Understanding Lameness: A Summary of a
Lecture for Horse Owners
By Doug Thal, DVM
This article is a summary of a lecture that I gave to horse owners in Santa Fe last year.
I have always felt it important to make horse owners more aware of lameness and its
diagnosis. Lameness accounts for the greatest losses for the equine industry - hundreds of
millions of dollars annually. Lameness affects individual horses of all kinds and at all
levels, from subtle reduced performance to complete loss of use or euthanasia. Sadly,
many horses are asked to perform when they are in pain because of rider failure to
recognize lameness.
Understanding lameness basics (and working with an equine veterinarian with experience
in lameness) helps a horse person to:
Purchase horses (using a veterinary pre-purchase exam) who do not have current
lameness and are of a conformation less likely to become lame.
Recognize conformational predispositions in their horses and manage for
treatment and prevention of lameness.
Recognize or at least suspect when lameness is the root cause of your horse’s poor
performance (versus training issues), and get the lameness problems diagnosed
and treated.
Breed better horses. Understanding lameness and basic form and function allows
breeders to breed horses that are of superior conformation and thus less likely to
become lame.
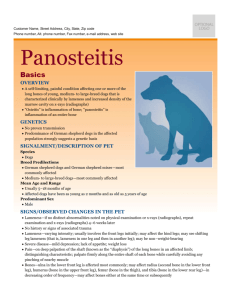
Some important points about lameness that every horse owner should know:
Lameness can result from pain coming from any component of the limb which
contains nerve endings. This means that skin wounds, connective tissue bruising,
muscle pain, arthritis (joint inflammation), tendon sheath and bursal
inflammation, tendon and ligament injury, and injuries to bone all can cause
lameness. The important point here is that what is causing the pain cannot
necessarily be distinguished based on the appearance of the lameness.
Horses of certain types and uses have specific lameness problems more
frequently. An example is arthritis in the knee (carpus) in race horses or hock
arthritis in cutting horses.
Forelimb lameness is easier for most people to recognize than hind limb
lameness. The mechanics of the forelimb means that lameness is more consistent
in appearance and more obvious to the untrained eye. Hind limb lameness is
generally more difficult to visualize and diagnose (this is especially true of subtle
upper limb problems). The massive musculature of the upper hind limb makes it
much more difficult to see and feel deeper structures in this region and very
difficult to image these structures using x-ray and ultrasound.
A high percentage of lameness is below the level of the fetlock and frequently in
the foot. Upper limb forelimb lameness is not common in adult horses. Upper
limb lameness is more common in younger horses because developmental
orthopedic disease (osteochondrosis, epiphysitis) is relatively common in these
sites in young horses.
Conformation correlates directly with function of the limb and is closely related to
the development of lameness. Horses with poor conformation are more likely to
experience problems with joints, tendons and ligaments than are horses of
“normal” conformation. An example is angular limb like “pigeon toe”(toe-in at or
below the fetlock level), for example, which cause a horse to paddle when it
moves and sets it up for uneven mechanical forces in the limb which over time
can lead to damage of joints and arthritis.
The lameness exam
The lameness exam is a detailed and methodical veterinary exam which allows the
localization of lameness. As a horse owner it is important to understand the importance of
this exam, and to understand the basis for it. The exam consists of a careful history, a
standing exam, an exam in movement, flexion and hoof tester exams, diagnostic
anesthesia (nerve blocks) and imaging (examples are x-ray, ultrasound, MRI). The
lameness exam is as much an art as it is a science. The diagnosis comes out of a synthesis
of findings from all of the above parts of the lameness exam. The exam is based on an
understanding of anatomy, and requires experience and a methodical approach to perform
well.
The first part of a thorough lameness evaluation is a thorough history of both the horse
and the injury. Examples of information gathered about the horse are breed, age, and
prior use. The history of the injury would include the date that lameness was first noticed,
how severe the lameness has been, and how the
injury occurred if this is known. All of these are
important questions which veterinarians ask and
horse owners should be try to provide accurate
answers to.
Examination is done first at a distance to evaluate
conformation and general appearance. More careful
examination and palpation of specific structures for
swelling, heat, pain, follows.
