1140_20061572_hcv-article - Pakistan Journal of Scientific and
advertisement

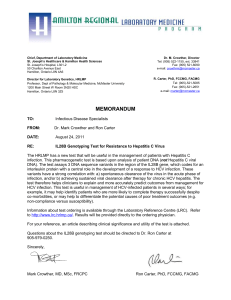
Overview of Hepatitis C Virus in Pakistani population Sumiya abbasi,kahkshan jabeen,Bushra uzair* *Corresponding author: Bushra uzair Islamic International University H-10, Islamabad Contact # 051 908 561 71 1 ABSTRACT. Hepatitis C virus (HCV) is an important human pathogen that causes acute and chronic hepatitis, cirrhosis and hepatocellular carcinoma worldwide. HCV is common among the Pakistani population. Approximately 10 million people could be carrier in Pakistan. HCV prevalence was moderate in the general population but very high in injecting drug users and multi-transfused populations. HCV enters the cell with CD81 and LSIGN, D-SIGN, Claudin-6/9 receptors(SRBI), (OCLN), (GAG), (LDLR), (EGFR), ephrin receptorA2 (EphA2), and Niemann-Pick C1-like L1 (NPC1L1 and its single stranded RNA genome directly serves as the template for translation. Accordingly, E1/E2 encode the outer membrane while nonstructural protein 4B (NS4B) induces the specific membrane alteration, designated as membranous web (MW), that harbors this complex. HCV NS3 is a serine protease/RNA helicase that plays a pivotal role in catalyzing the cleavage of the single polyprotein encoded by HCV after infection of hepatocytes. The HCV genome shows remarkable sequence variability 1 of E2 protein encoding region worldwide leading into 6 genotypes, numerous subtypes and HCV exists in each infected patient as quasispecies. The genotype may be linked to the severity of the disease and to the efficiency of the combination treatment with interferon and ribavirin. The epidemiology, pattern of transmission, different genotypes and clinical consequences of the disease has been studied worldwide, but little is known about the genomic organization and epidemiology of HCV infection in Pakistan. This review article covers key areas of HCV particularly its genomic organization, prevalence, life cycle, treatment options, genotypes and various factors associated with HCV infection in the Pakistani population. Key Words: HCV; genomic organization; genotypes; life cycle; treatment options. 2 INTRODUCTION Hepatitis C is a life threatening infectious disease of the liver which is caused by the hepatitis C virus (HCV). An estimated 170-200 million people worldwide are infected with HCV (Conca and Tarantino, 2009). HCV seroprevalence in Pakistan reported range between 2·4% and 6·5%. (Second highest in the world) (Luby, 1997, Khattak et al., 2000, Mujeeb et al., 2002). Egypt, with an estimated seroprevalence rate, 22% is reported to be highest in the world (Egypt data sheet 2005).10% of the Pakistani population is chronically infected with this viral pathogen (Farhana et al., 2009; Idrees and Riazuddin, 2009; Akbar et al., 2009). Still there is no vaccine developed against HCV which is often referred to as a silent killer (Suresh D Sharma, 2009). The existence of hepatitis C (originally "non-A non-B hepatitis") was postulated in the 1970s and proved conclusively in 1989 (Choo et al., 1989). The global epidemiology of viral hepatitis A and hepatitis B is well established, but HCV data remains limited, particularly in Pakistan (Raja and Janjua, 2008). In 2004 it was estimated by the WHO that the annual deaths due to liver cancer caused by HCV and cirrhosis were 3,08,000 and 7,85,000 respectively (World Health Organization 2004).HCV infection is well recognized and pose severe health problem worldwide, especially in the developing countries including Pakistan. HCV prevalence in Pakistani population is nearly 5%. Its prevalence in injection drug users (IDUs) and the multitransfused population is high, suggesting that the reuse of syringes is common among the injecting drug users, and blood transfusions are not properly screened here in Pakistan (Waheed et al., 2009). HCV cannot be contracted from or