July - October 2002 - World Health Organization

Office for the Coordination of
Humanitarian Affairs
World Health Organisation
Assessment on Emergency Preparedness in
Disaster Situations
Integrated Approach on Nationwide Preparedness
Capacities and Capabilities within the Republic of
Indonesia
July – October 2002
Assessment Report
Dr. Jose M. Echevarria, WHO
Pierre Bessuges, OCHA
Prof. Dr. Bastaman Basuki, WHO
Jakarta
October 2002
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
Thank You to…
Warm thanks to the staff of WHO, OCHA and other UN agencies in Jakarta and in the field
(Ternate, Aceh, and Kupang). You have all contributed to make this assessment possible and you have been kind and helpful in the whole process.
Thank you to all health partners in the Ministry of Health in Jakarta and in the Provincial and
District Health Offices that we have visited (Namroe Aceh Darussalam, Bengkulu, Nusa
Tenggara Timur, North Maluku, North Sumatra and South Kalimantan) your collaboration and information have been crucial to the success of our mission.
Thank you also to all other key persons and friends who were willing to meet us, and patient to respond our questions, your contribution has also been essential for our job.
Last, but not the least, we hope and wish that our recommendations would drive the emergency preparedness in Indonesia to a substantial improvement, and consequently to a more efficient and effective response in next emergencies.
…from the Assessment on Emergency Preparedness Team.
All comments, feedback and opinions are very welcome.
Dr. Jose M. Echevarria
Pierre Bessuges jotaeche@hotmail.com
Prof. Dr. Bastaman Basuki, bbasuki@bit.net.id
pbessuges@wanadoo.fr
22/09/02
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
Executive Summary
1. Disasters and Risks
Geographically, Indonesia lies in a potential area for natural disaster as well as man made disasters due to pluralistic and heterogeneous characteristics, such as political, economic, social and cultural aspects.
All through the last 10 years more than 10,000 people were reported killed and more than 6 million were reported affected due to natural disasters in Indonesia.
Man made disasters have resulted in a significant number of people forced into displacement (IDPs). From 1999 to date, internal conflicts have provoked more than 2 million IDPs. Today approximately 1,2 million IDPs are still remaining in Indonesia.
2. Background and Objectives
Given the above context, WHO and OCHA made the decision to undertake an independent nation-wide assessment on the state of emergency preparedness (AEP) in the country.
Although the focus of the assessment is on the health sector, other sectors, essential for emergency management, are assessed to illustrate an overall picture on emergency preparedness.
Based on collected data and analysis on the findings, AEP aims to suggest recommendations to the Government of Indonesia, donor’s community and UN agencies to strengthen collaboration and improve effectiveness in the management of the emergencies.
3. Main Findings
o There are notable good will and efforts in the Government to build or reinforce their capacity and capability on emergency management (preparedness, readiness, response and rehabilitation). However, the coordination mechanisms among the public sectors are poor at all levels due to ad hoc and informal meetings, poor transfer of information and knowledge, and lack of sensitivity on preparedness, compared to response. o The multiple efforts and activities, undertaken by the UN agencies on the emergency management topic, seem to suffer from the same challenges in coordination mechanisms and information flows as the government public sectors.
o In 2000, the Ministry of Health established the Health Affairs Crisis Center (PPMK), which has the role of coordinating emergency preparedness. The PPMK yearly budget as well as its number of qualified staff is clearly insufficient to properly accomplish the tasks and fulfil the responsibilities mentioned in its mandate.
o Community awareness on emergency management, comes from spontaneous knowledge acquired from the lived experiences rather than from an official/technical way.
The communities and their leaders are rarely involved in emergency preparedness or management. o Numerous trainings on emergency management have taken place throughout the country. However, the criteria for the selection of trainees and the high staff turnover do not allow sustainable and consistent conditions for benefiting from the emergency preparedness trainings. o The central government allocates funds from the national budget for routine and overall emergency matters, but most of these funds are used for response rather than for preparedness.
22/09/02
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
4. Recommendations
o The central disasters coordination body, BAKORNAS, does not have implementation or policy-making functions, its role and responsibilities must be assumed effectively by all ministries and other members in the Coordination Board. o The UN humanitarian leadership and coordination mechanisms must be reinforced in order to present a proper model for the Government to improve its emergency preparedness capacity and efficiency. o The international donor community must strengthen the sustainability of emergency preparedness projects by supporting more effective projects (horizontal programmes) than efficient ones (vertical programmes). o National and international institutions must coordinate emergency management activities and humanitarian assistance at central and decentralized levels. o The level of knowledge in emergency management must be improved and the level of professionalism in emergency preparedness must be enhanced. Communities must be involved in emergency preparedness and management. o WHO must establish a emergency management post to support the PPMK to accomplish its essential tasks o OCHA must reinforce its role as the leading trigger to facilitate the collaboration and coordination with the government, UN and other humanitarian actors.
“If disaster is defined as failure to cope with an emergency, then the aim of preparedness programmes is (1) to lengthen the period between disasters and (2) to reduce the impact of emergencies/disasters when they do occur.”
22/09/02
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
Table of Content
E NTRY POINT 1: E MERGENCY P REPAREDNESS C OORDINATION M ECHANISMS
C OORDINATION , O PERATING C ONDITIONS AND D ISTRIBUTION OF R OLES
O FFICIAL / L EGAL G UIDING D OCUMENTS
D ECISION MAKING P ROCESSES , L EADERSHIP AND C HAIN OF C OMMAND
E NTRY POINT 2: F INANCIAL M ECHANISMS
R ESOURCE M OBILISATION S OURCES
R ESOURCE M OBILISATION P ROCESSES
E NTRY POINT 3: L OGISTICS AND C OMMUNICATIONS
A CCESS /T RANSPORT /I NFRASTRUCTURE
P ROCUREMENT /P URCHASING /S TORAGE /D ISTRIBUTION (F OOD / NFI/D RUGS )
E NTRY POINT 4 : H EALTH S ECTOR
N ATIONAL H EALTH C RISIS M ANAGEMENT C ENTRE (PPMK)
H EALTH S TAFF AND F ACILITIES
E VACUATION /R ESETTLEMENT A REAS AND W ATER S OURCES
E NTRY POINT 5: I NFORMATION AND C APACITY B UILDING
E XAMPLES OF P OSITIVE F INDINGS DURING THE F IELD V ISITS
E MERGENCY P REPAREDNESS C OORDINATION M ECHANISMS
L OGISTICS AND C OMMUNICATIONS
I NFORMATION , C APACITY B UILDING AND T OOLS
22/09/02
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
1. Introduction
1.1.Indonesian Context
1.1.1.Geography and Demography
1
Indonesia is the largest archipelago in the world consisting of 5 large islands (Sumatra,
Kalimantan, Sulawesi, Java and Papua) and more than 17,000 smaller islands and islets
(40% inhabited) spanning 3,200 miles between the Indian Ocean and the Pacific Ocean with an area of 5,193,250 sq. km of which only 1,919,317 (39%) sq. km is land area.
