your injections without waiting to see the doctor. However, we would like to have you see a doctor each time you start new vials. 6. If you are having any symptoms or are sick, please schedule an appointment to see your doctor before receiving an injection. 7. To expedite your visit, please schedule with the receptionist the day you wish to come in for injection or to see the doctor. 8. You should wait in our office for 20 – 30 minutes after each injection in case there is a reaction to an injection. 9. Optimum therapeutic results usually require three to five years of desensitization therapy. Discontinuation of therapy earlier than this may result in a higher increase of recurrence. 10. TO ALL OF OUR FEMALE PATIENTS: Not all drugs used in treatment of allergic diseases have been cleared for use during pregnancy. If you are planning on becoming pregnant, or are pregnant, please discuss drug use with one of our physicians. 11. Desensitization therapy generally takes at least 6-12 months before any benefit is noted. Improvement thereafter may be gradual. 12. If you have any questions regarding your injections, these instructions, or your allergy symptoms, please call our office at any time and speak with one of the doctors. There are 24 hour answering services on all office and home telephones, and a physician is available 24 hours a day for consultation. 13. Please inform your primary physician of allergy medication you are taking, so proper prescribing can occur. GENERAL RELEASE Patient’s Name: I have requested that allergy injections prescribed and/or provided by (the name of your office) be administered by someone other than employees of the allergy office. I acknowledge that I have been advised by the allergy office that the injection of the allergy extract should be performed by a qualified person and not by the patient, or the parent of the patient. I have in turn advised the agents of the allergy office that a duly licensed individual will give the injections. I understand that because of the above, the allergy office, its agents, successors and assigns, and all other persons, firms and corporations involved in the manufacture and prescription of the extract, cannot assume responsibility for the administration of the extract, and any resulting consequences. Therefore, on behalf of myself, my heirs, executors, administrators and assigns, as well as any minor children for which I am acting as parent and/or guardian, I hereby demise, release and forever discharge (the name of your office) and its agents, successors and assigns of whatsoever kind of nature, arising from and by reason of any and all known and unknown, foreseen and unforeseen bodily and personal injuries, and the consequences thereof, resulting and to result from the administration of said allergy extracts. I acknowledge that the person who will be requested to administer and inject the extract will be advised of this release. I understand that the new policy (the name of your office) advised against this and I have decided to waive that warning and continue home administration. I understand that the position statement of the AAAAI strongly recommends against home administration of allergen immunotherapy and I understand there have been deaths reported in association with allergen immunotherapy. Patient Signature Address City, State, & Zip Date Parent Signature (for minor) Date