transferred to any other animal. Chimpanzees can be infected with the virus or the full length viral RNA made in the laboratory, but they do not develop the disease. The infection is often asymptomatic in most of the infected individual, but once 3 established, chronic infection can progress to scarring of the liver (fibrosis) and development of advanced scarring (cirrhosis) which is generally apparent after many years (Thomson et al., 2003). In some cases, those with cirrhosis will go on to the development of liver failure or other complications of cirrhosis including cancer or life threatening esophageal varices and gastric varices (Asselah et al., 2003). A relationship between insulin resistance and hepatitis C has been observed in HCV infected patients. Indeed, insulin resistance is frequently seen in patients with chronic hepatitis C than in healthy controls (Romero-Gomez, 2006). In a cross-sectional survey it was reported that HCV-positive persons have an increased risk for type II diabetes mellitus, more than 3-fold than persons without HCV infection but, no association was seen between HBV infected patients and diabetes type II (Mehta et al., 2000). In another study Diabetes mellitus was investigated and seen more often in cirrhotic patients. However, in a cohort of 45 non-cirrhotic HCV patients the prevalence of type II diabetes mellitus was 33% higher than in the control group (Knobler et al., 2000). Genotyping is important to guide treatment because some viral genotypes respond better to therapy than others. HCV PREVALENCE IN VARIOUS GROUPS Ten different studies showed that the percent prevalence of HCV in the general adult population was 4.95% ±0.53% (Luby et al., 1997, Tunveer et al., 2008). Four different reports showed a high 57% ± 17.7% prevalence of HCV among the IDUs (Kuo et al., 2006, Platt et al., 2009). Thalassemic and hemophilic patients require life-long blood transfusions, so it is necessary to obtain screened blood from a reputable source, because the multitransfused population is more prone to blood-borne pathogens. Arif et al reported that only 15.8% of parents of thalassemic children knew the importance of blood screening. Hamid et al reported that recapping of 4 syringes is the key factor for receiving needle stick injuries in health care workers and that transmission of HCV by needle stick injury ranges from 2% to 10%. Janjua et al reported that 68% of individuals received injections during the previous three months in Digri and Mirpurkhas, two districts of Pakistan, out of which only 54% were from freshly opened syringes. It has been reported from the US that up to 20% of new HCV infections are due to sexual activity (Alter, 1999). The main problems in Pakistan are illiteracy, lack of awareness about sexually transmitted diseases and low use of condoms among the sex workers. Saleem et al reported in 2005 that 17% of female sex workers, 3% of male sex workers and 4% of hijras (transgender men) consistently used condoms during the previous month; 67% of female sex workers were illiterate, 34% of female sex workers were suffering from sexually transmitted infections. HCV GENOTYPES AND THEIR DISTRIBUTION HCV has been categorized into different genotypes whose members have at least 67% nucleotides identity with each other (Jose et al., 2002). HCV has a highly variable sequence, allowing description of 11 genotypes and above 100 subtypes with different geographical distributions. Clinical outcomes as well as response to antiviral therapy are strongly influenced by HCV genotype (Eric et al., 2010).In Pakistan the prevalent genotype is 3a followed by genotype1a and 2a while other genotypes are quite rare (Idrees and Riazuddin, 2008). Genotype 3a and 1a are also the foremost genotypes in Indian population. (Narahari et al., 2009). HCV subtypes1a, 1b, 2a and 2b are found commonly in Unitesd States (Nainan et al., 2006).Genotyping is