Indonesia has two weather seasons closely related to the direction of the winds. Between
June and September the dry winds blowing from Australia cause the dry seasons and between December and March wet winds from Asia and the Pacific cause the rainy season in Indonesia.
The estimated total population of 209 millions (51,8% female) makes Indonesia the world’s fourth most populous country. Around 55% of the population is concentrated on the islands of Java and Bali, one of the most densely populated areas of the world. Close to 40% of the population lives in urban areas and 60% in rural ones. Overall, Indonesia comprises more than 300 ethnic groups speaking over 350 languages. Javanese gives rise to the countr y’s largest ethnic group, which forms 45% of the total population. Indonesia has the largest
Moslem population in the world with 87 % of its population nominally adherent. A Christian minority (9%) resides predominately on the outer islands. ( For additional information on
Political Structure and Administrative Division see Indonesian Country Emergency Profile in the website : http://www.who.int/disasters/ )
1.1.2.Disasters and Risks
Geographically, Indonesia lies in a potential area for natural disaster as well as man made disasters due to pluralistic and heterogeneous characteristics, such as political, economic, social and cultural aspects. In recent years, political, economic and social crises have led to complex
According the BMG in Indonesia
Since 15th July to 31st August 2002
74 earthquakes have been registered on average, 1,7 earthquake / day average magnitude 4,5 emergency situations. The economic and political crises in Indonesia as well as natural disasters have increased public health risks for the population of Indonesia.
Natural Disasters
Indonesia is located in an area of the world that experiences regular natural disasters, such as earthquakes, tsunamis, floods, severe droughts and volcanic eruptions. Since the
Indonesian archipelago forms a part of the Pacific Ring of Fire, it is prone to earthquakes
1 Based on the “ State of the World’s Children ”, UNICEF, 2001 and “
World Almanac and Book of Facts
”, 2001,
MacGeveran
22/09/02 1
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002 and volcanic eruptions. Since last year, the government has been putting 10 of its 129 active volcanoes on “alert” status.
Man made disasters including civil disturbances, communal violence and separatist guerrilla warfare has resulted in a large quantity of the persons forced into displacement (IDPs). At the same time, the Republic of Indonesia has been experiencing the economic backlash of the Asian financial crisis, while making a transition to democracy and initiating a complex decentralization process.
Manmade Disasters’ Consequences
From 1999 to date, internal conflicts have provoked more than 2 million IDPs. Today approx. 1,2 million IDPs are still remaining.
Potential imbalance in population is expected due to the on-going arrival of
“illegal workers” (500.000 announced) from Malaysia.
In early September 1999, a large number of people
(estimated 300,000) fled East Timor for the safety of the western part of Timor, Nusa Tenggara Timur
(NTT) province. In July 2002 it was estimated that well over 50,000 still remain in NTT 2 .
From mid-January 1999, and November 1999
Maluku and North Maluku Provinces, respectively, experienced dramatic sectarian violence between
Moslem and Christian communities.
Civil Conflicts have displaced over a hundred thousand persons in provinces of Maluku,
North Maluku, Southeast and Central Sulawesi, Kalimantan, Aceh and Nusa Tenggara
Timur (West Timor). Tens of thousands of persons are displaced in nine other provinces.
The Indonesian National disaster Management Coordinating Board (BAKORNAS) estimated in May 2002 that there were about 1,250,000 IDPs in Indonesia.
Many emergency and disaster incidents has occurred in the last ten years, and they caused hundreds to thousands deaths, and hundreds of thousands people injured and more than one million people evacuated to 20 other provinces for safety reasons. The multidimensional crisis in Indonesia has made the situation more serious, due to the increase in psychosocial disturbances, and damage to the environment and infrastructure.
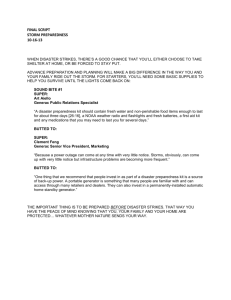
Evolution of Number of Victims of Natural Disasters in Indonesia over the last Two Decennials 3
Victims of Natural Disasters
In Indonesia
1982 – 1991 1992 –2001 Increase
People reported killed
People reported affected
4,290
2,000,000
10,500
6,900,000
+123%
+172 %
1.2. Assessment Rationale
Given the above context, WHO and OCHA have made the decision to undertake an independent nation-wide assessment on the state of emergency preparedness (AEP) in the country 4 .
Although the focus of the assessment is on the health sector, other sectors, essential for emergency management, are assessed to illustrate an overall picture on emergency preparedness and its policies and activities.
From the findings, the AEP Team make recommendations, especially to WHO but also to other UN agencies, for strategic actions to increase the capacity for and quality of disaster preparedness and management at the central, provincial, district and community levels.
The recommendations also are addressed to the government, non-government and donor partners, with whom WHO could collaborate in emergency preparedness strategies.
2 Based on IOM and WFP data, especially latest map on IDPs in Indonesia, May 2002.
3 Based on data in “ World Disasters Report 2002, Focus on Reducing Risk ”, International Federation of Red
Cross and Red Crescent Societies
4 See Annex 1 - AEP Terms of Reference
22/09/02 2
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
1.3.Objectives
To define a methodology and collect secondary and primary information in order to get an understanding of the state of emergency preparedness in the country at all central and decentralised levels.
To analyse the information in order to draw conclusions on the main current trends, constraints and good practices, regarding emergency preparedness aspects in the country.
To suggest recommendations to the Government of Indonesia, donor’s community and UN agencies to strengthen collaboration and improve effectiveness in the management of the emergencies.
1.4.Methodology
The AEP Team was composed of 3 members. In order to achieve these objectives, the AEP
Team has based its work on a specific methodology 5 . The AEP Team considered preparedness as:
“ The set of measures that ensure the organised mobilisation of personnel, funds, equipment and supplies within a safe environment for effective relief
”
6 .
P
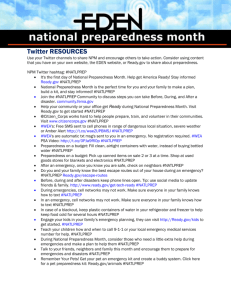
For data collection and analysis,
AEP Working Progress R
E the methodological sequence of the AEP are 1) a review of the
Te am
Brie fing
De
/Prep arat ion sk d ata
co llect ion dolo
Me tho gy defin itio n
Initi atio n w orks hop
Fie ld v isits
im
Fie ple me ld in nta format
An sis tion ion
co llect and
co
Draf ion ncl usi t rep ort ons
Fin al re port
S
E
N
T
A
T existing information, 2) interviews of key informants, 3) observations during of field sites visits and 4) conclusions and recommendations.
I
O
The assessment is primarily focused on the health sector
N
(public health issues, health facilities and resources). However, other sectors essential for emergency preparedness
(coordination and partnership collaboration, finance, communication and logistics, information and capacity building) are assessed to provide a picture of overall coherence of relevant policies and activities.
During an initial national workshop 7 , key-actors in the health sector were invited to Jakarta. The objective of the two day workshop was to identify national / provincial and district capacities in emergency preparedness facing natural and man-made disasters.
