Successful Resuscitation After Prolonged Cardiac Arrest in a Patient
advertisement

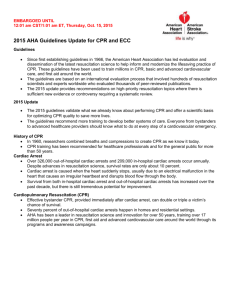
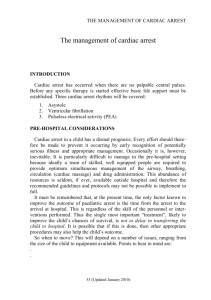
Successful resuscitation after prolonged cardiac arrest in a patient with massive hypertrophic cardiomyopathy Tzevan Poon, MD; Marshall Corson, MD; Stephen Hubbard, MD Department of Medicine (TP, MC, SH), Division of Cardiology (MC, SH), Harborview Medical Center, University of Washington. Seattle, WA 98104 Background: Sudden cardiac death (SCD) is a feared event in patients with hypertrophic cardiomyopathy (HCM), and most commonly afflicts those younger than 35 years old [1]. The risk of SCD has an estimated incidence of 1-2% per year. Risk factors for cardiac arrest in patients with HCM include a family history of SCD, otherwise unexplained syncope, non-sustained ventricular tachycardia (NSVT), abnormal cardiopulmonary exercise testing, and massive left ventricular hypertrophy (LVH) defined as left ventricular (LV) wall thickness 30mm (normal wall thickness <15mm) [1,2]. Resuscitation of HCM patients in cardiac arrest may pose numerous challenges due to the presence of severe LVH, dynamic LV outflow tract obstruction, mitral regurgitation, and diastolic dysfunction [1]. Objective: To report successful resuscitation with full neurologic recovery of a patient with massive HCM after cardiac arrest despite nearly two hours before return of sustained spontaneous circulation; and to underscore the importance of aggressive resuscitation and smooth transitions of care throughout the chain of survival despite unique logistical and medical challenges. Methods and Findings: A 19 year old previously asymptomatic male, diagnosed since age 13 with autosomal dominant HCM, was with two friends in a forest talking pictures of elk about 100 feet from the road at a remote national park, when he suffered cardiac arrest at approximately 1605. Out of cellular phone range, one friend ran to flag down a car, while the other started CPR and rescue breathing. Both friends learned basic life support (BLS) in public school. US park rangers arrived at about 1625 and took over chest compressions. Firefighters arrived 9 minutes later with an automated external defibrillator. The patient was cardioverted twice and a weak but palpable pulse with a blood pressure of 80mmHg/palpation was achieved at 1648, 43 minutes after CPR was first started. The patient was transported by rigid backboard off the trail and was sent by ambulance to a local airstrip. However the patient’s heart rhythm soon degraded into pulseless ventricular tachycardia and CPR was resumed. Critical care airlift was dispatched by helicopter at 1631 and arrived at 1702. Airlift nurses found the patient cold, cyanotic, with a Glasgow Coma Score of 3, and covered in vomit. Blood glucose was 115mg/dL. They intubated the patient with a 7.5 endotracheal tube using a Glidescope video laryngoscope (Verathon, Inc. Bothell, WA). CPR was continued for another 55 minutes, from 1707 to 1802, for ventricular fibrillation, ventricular tachycardia, and pulseless electrical activity. He was cardioverted an additional 6 times during this time. During the resuscitation, the patient was given intravenous boluses of epinephrine 1mg on four occasions, vasopressin 40 units once, calcium chloride 10mg/kg once, sodium bicarbonate 50mEq twice, atropine 2mg once, lidocaine 100mg twice, amiodarone 300mg once, and magnesium 2gm once. He received 1.2 liters of crystalloid. End tidal carbon dioxide monitoring used during CPR averaged only 17mmHg. The patient was airlifted at 1810, and arrived at our Emergency Department (ED) at 1842. His temperature was 35.2C, heart rate was 67 beats per minute, and blood pressure 78/40mmHg. A bolus of 100 micrograms of epinephrine was given. We then used a portable ultrasound (M-Turbo, Sonosite. Bothell, WA) to obtain a 4 chamber view of the heart which showed severe LVH and complete obliteration of the intraventricular chamber during systole suggesting that the patient was quite hypovolemic. We bolused 3 liters of crystalloid and the patient became hemodynamically stable without further need for inotropes or vasopressors. He was started on an amiodarone drip. We cooled the patient in the ED using an external temperature management system (Artic Sun. Medivance, Inc. Louisville, Colorado) in accordance with our institution’s mild hypothermia protocol; and he quickly reached a goal temperature of 32.4C, 123 minutes after arrival. Computer tomography of the head and neck showed no acute intracranial or cervical abnormality. Urine