to the Health Data Form
advertisement

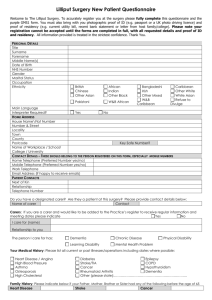
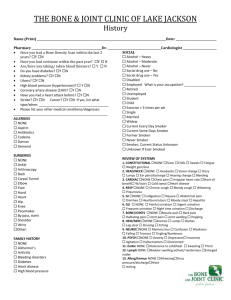
Monkspath Surgery Health Data Form The purpose of this form is to establish as much information about each patient as possible. This is important because it can be several weeks before medical records are received from your previous doctor. The information will be recorded on computer. You may ask to see the information held on screen about you at any time. The practice is registered under the Data Protection Act. All information will be strictly confidential. Please complete a form for each member of the family registering with the practice. If you have questions, a member of the reception staff will be happy to help. If you are taking any regular medication, please make an appointment with one of the doctors to discuss this. Electronic transmission of prescriptions - If you have nominated a pharmacy at your previous practice, please remember to update this nomination ASAP. If you wish to have your prescriptions sent electronically to a participating pharmacy, please collect a form from reception or your chosen pharmacy. Registration Details Surname: Title : Mr / Mrs / Ms / Miss First Names: Date of Birth: Address: Home Tel no: Work Tel No: Mobile: Email address: Sex: Male / Female Blood Group: Please state any allergies (medicines, food, animals etc) : Are you a carer or being cared for? If you are a carer of a patient of this practice, please indicate the name and address of the patient: If you are being cared for, please give the name and contact number of your carer: If you are a carer (whether of a patient at this practice, or elsewhere) and would like to discuss your situation and consider the involvement of other agencies, please make an appointment to see a doctor. If you have a visual impairment, hearing loss or learning disability which you feel may affect your access to the services at the surgery please do let us know so we can record any relevant information about communicating with you on your records. ………………………………………………………………………………………………….. Medical History Please tick the box if you have suffered from any of the following: Diabetes? If so, do you use insulin? Yes / No Asthma? Angina? Heart Attack? Date: High blood pressure? Depression? Epilepsy? Hepatitis? Stomach Ulcer? Please tick if you have had the following: Hysterectomy? Date: Vasectomy? Date: Family History Does anyone in your immediate family suffer from: Heart Disease ? Stroke ? YES / NO YES / NO High Blood Pressure? If yes, what is their relationship to you? If yes, what is their relationship to you? YES / NO If yes, what is their relationship to you Smoking Please circle Smoker / Non Smoker / Ex smoker If smoker, please state consumption. Number per day:…………… Cigarettes/ Cigars- please circle If ex smoker, please state date stopped smoking …………… Women Only (please answer those questions applicable to you) When did you last have a cervical smear ? What was the result? Where was the test carried out ? GP Surgery / Hospital / Clinic Please give details of any pregnancies, including miscarriages: Date Method of Delivery Details if child – sex / birth weight Children Only Please enter dates of the following immunisations: Immunisation Date given Date given Tetanus Diphtheria Pertussis Hib Polio Pneumococcal Meninigitis C MMR BCG Other – please indicate Date given Date given Signature of patient (or representative if under 16): Thank you for your help. Please return completed forms to the surgery. Date given