The core work of the AEP have come out of the visits to different areas across the Indonesian archipelago and the observation of the reality in the field and the collection of first hand information.
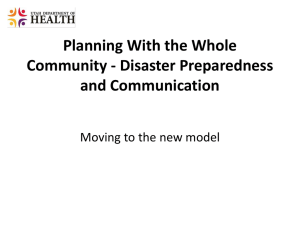
Indeed, the AEP Team made the choice to give the priority to primary information collection and analysis. The
AEP Team listed the relevant
Aceh
Bengkulu
Central Administration
• Ministry of Health
• Ministry of Social Welfare
• National Coordination
Body (Bakornas)
West Kalimantan
Jakarta
Central Java
Yogyakarta
Origin of Workshop
Participants
Central Sulawesi
Maluku
South Sulawesi
Irian Jaya
Nusa TenggaraTimur
5 See Annex 2
–Information Sheet AEP Methodology
6 See “WHO and Emergency Preparedness at Global Level”, Department of Emergency and Humanitarian Action,
WHO, September 2000
7 See Annex 3 - Workshop Report, and Annex 4 – AEP Base Questionnaire Form
22/09/02 3
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002 informants and institutions to constitute the AEP interview panels with which the AEP Team would meet at each level for each visit.
The collected information has been organised in a framework developed especially for the
AEP. Each site visit results in an
Information Sheet including the key elements characterising the site visited, the information collected and analysed. The information sheets are available is each AEP framework field reports 8 . The AEP report illustrates its findings and conclusions through basic indications for further studies and examples in order to develop common awareness on the importance and challenges of emergency preparedness.
The findings, conclusions and recommendations are presented in the AEP logical order. The AEP team has chosen to organise the consolidated information thematically, according to the AEP framework entrypoints (key points) from the AEP Framework Field Report , in order to reflect the dynamic, crosscutting and operational orientations of the AEP.
8 See Annex 5 AEP Field Reports
22/09/02 4
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
2. Findings
2.1.Entry-point 1: Emergency Preparedness Coordination Mechanisms
2.1.1. Structures
1966
Advisory Board for Natural Disasters
Management
(Emergency Relief for Disaster Victims)
1979
BAKORNAS PBA
Extended to Provincial ( SATKORLAK) and District Task Forces ( SATLAK)
Four Ministers, Chaired by Minister for
People Welfare
1990
BAKORNAS PB
Armed Forces included
1999
BAKORNAS PBP
Management of man-made disasters or social unrest, (IDPs issues) included.
Membership extended up to 13
Ministers and related Governors
National Government Body
In 1979, the National Natural Disaster Management
Coordinating Board 9 (BAKORNAS PBA) was established to replace Advisory Board for Natural
Disaster, directly responsible to the President and chaired by the Coordinating Minister for People Welfare.
Its membership comprises four ministers and 17 officials appointed by related ministers and heads of agencies.
On 2 nd September 1999, the Presidential Decree No.
106/1999 was issued to include the management of man-made disasters or social unrest and BAKORNAS
PBA became BAKORNAS PBP. In order to facilitate this additional scope to disaster coordination, the members were extended up to 13 Ministers and related
Governors. Since 2001 and the Presidential Decree No.
111/2001, BAKORNAS PBP is directly under the responsibility of the Vice-President of Indonesia. Since
2002, the structure of BAKORNAS Secretariat has been transformed to a permanent entity with 4 organisational units 10 .
Other National Bodies
Emergency preparedness issues are also part of the National Government agenda through other national bodies, such as the Central Planning Agency (BAPPENAS) producing the 5year National Plan (currently, 6 th Plan, 1999-2004), the Ministry of Transport, including the
Search and Rescue Unit (BASARNAS), other line Ministries which are members of
BAKORNAS PBP 10 .
Decentralised Bodies
At Provincial level, the inter-sectoral coordinating body is the SATKORLAK, which depends directly on the Province Government. The Head of Satkorlak is the vice-Governor, the
Deputy is Head of the Development and Unity Division (KESBANG / LINMAS). The
Secretary of Satkorlak is the Head of the Provincial Social Office (DINSOS). SATKORLAK members are all the heads of the Government Administrations, including the Armed Forces, the Police and local PMI (Indonesian Red Cross).
At District level, the inter-sectoral coordinating body is the SATLAK, which depends directly on the District Government. The Chairman of the SATLAK is the Bupati, and the members are representatives for various departments on the same model as the Provincial organisation.
2.1.2. Coordination, Operating Conditions and Distribution of Roles
Four types of coordination mechanisms exist within the UN system in Indonesia, which can constitute forums for emergency preparedness:
9 See Annex 6 - Information Sheet BAKORNAS
10 For further information, see “ Report on Final Evaluation on Strengthening Disaster Management in Indonesia”
UNDP, July 2002.
22/09/02 5
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
o Formal Coordination Meetings: a monthly meeting is held with the participation of UN agencies, NGOs and donors community. o The UNDMT is normally composed of all the UN Agencies. In Indonesia, the
UNDMT involves non-UN international actors in emergency and disaster management related activities. The UNDMT Indonesia closely works with
BAKORNAS PBP, its Secretariat and Indonesian Red Cross (PMI). When necessary, joint meetings may be conducted, in particular in emergency response situations. o The “Friends of BAKORNAS” group is an informal group, gathering various actors (UN, NGOs and BAKORNAS) interested in enhancing information sharing and implementation of activities related to emergency management 11 .
Specific supportive actions to the MoH and BAKORNAS on emergency management related issues. o The Ministry of Health has received bilateral technical assistance support from, amongst others, USAID, AUSAID, ADB, for disaster management capacity in the country. o WHO has been working with the MoH since 1998 on emergency management and more recently, with PPMK, especially on emergency preparedness. The UNDP is working directly with BAKORNAS in capacity building (Programme to be re-initiated in 2002), and other UN agencies, such as OCHA and UNHCR, have assisted the Government in an ad hoc way, in training and coordination of emergency response, rapid assessments, and contingency planning.
Coordination mechanisms depend on routine interdepartmental meetings, ad hoc meetings and informal / inter-personal relationships.
NTT
SATKORLAK and SATLAK coordination meetings usually occur once every 2 to 3 months. In case of emergency, the frequency of the coordination meeting increases and can be daily if necessary.
The informal channels to get information (friends, chance, rumours) can supersede the official ones.
The participants to these meetings may include specific institutions or representatives, such as the community leaders, in addition to the usual members of the SATKORLAK and SATLAK. This depends on the agenda and the type of disaster / impact in the area.
The health officers and SATKORLAK representatives consider that there is a good coordination among the various members, as well as between the health office and social affairs, public work and transmigration departments. However, on a general basis, there is a lack of coordination between sectors and
North Maluku horizontal institutions based upon insufficient crossing/sharing/feed backing information systems.
However, SATGAS (Taskforces) can be part of the
SATKORLAK and SATLAK organisation charts (e.g.
NTT) or separate (e.g. North Maluku). There can be a
In 2000, DINKES North
Maluku District established its own health emergency taskforce ( SATGAS PBPP ) for IDPs and Disasters. strong discrepancy between SATKORLAK and SATLAK coordination mechanisms and sector coordination SATGAS (taskforces). This can create an environment of competition and difficulties resulting from the overlap of leadership (coordinating bodies / sector leadership).