toxicology was negative for illicit substances. We treated the patient for non-ST elevation myocardial infarction (troponin-I peaked at 38.2ng/mL), pneumothorax and pneumomediastinum due to CPR, aspiration pneumonia, shock liver, acute kidney injury, and rhabdomyolysis. The patient was rewarmed after 24 hours to 37.4C (though his temperature rose spontaneously to 38.7C for a brief period). A formal transthoracic echocardiogram (TTE) obtained on hospital day 1 showed severe asymmetric hypertrophy with the intraventricular septum measured at 42mm from the subcostal view. The LV lateral wall was 31mm. A follow-up study showed severe LV outflow obstruction with a calculated peak gradient of 67mmHg (Figure 1, panel A). Right and left ventricular systolic function was normal. The patient continued to have no evidence of higher cortical function until hospital day 3 when he began to respond to simple commands. He was extubated on day 4 with no focal neurological deficits. By day 6 he was speaking fluently, chatting with his friends, and using the Internet on his smartphone. An episode of 12 seconds of rapid monomorphic NSVT (300 beats per minute) was noted on hospital day 6 (Figure 1, panel B). Formal neurocognitive testing initially showed isolated moderate memory deficits; however he improved and had only mild memory deficits on repeat testing prior to discharge. An automated implantable cardioverter defibrillator (AICD - Secura DR. Medtronic, Inc. Minneapolis, MN) was inserted on day 15. The patient was discharged home on day 17. Routine AICD interrogation shows that he continues to have brief episodes of asymptomatic NSVT. He has not received any AICD discharges. Eight months later our patient reports only trace occasional short-term memory loss. He has an active social life, and works at a local retail sports shop. Discussion: To our knowledge, this is the longest documented resuscitation of a patient with HCM with good outcome. We calculate his two episodes of total pulselessness lasted 43 and 55 minutes, and 117 minutes before return of sustained spontaneous circulation. We attribute the recovery of this patient to an uninterrupted chain of survival – including good quality CPR with frequent rotations; early cardioversion by first responders; transition to ACLS when available; expeditious transport to a tertiary care facility that cares for a high-volume of cardiac arrest patients; and early use of therapeutic mild hypothermia [3]. The patient’s youth and his prior high level of fitness may have also helped him survive. This patient was quite cool on arrival from the field and was subsequently further cooled. Mild hypothermia (32 - 35C) has been shown to improved neurological protection after cardiac arrest [4]. A randomized pilot study of 125 patients suggested that prehospital induction of mild hypothermia after return of spontaneous circulation from cardiac arrest may improve neurological outcome [5]. A larger multi-center randomized trial evaluating this timed intervention is ongoing at our institution. This case report also illustrates the benefit of point-of-care ultrasound in directing resuscitation efforts. We recommend ongoing collaborations with Cardiology, Emergency Medicine, and Critical Care departments to safely develop and deploy this emerging diagnostic modality. In summary, we demonstrate that successful outcome may be possible in patients with HCM despite challenging logistical issues, massive hypertrophic cardiomyopathy, and very prolonged resuscitation. (We thank the first responders, US National Parks Service rangers, firefighters of the cities of Greenwater and Buckley, and the University of Washington Airlift Northwest crew for being instrumental in this rescue.) Potential Conflicts of Interest: None reported. 1) Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002 Mar 13;287(10):1308-20. 2) Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.Circulation. 2011 Dec 13;124(24):2761-96. Epub 2011 Nov 8. 3) Peberdy MA, Callaway CW, Neumar RW, et al. Part 9: post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010 Nov 2;122(18 Suppl 3):S768-86. 4) Bernard SA, Gray TW, Buist MD, et al. Treatment of Comatose Survivors of Out-of-Hospital Cardiac Arrest with Induced Hypothermia. N Engl J Med 2002; 346:557-563 5) Kim F, Olsufka M, Longstreth WT Jr, Maynard C, et al. Pilot randomized clinical trial of prehospital induction of mild hypothermia in out-of-hospital cardiac arrest patients with a rapid infusion of 4 degrees C normal saline. Circulation. 2007 Jun 19;115(24):3064-70. Epub 2007 Jun 4.