important to guide treatment because some viral genotypes respond better to therapy than others. The genetic diversity of HCV is one reason due to which it has been 5 difficult to develop an effective vaccine. In Taiwan the most common genotype is 1b (Lee et al., 2010). Type 4 is found in Middle East countries (Ayesh et al., 2009). Genotype 6 is found in Hong Kong, Thailand, south China and south-east Asian population (Akkarathamrongsin et al., 2010). Genotype 1 and 4 has been reported to be the common genotypes in African countries (Muasya et al., 2008). In Sri Lankan population genotypes 1b and 2b are the leading genotypes (Senevirathna et al., 2008) while in Korean population the most prevalent genotype is 1b followed by 2a (Shin, 2006). More than two of every three persons who are infected by HCV may continue to have the virus in their blood, which can transmit the infection to others. Those at increased risk of developing HCV include: Healthcare workers who expose themselves with infected blood from a cut or bruise or from a device or instrument that has been infected ("contaminated") Persons who inject illicit drugs into their veins and skin, with shared needles and syringes Anyone who gets a tattoo or has his or her skin pierced with an infected needle Persons with hemophilia who require large amounts of blood and blood products after bleeding Patients with kidney disease who have periodic dialysis and often requires the patient to have blood transfusions About one-fourth of patients with HCV do not belong to any of these high-risk groups. Although blood transfusion is now a much less common cause of HCV infection than in earlier years, but cases still occur. Also, sexual transmission is possible, and may take place with either heterosexual or homosexual behavior (Ask.com, 2010). 6 WHAT ARE THE SYMPTOMS OF HCV INFECTION? About 75% of people have no symptoms when they first acquire HCV infection. The remaining 25% may complain of fatigue, loss of appetite, muscle aches or fever. Yellowing of the skin or eyes (jaundice) is rare at this early stage of infection. Over time, the liver with chronic infection may begin to experience the effects of the persistent inflammation caused by the immune reaction to the virus. Blood tests may show elevated levels of liver enzymes, a sign of liver damage, which is often the first suggestion that the infection may be present (Zechini et al., 2004). Patients may become easily fatigued or complain of nonspecific symptoms. As cirrhosis develops, symptoms increase and may include: weakness, loss of appetite, weight loss, breast enlargement in men, a rash on the palms, difficulty with the clotting of blood, and spider-like blood vessels on the skin. GENOME ORGANIZATION HCV is a member of the Flaviviridae and is the leading cause of chronic hepatitis and liver cirrhosis in humans in the third world countries (Tanaka et al., 1996). The genome of HCV is a 9,600 nucleotides long positive-strand RNA that is translated into a polyprotein of approximately 3,010amino acids (Tanaka et al., 1996). The 5’-NCR is highly conserved among different HCV isolates and contains IRES that is essential for cap-independent translation of the viral RNA. The 3’-NCR is composed of a short variable region which is a poly(U/UC) tract with an average length of 80 nucleotides, and an invariant of 98 nucleotide RNA elements which is designated the X-tail (Kolykhalov et al., 1996). The conserved elements in the 3’-NCR,including a minimal poly(U) tract of about 25 bases, are essential for replication in cell culture (Yi Male et al., 2003) and in vivo (Kolykhalov et al., 2000). Translation of the HCV yields a polyprotein 7 precursor that is co- and post-translationally processed by cellular and viral proteases into the mature structural and non-structural proteins. Figure: 1 (Genetic organization and polyprotein processing of HCV) Once initiated, translation