Given the recent and rapid decentralisation and the on-going division of Provinces and Districts, offices premises and equipment are not always available for
11 See Annex 7: Friends of Bakornas Activities Matrix
22/09/02 6
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
STAKORLAK and SATLAK organisations. In some cases, the coordinating bodies are hosted in the premises of local government offices.
Monitoring mechanisms are too weak to properly support sustainable coordination mechanisms.
Where SATKORLAK and SATLAK are in charge of the official coordination, specific responsibilities are given to their members such as health/medical and water/sanitation assistance to Health Departments (DINKES), food control and distribution to Social Departments (DINSOS), transport to Public Works Offices (PU) and evacuation, shelter and security to the Armed Forces (TNI) and the Police.
2.1.3. Official / Legal Guiding Documents
BAKORNAS has edited general guidelines on emergency management that have to be adapted and agreed upon at all decentralised
Aceh levels. The level of adaptation and ownership of the guidelines by the various decentralised administrations and stakeholders vary from one
Province or District to another (from non existing to
In June 2001, a 2-day workshop was organised by
Bakornas on Emergency
Contingency Planning. nearly adapted). BAKORNAS has the initiative to disseminate the information and emergency standard procedures.
Decrees and Policy Papers on emergencies management exist at national, provincial and district levels 12 , and the latest ones are under the Governor and the Bupati authorities. Memorandum of Understanding usually exist linking the members of
SATKORLAK and SATLAK, especially the Government Offices, Armed Forces and the Police.
In some case, Emergency Standard Operating Procedures already exist but they are not operational because they have not been adapted to the local context or disseminated. In some cases, the Standard Operational Procedures (SOPs) are more like guidelines since no specific action is identified by sector, and no detailed activities/responsibilities are specified. There is a tendency that good SOPs are prepared locally after disasters. However, due to the lack of resources, the implementation of the SOPs has not been sustainable. (i.e. Nusa Tenggara Timur
Province, Sikka District)
2.1.4. Decision-making Processes, Leadership and Chain of Command
The decisionmaking process depends on the “size” of the disaster. It starts with the responsibility of the Camat at Sub-District Level and the Bupati at District Level. If the disaster has a “Provincial” dimension, it falls into the responsibility of the Governor. A national disaster requires BAKORNAS coordination.
In some cases, direct support can be obtained from BAKORNAS even though the disaster does not have a national impact. In addition, no cases of bilateral cooperation in case of emergency or on emergency preparedness issues were reported between two neighbouring Provinces.
There is a strong correlation between the origin/background of the person in charge
(Governor, Bupati, Heads of Operational Units of the SATKORLAK and SATLAK) and the organisation of the coordination body. In other terms, a person with a military background will have a different impact on the structure, staff management, risk mapping and operating conditions of SATKORLAK and SATLAK than a person in charge with an agricultural background.
Political will is also very important since it requires a specific attention and targeted efforts to enhance the emergency preparedness. The lack of sensitivity on preparedness at the highest level affects the coordination mechanisms.
12 See legal reference documents among the documents consulted.
22/09/02 7
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
2.2. Entry-point 2: Financial Mechanisms
2.2.1. Resource Mobilisation Sources
The central government allocates funds on national budget (APBN) basis for routine and emergency matters. (Bakornas PBP, Ministry of Health, Ministry of Social
Welfares, Ministry of Public Works).
The MOH has a contingency budget, which can be released directly by the Ministry of
Health. The Ministry of Social Welfares provide funds for internally displaced people and other natural and man-made disasters victims. The Ministry of Public Works provides funds for related emergency infrastructures matters.
Provincial government (Governor office), District office (Bupati office), and Sub-district office (Camat office) allocate routine and emergency funds through decentralised budgets (APBD).
Unofficial funds are normally coming from the communities. In order to have more emergency funds, a province generate a mobilisation fund community through
Community response
Rapid local funding response comes from religious communities and/or from the
Zakat Fund. The
Zakat Fund is in the Moslem rules in spontaneous neighbourhood solidarity. accordance with which all the
Moslems have to give a proportion of their income for common or public purposes or needs. Personal and community voluntary basis for emergency matters in Indonesia with the spirit of “gotong royong” ” (Spontaneous community/ neighbourhood solidarity).
2.2.2. Resource Mobilisation Processes
In case of emergency, temporal and immediate funds can be released by the Camat or Bupati offices to cover immediate needs. If required, the Bupati or Governor offices can then reimburse these funds respectively. When emergency resources are released directly through Satkorlak or Satlak, the local governments can search for extra funds from other sources (e.g. Central level, external aid, etc.) to cover their expenses.
In case a district could not cover the cost of an emergency, the district has to conduct a rapid needs assessment and send a request to Central Government and PPMK.
PPMK will then forward it to the Secretary
General of MOH. Upon his approval, the Rapid Resources Mobilisation
Secretary General of MOH forwards it to the Minister of Health for releasing the contingency fund requested by the district.
Timing to release contingency funds to cope with an “urgent-emergency-scenario”, could need 4 days after a long and weighty bureaucratic path.
The time required for releasing the contingency funds depend on the completed need assessment and on who ask the contingency fund. In general, the process to release contingency funds can take at best about 34 days after the district’s request.
2.3. Entry-point 3: Logistics and Communications
NB : The information regarding logistics and communication cannot be obtained by interviewing people only, but requires the visits of different sites, the discussion with relevant experts, and the observation of physical areas. Therefore, the information gathered on this entry-point is relatively uneven and cannot be generalised.
2.3.1. Access/Transport/Infrastructure
The state of infrastructure (road, tracks, airstrips, harbours, railways) is not to be generalised because it was not specifically assessed. However, examples were seen that remote areas, accessible by road in the dry season, could be cut off when rains
22/09/02 8
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
flood the road (North Sumatra), and unsecured areas around sensitive industrial sites
(West Java).
Most of the places visited have sea access. However, the level of emergency preparedness of the seaports is irregular. The seaports are usually very crowded areas, and
North Maluku access/evacuation points are made of wooden peers.
In case of evacuation, TNI, Navy, Search and Rescue and Police transport means are mobilised. Personal
Dufa Dufa seaport, proximity to
Airport (North of Ternate
Island), is a good location for contingency evacuation plans. means such as wooden boats/barges are used when available among the families.
However, probably due to geography and the maritime tradition of the country, sealocated infrastructures and means are relatively in better state of preparedness compared to land-located infrastructure and means. For instance, the legislation regarding road building and maintenance is very scarce and the responsibilities are unclear and diluted between the various Ministries and the new decentralised authorities. The importance of the impact of deforestation and agriculture of subsistence is underestimated when emergency preparedness issues are mentioned.
Security (Aceh) and long procedures for official clearance (Maluku, NTT West Timor) can be a constraint for delivering emergency response, conducting a routine check and visiting facilities and institutions.
