Anaphylaxis following immunization
advertisement

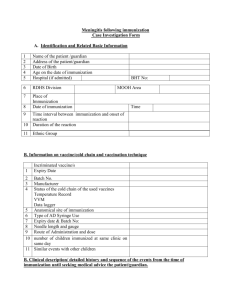
Anaphylaxis following immunization Case Investigation Form A. Identification and Related Basic Information 1 2 3 4 5 Name of the patient /guardian Address of the patient/guardian Date of Birth Age on the date of immunization Hospital (if admitted) 6 RDHS Division 7 Place of Immunization Date of immunization 8 9 BHT No: MOOH Area 10 Time interval between immunization and onset of reaction Duration of the reaction 11 Ethnic Group Time B. Information on vaccine/cold chain and vaccination technique Incriminated vaccine/s 1 2 3 4 Expiry Date Batch No. Manufacturer Status of the cold chain of the used vaccines Temperature Record VVM Data logger 5 Anatomical site of immunization 6 Type of AD Syringe Use 7 Expiry date & Batch No: 8 Needle length and gauge 9 Route of Administration and dose 10 number of mothers immunized at same clinic on same day 11 Similar events with other mothers B. Clinical description/ detailed history and sequence of the events from the time of immunization until seeking medical advice the patient/guardian. C. Clinical description/ sequelae of the event as per medical records/by clinicians Presence or absence of key anaphylaxis clinical features/laboratory findings Key Clinical Feature Yes/ No 1 Presence of features of cardiovascular signs/ symptoms a. Hypotension b. Tachycardia c. Features of Poor peripheral perfusionprolong capillary refilling time>3 sec d. Decreased level of consciousness/loss of consciousness 2 Presence of respiratory symptoms a. Bilateral wheezing b. Shortness of breath c. Stridor d. Upper airway swelling (lip, tongue, throat, uvula, larynx) e. Respiratory distress (tachypnoea, use of accessory muscles, recessions, cyanosis, grunting) f. Persistent dry cough g. Hoarse voice Remarks h. Sneezing/ rhinorrhea 3 4 5 Presence of dermatological/ mucosal features a. Generalized urticaria / erythema b. Angioedema c. Generalized pruritus with skin rash d. Generalized prickle sensation e. Injection site urticaria f. Red and itchy eyes Presence of gastrointestinal symptoms a. Diarrhea b. Abdominal pain c. Nausea d. Vomiting Laboratory findings a. Serum beta tryptase assay D. Concurrent Sings, Symptoms and Diseases 1 2 3 4 5 Concurrent Sing, Symptom and Disease Ictal or postictal state Fever Any symptoms of concurrent infection Concurrent /Long term medication Intoxication E. Clinical Examination findings: 1 2 3 4 5 6 General examination Cardiovascular System BP Pulse Volume Highest Heart Rate Respiratory system Highest Respiratory Rate Recorded Abdomen Central Nervous system Pulse Oximeter ? Yes/ No Remarks/Description F. Investigations 1. Random Blood Sugar2. CXR 3. Any other investigations G. Management a. Immediate resuscitation b. Subsequent Management H. Diagnosis on discharge/outcome of the patient I. Detailed history of this pregnancy (if applicable) /Any identified risk factors J. Past Obstetric History K. Past medical problems of the mother (if applicable) a. History of bronchial asthma/ allergic rhinitis/ eczema b. Allergic History (foods, drugs) c. Any other significant medical problems/previous hospitalizations L. Any adverse events noted following previous immunization with same vaccine/ or different vaccines M. Family history of similar events ………………………………………………………………………………….. Name , Designation, Signature of the investigator and Date of Investigation