of the HCV genome produces a large polyprotein which undergoes proteolytic processing by both host signal peptidases and viral proteases to yield 10 mature viral structural (C, E1, and E2) and nonstructural (p7, NS2, NS3, NS4A, NS4B, NS5A, and NS5B) proteins (Figure 1). The structural proteins and the p7 polypeptide are processed by the endoplasmic reticulum (ER) signal peptidase whereas the non-structural proteins are processed by two viral proteases, the NS2–3 protease and theNS3–4A serine protease. The HCV core protein is a highly basic, RNA8 binding protein, which presumably forms the viral capsid. The HCV core protein is a 191aa precursor of 23-kDa. In addition to its role in viral capsid formation; the core protein has been suggested to directly interact with a number of cellular proteins and pathways which are important in the viral lifecycle (McLauchlan, 2000). The two envelope glycoproteins, E1 and E2, are essential components of the HCV virion envelope and necessary for viral entry and fusion (Nielsen et al., 2004). E1 and E2 have molecular weights of 33-35 and 70-72 kDa, respectively. These proteins are involved in entry of virion in the cell through cell surface receptors. p7 is a small, 63 aa polypeptide, that is shown to be an integral membrane protein (Carrere-Kremer et al., 2002). NS2 is a non-glycosylated transmembrane protein of 21-23 kDa. It consists of two internal signal sequences at aa positions 839-883 and 928-960, which are responsible for ER membrane association (Yamaga andOu, 2002). NS2, together with the amino-terminal domain of the NS3 protein, theNS2-3 protease, constitutes a zinc-dependent metalloprotease that cleaves the site between NS2 and NS3 (Hijikata et al.,1993). NS3 is a multi-functional viral protein of 70kD containing a serine protease domain in its N terminal third and a helicase/NTPase domain in its C-terminal twothirds. NS4A,which is a small protein of 54 amino acid residues, is a cofactor of NS3 protease activity. The NS3-NS4A protease is essential for the HCV lifecycle. It catalyzes HCV polyprotein cleavage at the NS3/NS4A, NS4A/NS4B, NS4B/NS5A and NS5A/NS5B junctions. NS4B is an integral membrane protein of 261 aa with an ER or ER-derive membrane localization (Hugle et al., 2001; Lundin et al., 2003). One of the functions of NS4B is to serve as a membrane anchor for the replication complex (Egger et al., 2002). NS5A is a 56-58 kDa phosphorylated zinc-metalloprotein that probably plays an important role in virus replication and regulation of cellular pathways. NS5B belongs to a class of membrane proteins termed tail- 9 anchored proteins (Ivashkina et al., 2002). An alternative reading frame (ARF) was identified in the HCV core coding region, as a result of a –2/+1 ribosomal frame shift in genotype 1a which has the potential to encode a protein of up to 160 amino acids and designated ARFP (alternative reading frame protein) or F (frameshift) protein (Branch et al., 2005). THE HCV LIFECYCLE HCV only infects humans and chimpanzees. Hepatocytes are the main target cells but infection of B cells, dendritic cells and other cell types has also been reported. All hepatitis C viruses are made up of an outer coat (envelope) and have enzymes and proteins that allow the virus to replicate within the cells of the body particularly liver cells (hepatocytes). Enveloped virus particles interact with specific surface receptors CD81 (a tetraspanin protein) is found on the surface of many cell types, including hepatocytes scavenger receptor class B type I (SR-BI), the LDL receptor (LDLR), and claudin-1 have been proposed as HCV receptors (Bartosch et al., 2006) Fusion of the viral and cellular membranes, triggered by the low pH of the endocytic compartment leads to the release of a single-stranded (ss), positive-sense RNA genome into the cytoplasm of a newly infected cell. This genome serves multiple roles within the virus life cycle: first, as a messenger RNA (mRNA) for translation of the viral proteins; second as a template for RNA replication; and third, as a nascent genome packaged within new virus particles. As in all positive-strand RNA viruses, HCV RNA replication occurs in association with altered cytoplasmic membranes. 