Usually, several combined means of transport are necessary to reach remote areas
(sea/road, train/road, air/sea/road). Some areas are inaccessible but by using helicopter or walking (Mountainous areas in Aceh or Papua Provinces). Some partnership arrangement can be made related to the emergency use of routine equipment (NGO boat, Foreign Private Company’s Helicopter, etc.).
The Armed Forces and the Police have considerable transportation and communication facilities due to their primary role in the past and until now. However, although BASARNAS has decentralised Search and Rescue Posts Facilities in 26
Provinces, no mention of this institution was made at central and decentralised level when the visits were implemented.
2.3.2.Procurement/Purchasing/Storage/Distribution (Food/ NFI/Drugs)
The nationwide BULOG-DOLOG-Sub-DOLOG system is responsible for the overall logistical management of food storage respectively at national-provincial-district.
Food distribution is organised and managed locally by the Provincial/District Social
Welfare offices (DINSOS).
For instance, the Province Government, through DINSOS can provide funds to
DOLOG to buy rice from the cooperatives (at market price) and redistribute it (at
1000 Rp per Kg) to the poorest families (20 Kg of rice / month), identified by the
Family Planning Office.
Medical equipment and drugs stocks are managed by the Health Authorities at
Central (DEPKES/PPMK), Provincial and District levels (DINKES), and health centres (PUSKESMAS). Routine stocks are constituted at each level. Due to physical storage and preservation conditions and due to the difference in population routine needs, the storage capacity varies from 3 month at District level to 12 months at
Central level. Additional drugs can be obtained from the MOH but the delivery and logistical mobilisation delays can be a constraint during the first moments of the emergency.
In proportion to the size of the country and the distances between different areas, there are relatively few warehouses, e.g. three DOLOG warehouses for the whole
North Maluku Province, all located on Ternate Island.
22/09/02 9
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
A system of airdrops of food/drugs is usually preferred to a warehouse-spread storage system and organised upon necessity. The local health officers consider that drug assistance (such as drugs, water purifier units) for emergency cases is easy and fast to deliver, therefore little stock as are constituted locally.
2.3.3.Communication Means
Mobile phone relays and connections are improving across the country, although still lacking in some cases, in crucial areas such airports (e.g. Ternate).
SSB radio coverage is good and widely used by military, civil and medical staff. SSB radio at all
NTT
A radio-based Early Warning System was developed in 1998, but since then the trained staffs have left and there is no plan to train new staff, due to lack of funds hospitals and health facilities are available. However, communication equipment, if available, is not functioning because of lack of staff and maintenance.
Examples of transfer of knowledge combined with transfer of technologies have been assessed. For instance, in North Maluku, the equipment used for the Emergency
Training will be given to SATLAK - 1 computer and to CAMAT - 12 walky-talky handsets.
2.4. Entry-point 4 : Health Sector
2.4.1. National Health Crisis Management Centre (PPMK)
Based on Ministry of Health Decree No 1277/2001, the Centre for Health Emergency
Response 13 (PPMK) is an agency directly under the responsibility of the MOH
Secretary General. The PPMK has tasks to develop general policy concept, to prepare implementing policy concept and to develop technical policy as well as coordinating in implementing, advocating, and controlling health crisis and health problem management.
The PPMK strategic plan p resents the rationale for the Centre’s approach to emergency management. The plan considers internal and external environmental analysis, vision and value statements, future assumptions, and critical limitations before proposing emergency management goals
I n November 2001, the Ministry of Health launched a pilot project for handling emergency health situations (IEH), to be implemented in 6 Provinces. and objectives for the Centre. While the various crises in Indonesia have compromised resources available to the
Centre, an ambitious capacity building
In September 2002, 3 heads of Province
Health Offices from the 6 pilot-provinces, did not know about IEH. program is planned for hazard mapping, global disaster information networking, community participation, and professional training.
2.4.2. Official Guiding Documents
Numerous useful and practical guidelines and health SOPs on EPR have been developed at the central level, these documents have not been accessible to all the structural levels including provinces, districts and sub-districts. Such information has not been shared hierarchically as well as horizontally across provinces, districts or sub-districts.
In another instance, in November 2001, the Ministry of Health launched a pilot project for handling emergency health situations (IEH), mainly focused on IDPs issues, to be implemented in 6 Provinces: Central Kalimantan, NTT, North Maluku, Maluku,
Central Sulawesi, East Java. However, some heads of the provincial health offices were not informed about the IEH Plan.
13 See Annex 10: PPMK Information
22/09/02 10
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
The most essential materials such as SOPs for Hospitals are not available in many of the provinces. Out of an approximate total number of 1800 hospitals in the country
(both public and private), maximum 30% have emergency plans but it is unknown when these emergency plans were reviewed, updated and/or practiced.
2.4.3. Health Staff and Facilities
Health staff (doctors and paramedical staff) and health facilities (hospitals, health centres and sub-health centres) seem to be quantitatively sufficient to cope with an emergency or disaster situation, depending on the importance of the disaster.
However, qualified health staff on emergency preparedness is frequently transferred to other provinces and often not replaced with those with the same quality of competence.
Some of the hospitals in the assessed provinces have not specific emergency equipment and among those that have it, the equipment is obsolete or out of order due to lack of maintenance.
2.4.4. Health Early Warning
In Indonesia, national and provincial health authorities have well-established epidemiological surveillance systems. While the provincial systems have varying degrees of analytic competence and reporting compliance, the building blocks of reporting forms and reporting requirements are widely disseminated among some provinces and some humanitarian actors. However, the Indonesian experience suggests much work remains ahead to streamline these normative tools for widespread applicability.
Surveillance activities are not well performed. Information is not complete in terms of places covered and the quality is not sufficient for useful early warning tools, which include data on main potential outbreak diseases and food shortage.
Surveillance data are not regularly reported punctually. Frequently, the monthly routine reports are delayed for a few weeks. It was also found some difficulties in collecting and reporting surveillance data since experienced staff is transferred frequently and newly arriving staff is not properly trained on surveillance.
2.4.5. Evacuation/Resettlement Areas and Water Sources
None of the levels (from central to sub-district) has formally identified temporary settlement and/or alternatives water and food sources for affected population in the case of emergency.
Usually open areas, public and religious buildings (Mosques, Churches, etc) are used as spontaneous shelters or areas of evacuation after a disaster. No alternative water sources or purifying/drinking water kits stocks have been identified or constituted.
2.5. Entry-point 5: Information and Capacity Building
2.5.1. Information flows
The problem of lack of information and poor transfer of knowledge is severe at all central and decentralised levels. As a result, the materials have not been utilised in the decentralised levels to develop their own guidelines, which reflect the regionspecific situation and accommodate the regional needs.
Early warning information related to natural disasters is accessible through the
National Meteorological and Geophysics Agency 14 . Land and Forest fire Early warning maps are very pre design (English website at www.fdrs.or.id
, this website
14
BMG - Operational building, 5 th floor, GIS room, Badan Meteorologi dan Geofisika, Jl. Angkasa I/2, Kemayoran
- Jakarta Pusat, 10720
22/09/02 11
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002 is under development phase). There are two locations that produce all maps, one is coming from Edmonton-Canada (Canadian Forest Service) and the second is coming from Indonesia (Meteorological and Geophysical Agency - BMG: www.bmg.or.id
).