The next part of the exam is to see the horse in movement. Lameness is mostly
evaluated at the trot. Most thorough lameness exams are performed on firm to hard, even
footing. Examination often includes circles to both directions and may include inclines or
specific patterns. For the diagnosis of some types of lameness problems, having a rider up
can be advantageous.
Flexion exams are an important part of
lameness evaluation. Flexion exams
involve putting specific joints or regions
of the limb under stress for a specified
time. The horse’s degree of lameness is
assessed before and after flexion. The
results (change of degree of lameness
following flexion) give additional
information regarding areas of pain. As with
many parts of the exam, flexion tests must be interpreted in light
of what is normal for that specific horse.
Hoof testing involves the use of a pincer-like tool to put pressure
on specific regions of the foot in search of a pain response. As
with flexion exams, the key to smart interpretation of hoof tester
examination is knowledge of what constitutes a normal response.
This can only be gained through a methodical approach and lots
of experience with different types of horses.
At this point in the exam, we should know which limb is the
lame one, and we may or may not have a hunch as to where in
the limb the problem is. If the examiner is not certain of where the problem is, then nerve
blocks are performed to try to isolate the area of lameness.
Nerve blocks are used to methodically numb portions of the limb. Also known as
diagnostic anesthesia, “blocking” is injection of a local anesthetic agent around specific
nerves or into specific joints or other structures. The horse is evaluated before the block,
the area in question is numbed, and the horse is asked again to trot off. Either there is
improvement in the lameness or not. If there is not, the process is continued on specific
nerves progressing up the limb until the lameness is visibly lessened. Specific joints and
tendon sheaths can be blocked for a more specific localization of lameness. Blocks into a
joint or tendon sheath require surgical cleanliness to prevent infection of these structures.
Only once we have found the region from which the pain is coming
from do we use diagnostic imaging to describe the structures in that
area. This includes x-ray (radiology) to image bone, ultrasound to
image soft tissues, and may include less familiar technologies like
MRI, CAT Scan, and nuclear scintigraphy (bone scan).
X-ray is the first line of imaging for bone. It is less useful for
soft tissues. X-ray is often performed in the field with
portable equipment. More difficult studies can often be
performed better in a clinic setting. Digital x-ray is new
technology which does not rely on film. It is quickly
becoming the standard for equine x-ray.
Ultrasound utilizes sound waves traveling through tissues
to image those tissues. It is excellent for imaging soft
tissues, but cannot penetrate healthy bone. It is used
commonly to image tendons, ligaments, the surfaces of
bone, and other soft tissues.
All of the above pieces, when they are performed properly, and
assembled and interpreted correctly, provide an accurate diagnosis. Until we have an
accurate diagnosis there is no way to know what the treatment and prognosis of the
problem will be.
The future of the lameness exam is based on advances in imaging and more
technologically advanced treatments, but the cornerstone is a knowledgeable veterinarian
and a thorough exam.
MRI is being used more commonly in equine lameness diagnosis and is changing
our understanding of lameness of the lower limb. MRI allows both soft tissue and
bone to be examined in great detail. In some cases, the detailed information
coming from MRI can allow more targeted treatment and a better understanding
of the prognosis for return to use.
Other improvements in imaging include digital x-ray and ultrasound, nuclear
scintigraphy (bone scan) and CT scan.
Advanced treatment options are becoming more available and may provide better
solutions for certain lameness problems. Examples of these newer treatments are
shock wave and stem cell treatment.
Conclusion
Horse owners should establish a relationship with their equine veterinarian and
use him or her to help clarify lameness questions.
An educated horse owner should understand basic equine anatomy and the basic
concepts of the lameness exam.
Always call sooner on a suspected lameness problem rather than waiting.
Be careful of inaccurate lameness information on the internet. Use your equine
vet to help screen this information for you.
Be careful of the supplement game. There are hundreds of products out there that
make a variety of claims for solving lameness problems. These products are
expensive and in many cases have no proof of effectiveness. There is no
regulation on these products and so it is up to the consumer to beware. In my
opinion, money is generally better spent on a lameness exam and the search for a
correct diagnosis.
New technology like MRI will add knowledge to the field but is no substitute for
a good exam. A thorough, methodical clinical exam will always be the
cornerstone of lameness diagnosis. Be prepared to haul your horse to a clinic for
the diagnosis of complex lameness problems. For many reasons, these exams are
better performed in a clinic setting.
 0
0