10 Figure: 2 (Lifecycle of HCV. (a) Viral entry; (b) cytoplasmic release and uncoating; (c) IRESmediated translation and polyprotein processing; (d) RNA replication; (e) packaging and assembly; (f) virion maturation and release) Little is known about the process of HCV RNA synthesis within the replication complex (Cocquerel et al., 2006).With reference to related viruses, RNA synthesis is likely to be semiconservative and asymmetric where the positive-strand genome serves as a template to make a negative-strand intermediate and this negative strand then serves as a template to produce multiple nascent genomes. Nascent products from these reactions are protected from nuclease digestion by protease-sensitive factor and a detergent(Yang G. 2004). It is interesting to note that protease treatment of permeabilized cells destroyed most NS proteins without compromising RdRP activity which suggests that only a small fraction of NS proteins is actively engaged in RNA replication. The function of the ‘excess’ NS proteins and composition of the HCV replicase remain intriguing areas for future study. 11 TREATMENT OPTIONS FOR HCV When HCV was discovered in 1989, drugs targeting the viral proteins were expected to reach clinics rapidly (Choo et al., 1989). But more than two decades on, patients and physicians are still waiting. The current standard treatment for HCV infection involves weekly injections of pegylated interferon-α, with oral ribavirin twice-daily. These drugs, both of which are general inhibitors of viral infection, often have serious side effects, including depression and flu-like symptoms. Still completion of the year-long course of treatment does not always cure the patient, with success depending on characteristics of the virus, such as strain (the viral genotype), as well as host attributes, such as genetic variations. Generally, patients infected with HCV genotypes 2 or 3 more readily achieve a sustained viral response (SVR) than those infected with HCV genotype 1 (Jamall et al., 2008). A sustained virological response is achieved in 61% of the HCV patients getting IFN therapy. Several studies have shown an association between HCV genotype and both the responsiveness to interferon treatment and the extent of clinical progression of chronic HCV infection (Yoshioka et al., 1992). Studies have shown that there is a strong correlation of HCV genotypes with the grade and extent of steatosis, impaired glucose tolerance, body mass index (BMI), atherogenic lipid profile and insulin resistance (Szanto et al., 2006) and such genotype specific correlations are of high interest and clinical significance. It is noteworthy that the interferon alpha therapy for HCV is associated with many side effects such as emotional disturbances, cognitive impairment, chronic fatigue and psychotic states (Małyszczak et al., 2006). Viral enzymes are the prime targets for drug development, traditionally. Several HCV enzymes are required for the virus’s replication, including two proteases (NS2-3 and NS3-4A), a helicase 12 (NS3) and a polymerase (NS5B). Of these, NS3-4A and NS5B are the most attentive drug targets, showing encouraging results in clinical trials (De Francesco et al., 2005, Kwong et al., 2008). But the rapid and error-prone replication of HCV makes the emergence of drug resistance a significant issue. To combat resistance, cocktails of antiviral drugs with diverse mechanisms of action will probably be required, and researchers have therefore started looking beyond the viral enzymes. The antiviral drugs development has been hampered due to presence of several genotypes of HCV and hundreds of quaspecies distributors. At NCVI-NUST scientists have successfully obtained the consensus regions that can be targeted as peptide vaccine. The HCV pseudo type particles expressing HCV envelope proteins have been successfully generated that offer a great promise to be tested as vaccine specific for each genotype. Attempts are underway to develop nonhuman primate model for HCV infection where various antiviral (anti-protease, anti-helicase, anti-replicase) compounds will be tested. 