The maps coming from Canada can arrive quite late because the weather data is coming from Indonesia (BMG system). The maps from Indonesia (BMG) are up to date. These maps get all weather data from whole Indonesia (Southeast Asia) on
16.00 LST, and therefore, the up-to-date maps are out every day at 16.00 LST.
2.5.2. Public Awareness
At household/individual level, the local populations are aware about the risk/survival mechanisms in case of emergency. Local people are familiar with the ways to manage disasters such as mild and moderate earthquake and fire. However, the public Community awareness … knowledge is not based on the scientific evidences.
The community people and leaders are rarely involved in emergency/disaster preparedness, coordination and emergency taskforces.
…on disasters, comes from spontaneous knowledge acquired from the lived experiences in disaster-prone areas rather than from an official/technical way.
Some of the Health Provincial authorities consider that community awareness on emergency/disasters is sufficient but also admit that this awareness comes from spontaneous knowledge acquired from the experiences in disaster-prone areas and not from an official-technical way.
A basic Guidebook exists on BMG Website regarding the basic preparation actions in case of earthquake for the population to undertake in order to protect itself. This guidebook seems to be a useful tool but there are no questions on public awareness.
2.5.3. Training
Numerous trainings took place throughout the country. However, not much training was conducted specifically on emergency preparedness in disaster situations. The quality of much training was considered to be at an inappropriate level. Trainings tended not to Perdiem Culture have good methodology, and lessons learned and knowledge acquired at the central or provincial level, has not been utilized for other provincial or regional trainings.
For a five-day workshop on TB, a health centre from NTT Province appointed the ambulance driver to attend the workshop, because he was the only staff who had not profited from any perdiem that year. Trainings were not conducted regularly, and the last official training took place few years ago in many provinces. The same people attended similar training and normally the attendants were not the appropriate ones. The criteria of selection of trainees and the high staff turnover among institutions do not allow sustainable and consistent conditions for benefiting from the emergency preparedness trainings.
The MoH trough the PPMK is supporting innovative training programs in emergency management such as UNHCR’s Emergency Management Training National
Workshop for Indonesia and WHO’s Health as a Bridge for Peace and
WHO/UNDP/DINSOS Emergency Health Preparedness training in North Maluku
Province. UNICEF supports BAKORNAS PBP by involving its high level staff
(especially Relief and Protection of Refugees/IDPs Office and Relief and Disaster
Victims Office) in Essentials of Humanitarian Practices (sponsored by RedR
Australia) and its Emergency Preparedness and Response Training (EPRT).
An IDPs Health Management training for Nurse/midwives (40 people) is being held in
North Malukus health provincial office to identify the shortcomings and the needs of several sub-districts. Recently, reconciliation program with religious and community leaders has been implemented.
22/09/02 12
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
Some activities for floods emergency preparedness improvement were mentioned in
Pidie District (NAD Province): a) community education, b) prevention of deforestation, c) river shoulders reinforcement, and d) rivers enlargement.
2.6. Examples of Positive Findings during the Field Visits
Examples of Positive Findings during the Field Visits
Fact Place
22/09/02 13
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
Satlak developed SOP on emergency in 1996 Sikka district
Tenggara)
(East Nusa
Satkorlak developed guidance and SOP on emergency
North Sumatra
Province Health Office established its own health emergency task force PBPP SATGAS for IDPs and
Disasters to identify the shortcomings and the needs of several sub-districts
Ternate (North Maluku)
Fast spontaneous emergency response from the local community and neighbourhood districts and other countries during Bengkulu earthquake on 4 June
2000.
Bengkulu
The police district commander utilised existed local system (mukim) for community participation for a better peace condition.
Pidie District (Aceh)
SSB radio communication was available at hospitals, districts, and health centres.
North Maluku and East Nusa
Tenggara
Disasters mapping are available at i.e. IDPs, flood, typhoon, landslides, haze, and earthquake.
North Sumatra Satkorlak office
Technical Environmental Sanitation Office performed air pollution measurements on two-week interval for 7 points.
South Kalimantan
Almost every village had a Fire Prevention Clubs, funded and operated by the local village community.
The clubs worked together in case of fires.
Banjarmasin (South Kalimantan)
3. Conclusions
3.1. General Conclusions
Natural and complex disasters/emergencies in Indonesia are now epidemic.
Management of these emergencies and their underlying causes will help contribute to the country’s future political stability. Lessons learned from the Indonesian
22/09/02 14
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
experience carry trans-national importance as Indonesia forms part of the arc of instability in the East Asian area.
Whereas Indonesia has an extensive history with natural and some man made disasters, complex emergencies represent a relatively recent type of disaster for
Indonesia. Managing these disasters has been widely acknowledged as difficult and frustrating for all domestic actors —from the National Coordinating board for Disaster
Management (BAKORNAS) which coordinates activities of involved ministries, to the
Ministry of Health (MoH), and to district health authorities. Lessons from one theatre of operation have not been transferred to another. Underlying these issues are lack of funding, experienced staff, and district-level disaster management infrastructure.
Indeed, emergencies and disasters affect all aspect of human life. Paralysed public services such as breakdown of the government system, the destruction of public facilities, and the disruption of communication and transportation systems, result in the disruption of the social order of society. The loss of life and property, and the increase in morbidity are also the significant impacts of a disaster. Hence, it is extremely important to shift an emergency management focus from the emergency response and rehabilitation to stronger preparedness in anticipating emergency and disaster situations.
3.2.Emergency Preparedness Coordination Mechanisms
Coordination – The role of BAKORNAS, SATKORLAK and SATLAK is not clear yet for various reasons, including 1) the persistent confusion between coordination, implementation and control mandates; 2) the conflicts of interest and leadership; 3) the heavy dependence on personalities, the absence of real delegation of authority and too many political choices; 4) the lack of permanent and operational intermediate structures that can assure continuity, and initiate and coordinate preparedness activities; 5) the weak sense of responsibility among the insufficient and underequipped staff; 6) the multiplication of autonomous decentralised entities does not facilitate the coordination process; and 7) a tendency for each administrative / sector entity to develop its own Emergency Response Team and Taskforces which increases duplication and confusion 15 .
The multiple efforts and activities being undertaken by the UN agencies on the emergency management and/or preparedness topics (See annex 7: “Activities Friend of BAKORNAS”) are not well coordinated within the UN systems, and are not necessarily endorsed by all national counterparts.
Political priorities - The level of political will from the local government and parliament regarding emergency preparedness has a determinant impact on the actions undertaken and the level of awareness and sensitivity of the community. When a disaster occurs, emergency relief gives a chance to the various stakeholders to highlight their role and responsibility, whereas emergency preparedness is less visible and less marketable and requires more underground and sustainable efforts.
Inter-levels relationships – The decentralisation and the process of autonomy have a direct impact on the roles, competences and responsibilities among the Provinces and Districts authorities and also on the perception that the population has on its immediate leaders. Emergency preparedness and relief, and conflict situations are major issues when power relationships are at stake between the central and decentralised authorities. The confusion between de-concentration and decentralisation has a strong impact on how coordination, information sharing, resource mobilisation and operations will be handled.
