Orthopaedic Heath History Form
advertisement

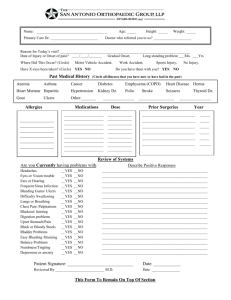
ORTHOPEDICS PATIENT HEALTH HISTORY In order for us to obtain a complete medical history, it is important for you to fill out this form as completely as possible. Please fill out every item. It is important for your doctor to know that you have carefully reviewed every area of this form. This information will be entered into the computer and you are welcomed to a copy of the report if you wish. Full Name _________________________________ Male Female Age_______ Date of Birth ________________ Height_______ Weight_______ Pharmacy Preference (include location) ________________________________________________ Primary Care Physician ____________________________ Referring Physician (if different)______________________________ (TAB 1) Are you taking ANY kind of medication now? (This includes prescription, over-the-counter or herbal medications) No Yes If yes, please list below include dosages. Dosage Medication Name (TAB 2) ARE YOU ALLERGIC TO ANY MEDICATIONS? Name of Medication No How often taken Yes If yes, please list below. Type of Reaction (TAB 3) Are you allergic to contrast dye? No Yes If yes, what reaction do you have?_______________________ Are you allergic to any non-medical things such as latex, tape, metal? No Yes latex tape metal (TAB 4) Have you ever been DIAGNOSED with any of the following problems? Cancer: bone breast lung lymphoma prostate multiple myeloma other______________ Heart and Blood Vessels: High / Elevated Cholesterol No Yes What year?_________ High Blood pressure Congestive Heart Failure Lungs and Respiratory: Asthma COPD/Emphysema Tuberculosis Stomach and Digestive: GERD Duodenal ulcer Hepatitis Stomach ulcer No No Yes What year?_________ Yes What year?_________ No No No Yes What year?_________ Yes What year?_________ Yes What year?_________ No No No No Yes What year?_________ Yes What year?_________ Yes What year?_________ Yes What year?_________ Kidney and Gender Problems: Renal failure No Are you pregnant? No Mental & Emotional: Depression No Anxiety No Glands, Hormones, and Sugar Control: Diabetes No Thyroid deficiency No Thyroid excess No Blood & Lymph Node problems: Anemia No Yes What year?_________ Yes What year?_________ Yes What year?_________ Yes What year?_________ Yes What year?_________ Yes What year?_________ Yes What year?_________ Yes What year?_________ Allergies, Immune & Infectious Problems: HIV No Yes What year?_________ Infectious mononucleosis No Yes What year?_________ (TAB 5) SURGERIES AND HOSPITALIZATIONS Have you had any surgeries? No Yes Please list any surgeries and when they were done ___________________________________________________________________ ____________________________________________________________________________________________________________ Have had problems with anesthesia (being numbed or put to sleep)? high fever trouble with intubation (placement of breathing tube PLEASE COMPLETE OTHER SIDE (TAB 8) FAMILY HISTORY Specific Anesthesia Problem Heart and Blood Vessels: Heart Disease High Blood Pressure Lungs and Respiratory: Asthma Lung Cancer Mother Father Brother Mother Mother Father Father Brother Brother Mother Mother Father Father Sister Brother Brother Sister Sister Brain and Nervous: Stroke Mother Father Glands, Hormones, and Sugar Control: Diabetes Mother Father Sister Sister Blood & Lymph Node problems: Bleeding/clotting problem Mother Other________________ Mother (TAB 9) SOCIAL HISTORY What is or was your occupation? __________________________________________ Have you ever used tobacco in any form? If yes, please complete the following: Type of Tobacco Cigarettes per day: ________ Other: (list type) __________ Are you currently using tobacco? Which is your dominant hand? Exercise level: None Living setting: Alone Assisted living No Yes No Sister Brother Sister Brother Brother Sister Sister Check here if you are retired. Do you consume alcohol? No Yes If yes, please complete the following: How Type of Alcohol Much How often Yes Right Left Regularly 1-2 times/wk Father Father Brother Neither is dominant (ambidextrous) Regularly 3 or more times/wk 20 mins Spouse Children other________________ Mother Father other_____________________ Nursing Home (TAB 10) REVIEW OF SYSTEMS: Have you recently had any of the following medical problems? CHECK yes or no and any of the following you have had. General Health Problems fever chills excessive fatigue Head, Face, Eye, Ear problems headache face pain blurred vision double vision hearing loss dizziness No weight loss Yes No Yes loss of vision ringing Stomach problems abdominal pain reflux diarrhea nausea Urninary problems recurrent infections pain with urination No difficulty urinating incontinence No Yes painful joints stiffness decreased motion Mouth & Throat problems change in voice snoring ulcers No sore throat Yes Bones, Joints and Muscles pain in back swelling of joints Neck problems neck masses or lumps No swollen glands Yes Brain or Nervous system problems change in alertness numbness seizures pain Heart or circulation problems No Yes chest pain irregular heartbeat heart murmur shortness of breath swelling of ankles blacking out or fainting leg cramps bluish discoloration of lips or fingernails Lung or respiratory problems chronic cough wheezing frequent upper respiratory infections No Yes No Yes heartburn vomiting No unsteady gait weakness Yes Yes Problems with Glands, Hormones No Yes heat or cold intolerance unwanted weight change excessive thirst or urination Problems with Blood or Lymph nodes No bleeds excessively after injury bruises easily anemia Yes