13 REFERENCES Choo Q, Kuo G, Weiner A, Overby L, Bradley D and Houghton M. 1989. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science. 244 (4902): 359– 362. Yoshioka K, Kakumu S, Wakita T, Ishikawa T, Itoh Y, Takayanagi M, Higashi Y, Shibata M and Morishima T. 1992. Detection of hepatitis C virus by polymerase chain reaction and response to interferon-alpha therapy: relationship to genotypes of hepatitis C virus. Hepatology. 16 (2): 293299. Hijikata M, Shimizu YK, Kato H., Iwamoto A, Shih J W, Alter HJ, Purcell RH and Yoshikura H. 1993. Equilibrium centrifugation studies of hepatitis C virus: evidence for circulating immune complexes. J. Virol. 67: 1953-1958. Kolykhalov A A, Feinstone S M and Rice C M. 1996. Identification of a highly conserved sequence element at the 3" terminus of hepatitis C virus genome RNA. J. Virol. 70: 3363–3371. Luby SP, Qamruddin K, Shah AA, Omair A, Pahsa O, Khan AJ, McCormick JB, Hoodbhouy F, Fisher-Hoch S. 1997. The relationship between therapeutic injections and high prevalence of hepatitis C infection in Hafizabad, Pakistan. Epidemiol Infect. 119: 349-356. Hamid SS, Farooqui B, Rizvi Q, Sultana T, Siddiqui AA. 1999. Risk of transmission and features of hepatitis C after needlestick injuries. Infect Control Hosp Epidemiol. 20: 63-64. Hepatol. 31 Suppl 1: 88-91. Knobler H, Schihmanter R, Zifroni A, Fenakel G, Schattner A. 2000. Increased risk of type 2 diabetes in noncirrhotic patients with chronic hepatitis C virus infection. Mayo. Clin. Proc. 75 (4): 355-359. Kolykhalov A A, Mihalik K, Feinstone S M and Rice C M. 2000. Hepatitis C virus-encoded enzymatic activities and conserved RNA elements in the 3" nontranslated region are essential for virus replication in vivo. J. Virol. 74: 2046–2051. McLauchlan J. 2000. Properties of the hepatitis C virus core protein: a structural protein that modulates cellular processes. J Viral Hepat. 7: 2-14. Mujeeb SA., Shahab S., Hyder AA. 2000. Geographical display of health information: study of hepatitis C infection in Karachi, Pakistan. Public Health. 114: 413–15. 14 Mehta, SH, Brancati FL, Sulkowski MS, Strathdee SA, Szklo, M and Thomas, DL. 2001. Prevalence of type 2 diabetes mellitus among persons with hepatitis C virus infection in the United States. Hepatology. 33 (6): 1554. Carrere-Kremer S, Montpellier-Pala C, Cocquerel L, Wychowski C, Penin F, and Dubuisson J. 2002.Subcellular localization and topology of the p7 polypeptide of hepatitis C virus. J Virol. 76: 3720-3730. Ivashkina N, Wolk B, Lohmann V, Bartenschlager R, Blum HE, Penin F and Moradpour D. 2002. The hepatitis C virus RNA-dependent RNA polymerase membrane insertion sequence is a transmembrane segment. J. Virol. 76: 13088-13093. Jose LW , Gutierrez JA, Branch-Elliman W, Stump DD, Keller TR, Rodriguez A, Benson G and Branch AD. 2002. Mutation Master: profiles of substitutions in hepatitis C virus RNA of the core, alternate reading frame, and NS2 coding regions. RNA. 8(5): 557-571. Khattak, MF.,Salamat, N., Bhatti FA., Qureshi, TZ.2002. Seroprevalence of hepatitis B, C and HIV in blood donors in northern Pakistan. J Pak Med Assoc. 52: 398–402. Asselah T, Boyer N, Guimont MC, Hatem DC, Tubach F and Nahon K. 2003. Liver fibrosis is not associated with steatosis but with necroinflammation in French patients with chronic hepatitis C. Gut. 52:1638-1643. Lundin M, Monne M, Widell A, Von Heijne G and Persson MA. 2003. Topology of the membraneassociated hepatitis C virus protein NS4B. J. Virol. 