Mainstreaming – Emergency preparedness does not appear to have a routine organisation, structure and meeting procedures. It remains to date as an ad hoc
15 See Power Point slide in Annex 12 illustrating this paragraph.
22/09/02 15
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002 mechanism, without systematic guidelines and standardised operating procedures socialised up to sub-districts and community leaders.
Institutional changes - The last two years have been difficult for developing capacity in preparedness. With the changes in the government and the reorganization of the Ministries of Health and Social Welfare, as well as the Coordinating Ministry for Public Welfare, the No more IDPs from 1 st Jan. 2003 institutional responsibilities have not been clear. It is now expected that these institutions are better established and responsibilities will become clearer.
Therefore, efforts will be strengthened in the area of preparedness during this biennium. A central pending
According to official sources, the policy consisting of giving three choices to the IDPs (return, resettlement or installation) will solve the IDP issue. question concerns the role of DEPSOS, which is also responsible for humanitarian assistance for IDPs and for the return of IDPs to the places of their origins. Given that the IDPs issue (problem) is supposed to be over by the end of 2002, the role of
DEPSOS in disaster preparedness and management in the future is not yet certain.
3.3. Financial Mechanisms
Decentralised management - After 25 years of highly centralized government,
Indonesia has committed itself to decentralization of bureaucratic control starting from
2001. The fundamental change is that financial resources will be increasingly allocated to district (sub provincial) level and the officials in decentralized levels will have responsibility for financial management of district affairs.
Roles and responsibilities - The implementation of the laws on decentralization (as of 2001) has made the process of management of resources, both human and financial, between the central and provincial levels much more complex. The roles and responsibilities need to be further clarified, and regulations for disaster management, in particular, need to be established and implemented.
Funds availability at all levels - A limited amount of emergency funds from the
Indonesian government are available to the sub-districts, district, and provincial offices.
In addition, a contingency fund under the Ministry of
Health authority is available upon request from the district and the
MOH Secretary General
MOH 2002 budget for emergencies response: USD 14 millions
…is the budget truly available?
During the floods in Jakarta (February 2002), and upon request of the MOH, WHO Indonesia spent USD 47,000 to purchase few urgent-essential supporting items (8 rubber boats + engines, purifier water kits, and others). approval.
However, the released
The budget was approved at the end of 2001 but it was not released until April 2002. contingency fund takes 4 to 7 days since the district requested the fund. Thus, the channel to release contingency funds could drive into a long bureaucratic process. In addition, in general, the allocated funds from the central, provincial, district, and sub district government seem to be insufficient.
The international donor’s community has realised the importance of the preparedness to improve the readiness and response to emergency situations. More funds are available for national and international humanitarian actors (UN, NGOs), to undertake and develop projects on emergencies management. Nevertheless, these projects have been conceived as a short or medium term activities and therefore suffer from lack of sustainability.
3.4. Logistics and Communications
National logistics system
– Various storage / logistics systems exist in parallel, with no organised connections among them. There is a negative impact of the decentralisation on emergency-item stock organisation, availability and management
22/09/02 16
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002 at Provincial and District levels. BULOG/DOLOG stocks and funds management system is not transparent.
Stocks against needs – There is a contradiction in the current system between smaller stocks at decentralised levels but immediate bigger needs in case of emergency. This has been confirmed in past experiences (e.g. Bengkulu), when late response on delivery of additional drugs and other related health equipment from MOH created a gap in the timely emergency response.
Access – Access is usually very limited for structural (state of infrastructure) and safety reasons. Therefore, it is even more difficult to conduct emergency preparedness activities such as awareness and information campaigns and households vulnerability analysis.
Communications - Communication systems are poor. Usually, when communication means are available (SSB, Radio Hand Sets, Walkie-
Talkies, etc), a good majority is out of order because of lack of maintenance, and inappropriate knowledge or repair facilities. Mobile phone signals and relays are not dispatched homogeneously, and some important areas
An effective communication system between the radio stations is the key to the success of disaster response operations. such as airports are not within the mobile phone coverage.
Decentralisation and chain of command - When a disaster occurs, the chain of command has to overcome protocol and heavier bureaucracy/longer leverages due to decentralisation in order to efficiently mobilise all logistical means available.
3.5. Health Sector
Disaster impact on health situation - Disasters followed by mass evacuations often cause major health problems. These problems arise due to a shortage of clean water supply, which causes a decline in personal hygiene and environmental sanitation that can spin off the spread of various communicable diseases. Inadequate food supply can in the long run also cause a decline in health status due to decline in fulfilling nutritional requirements. Available refugee shelters are often below the accepted health standards. This can directly or indirectly cause a decline in individual’s body resistance, which if not adequately improved, may also give a rise to various health problems.
Replication of good practices - Not enough information circulates all the way from central to sub-district levels. It should be a 2-way process: information/initiative from
Central level and request from Provincial level and vice-versa.
Capacity building - Strategic issues here implies to improve inter-sectors coordination and cooperation, and health manpower capability, to empower the people in the disaster area, to increase the quality and accessibility of health services to disaster victims and to increase funding through humanitarian
PPMK
…
…enough resources for such a large responsibility? assistance. Improving emergency preparedness will directly improve emergency response system
Budget 2002: USD 200,000
Total staff: 45 persons. that allows for a smooth flow of information from Technical-qualified staff: 14 persons the field to the appropriate unit at the different levels (national, provincial or district), followed by a rapid, effective and coordinated response. In particular, PPMK qualified staff at central and all decentralised levels seems to be insufficient to properly accomplish the tasks and fulfil the responsibilities mentioned in its mandate.
Global awareness and sense of responsibility - Training professionals, and general population on emergency preparedness, would lead to a more effective response in case of emergencies and/or disaster. In the mean time, community
22/09/02 17
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002 empowerment approach should be improved particularly for those people living in disaster-prone areas.
22/09/02 18
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
4. Recommendations
NB : AEP recommendations are laid out in this section. Some of them are for a longer time horizon, but suggestions could be made for others, in which immediate actions could be made, and these points were specifically indicated under
Suggested Action Points.
4.1.Coordination
1. The UN humanitarian leadership and coordination mechanisms must be reinforced in order to present a proper model for the Government to improve its emergency preparedness capacity and efficiency. The International Community involved in humanitarian assistance should therefore increase their initiatives that set a ground for national counterparts actions, especially coordinated by BAKORNAS.
2. All emergency management structures at the central level must reinforce their own coordination mechanisms, decision-making processes and operational collaboration by clarifying the specific roles and responsibilities played and taken by each member of BAKORNAS. As a coordination body, BAKORNAS does not have implementation or policy-making functions. Indeed, the organisation and the mandate of the
Secretariat of BAKORNAS must be clarified and then, assumed effectively by all line ministries and other members of the Coordination Board. The same recommendation is applicable at all decentralised levels. A clear understanding on roles and responsibilities must be reflected at the decentralised levels among the members of
SATKORLAK and SATLAK structures.
4.2. Operation / Implementation
3. The sustainability of technical and financial support must be assured by strengthening and institutionalising national emergencies prevention and preparedness planning and activities. These interventions must aim at enhancing the effectiveness of the response and mitigating the impact of a disaster situation in a coordinated and
Effectiveness: a measure of the benefit to the large group as a result of the intervention. This measure is more sensitive than specific. efficient manner.
Suggested Action Points:
The GoI should allocate regular and sufficient funds from the National Budget, specifically for emergency preparedness.
Efficiency: a measure of the relationship between the results of the intervention and the cost of it, in terms of time, money and resources. This measure is more specific than sensitive.
The international donor community must strengthen the sustainability of emergency preparedness projects by supporting more effective projects
(horizontal programmes) than efficient ones (vertical programmes).
4. National and international institutions must coordinate health response and humanitarian assistance by providing health expertise and specific needed information. Internal collaboration among provinces and districts themselves should be also encouraged. Contingency plans, adapted guidelines and standard operating procedures must be developed not only in an integrated perspective but also sector by sector at all different levels (province, district, sub-district and community).
5. Early Warnings System (EWS), integrated, coordinated and all-sectors endorsed, has to be shaped, to describe the processes currently available in the country for early recognition of potential threats. That EWS should cover outbreaks of diseases and epidemics, shortage of food, severe weather, movements of population, social and political unrest, economic crisis, other foreseeable natural, technological and industrial hazards.
22/09/02 19
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
6. Specific operational platforms between military and civil disaster management institutions must be organised in order to consolidate the previous experience and means related to emergency preparedness, and facilitate the transfer of know-how.
Given the importance of the role of the Armed and Police Forces, there is a need to standardize military/civil cooperation agreement and procedures in case of emergencies at all levels.
Suggested Action Point:
Emergency preparedness sectors should conduct an in-depth and systematic joint assessment on logistical and communication capacities in all provinces with the support of qualified institutions such as TNI and Police.
4.3. Information, Capacity Building and Tools
7. The level of knowledge in emergency management must be improved by supporting capacity-building activities especially for health staff at decentralized levels. All emergency management sectors should be involved in organization of these activities.
Suggested Action Points:
Emergency preparedness issues should be incorporated in academic curricula.
Sustainable and all-sector endorsed training programmes, including training of trainers, should be conducted at decentralized levels.
8. The population must be supported in organizing its capacity in effective emergency preparedness and response. The communities must be aware of what may be done to quickly handle an emergency situation and to reduce mortality and morbidity during natural and/or complex disasters or other emergencies. A network for emergency preparedness amongst the population in disaster-prone areas must be promoted.
Suggested Action Point:
A socialisation campaign on emergency preparedness should be undertaken for the population across the country, with the support of specific tools, such as posters, booklets, videotapes, simulation exercises, etc.
9. Access and dissemination of the information must be strongly improved. National data reports and database for decision-making related to emergencies must be available in a clear and user-friendly way.
Suggested Action Points:
A complete inventory of available data, reports and maps in the country must be made.
An information needs assessment must be conducted.
BAKORNAS could establish an integrated Disaster Management Information
Website.
10. The exchange of experiences/procedures 16 among the countries in Southeast Asia, which face the similar emergency risks and common geopolitical challenges, 17 should be regularly held. Nevertheless, the experiences and knowledge acquired in other countries, with better emergency management systems, should be taken into consideration.
16 See Guidelines for Emergency Preparedness and Management, Philippines.
17 Useful resources on Disaster Preparedness in South East Asia can be found with the Asian Disaster
Reduction Centre, based in Bangkok (. The ADRC also presents basic information on Indonesia emergency preparedness profile.
22/09/02 20
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
Suggested Action Points:
A comparative study on emergency preparedness must be conducted at the
Southeast Asia regional level.
An evaluation must be conducted on existing tools and mechanisms in civil protection and defence, in other countries (FIMA in the United States, Plan
ORSEC in France, Danish Civil Protection, Proteccion Civil in Spain, etc.).
4.4. Specific Recommendations to WHO/OCHA
11. Part of the role of WHO is to strengthen the capacity of the Indonesian Government to deal with natural disasters and other emergencies in an efficient and effective fashion. The capacity for preparedness must be strengthen to prevent adverse effects of all crises. In this perspective, for WHO/EHA, PPMK should be the natural counterpart, as the representative of the MOH in the National Disaster Management
Coordination Body (BAKORNAS PBP). PPMK has produced guidelines on rapid health assessments, risk mapping, contingency planning, and has worked with some provinces on provincial disaster management plans (5 of 30 provinces have these plans).
Suggested Action Point:
WHO must establish an emergency management post to support the PPMK to accomplish its essential tasks, aiming at reaching a higher level of efficiency and effectiveness at all decentralized levels and building higher levels of readiness for response to any emergency or disaster.
12. Given the current multiple of efforts being undertaken by several UN actors (UNDP’s contribution, HCR’s involvement, WFP’s assistance, WHO’s assessment on health issues, CAP preparation, Regional DMTP) and the structural challenges faced by
BAKORNAS, OCHA must take the lead in facilitating the communication and coordinating these efforts and actors.
Suggested Action Point:
OCHA must reinforce its role as the leading trigger to facilitate the collaboration with the government, to coordinate activities and to promote the information sharing with other international organisations and all other sectors and/or actors involved in emergencies management activities in order to allocate resources effectively.
“A state of emergency preparedness exists when an environment has been established in which communities, through their public, private and voluntary services and institutions, are ready and able to cope effectively at any time with both the impact and consequences of most hazards without l ittle or no external assistance.”
22/09/02 21
Assessment on Emergency Preparedness in Indonesia, WHO/OCHA Mission, July/October 2002
5. List of Annexes
Annex 1
Annex 2
AEP Terms of Reference.doc
Information Sheet AEP Methodology.doc
Annex 3 National Workshop Report Jakarta July 2002.doc
Annex 3bis Map Origin of Workshop's Participants.ppt
Annex 4
Annex 5
Annex 5
Annex 5
AEP Base Questionnaire Form.doc
Bengkulu Field Report.doc
Namroe Aceh Darussalam Field Report.doc
North Maluku Field Report.doc
Annex 5
Annex 5
North Sumatra Field Report.doc
Nusa Tenggara Timur Field Report.doc
Annex 5 South Kalimantan Field Report.doc
Annex 5bis Maps Field Visits.ppt
Annex 5bis Bengkulu visit map.ppt
Annex 5bis Aceh visit map.ppt
Annex 5bis North Sumatra visit map.ppt
Annex 5bis North Maluku visit map.ppt
Annex 5bis NTT visit map.ppt
Annex 5bis South Kalimanta visit map.ppt
Annex 6
Annex 7
Information Sheet BAKORNAS.doc
Matrix Activities Friends of Bakornas.xls
Annex 8
Annex 9
Information Sheet PPMK.doc
List of People Met.doc
Annex 10 Documents consulted.doc
Annex 11 List of acronyms
Annex 12 Slide illustrating the impact of decentralisation on disaster management
22/09/02 22