77: 5428-5438. Michael T,Michelina N, Michael B, Havert, Marian M, Sophia G, Harvey A, Stephen M, Feinstone, Krishna K, Murthy, Barbara R, and T. Jake Lian. 2003. The Clearance of Hepatitis C Virus Infection in Chimpanzees May Not Necessarily Correlate with the Appearance of Acquired Immunity. Journal of Virology. 77: 862-870. Yi M and Lemon S M. 2003. Nontranslated RNA signals required for replication of hepatitis C virus RNA. J. Virol. 77: 3557-3568. Janjua NZ, and Nizamy MA. 2004. Knowledge and Practices of Barbers about Hepatitis B and C Transmission in Rawalpindi and Islamabad. J. of Pak. Med. Asso. 54: 116. Nielsen SU, Bassendine M F, Burt AD, Bevitt DJ, and Toms GL. 2004.Characterization of the genome and structural proteins of hepatitis C virus resolved bfrom infected human liver. J Gen Virol 85: 1497-1507. World Health Organization. 2004. Department of Measurement and Health Information. Available 15 YamagaAK, and Ou J H. 2002. Membrane topology of the hepatitis C virus NS2 protein. J. Biol.Chem. 277: 33228-33234. Yang G. 2004. Newly synthesized hepatitis C virus replicon RNA is protected from nuclease activity by a protease-sensitive factor(s). J. Virol. 78: 10202–10205. Zechini B, Pasquazzi C and Aceti A. 2004. Correlation of serum aminotransferases with HCV RNA levels and histological findings in patients with chronic hepatitis C: The role of serum aspartate transaminase in the evaluation of disease progression. Eur. J. Gastroenterol. Hepatol. 16: 891–896. Branch AD, Stump DD, Gutierrez JA, Eng F &Walewski JL. 2005. The hepatitis C virus alternate reading frame (ARF) and its family of novel products: the alternate reading frame protein/F-protein, the double-frameshift protein, and others. Semin. LiverDis. 25: 105–117. Janjua NZ, Akhtar S, Hutin YJ. 2005. Injection use in two districts of Pakistan: implications for disease prevention. Int J Qual Health Care. 17: 401-408. Bartosch B and Cosset FL. 2006. Cell entry of hepatitis C virus. Virology. 348: 1–12. Cocquerel L, Voisset C andDubuisson J.2006. Hepatitis C virus entry: potential receptors and their biological functions. J. Gen. Virol. 87: 1075–1084. Kuo I, ul-Hasan S, Galai N, Thomas DL, Zafar T, Ahmed MA, Strathdee SA. 2006. High HCV seroprevalence and HIV drug use risk behaviors among injection drug users in Pakistan. Harm Reduct J. 3: 26. Małyszczak K, Inglot M, Pawłowski T, Czarnecki M, Rymer W and Andrzej K. 2006. Depressive symptoms during treatment with interferon alpha for HCV infection-preliminary report. Psychiatr Pol. 40 (4): 799-808. Nainan OV, Alter MJ, Kruszon-Moran D, Gao FX, Xia G, McQuillan G and Margolis HS. 2006. Hepatitis C virus genotypes and viral concentrations in participants of a general population survey in the United States. Gastroenterol. 131 (2): 478-484. Romero-Gomez. 2006. Hepatitis C and insulin resistance: steatosis, fibrosis and nonresponse. REV. ESP. ENFERM. DIG. 98: 605-615. Shin HR. 2006. Epidemiology of hepatitis C virus in Korea. Intervirol. 49 (1-2):18-22. Szanto P, Grigorescu M, Dumitru I and Serban A. 2006. Steatosis in hepatitis C virus infection. Response to anti-viral therapy. J. Gastrointestin. Liver Dis. 15 (2):117-124. 16 Arif F, Fayyaz J, Hamid A. 2008. Awareness among parents of children with thalassemia major. J Pak Med Assoc. 58: 621-624. Idrees M and Riazuddin S. 2008. Frequency distribution of hepatitis C virus genotypes in different geographical regions of Pakistan and their possible routes of transmission. BMC Infectious Diseases. 8: 69. Jamall IS, Yusuf S, Azhar M and Jamall, S. 2008. Is pegylated interferon superior to interferon, with ribavarin, in chronic hepatitis C genotypes 2/3? World J. Gastroenterol. 14 (43): 6627-31. Kwong, A. D., McNair, L., Jacobson, I. and George, S. 2008. Curr.Opin. Pharmacol. 8, 522–531. Muasya T, Lore W, Yano K, Yatsuhashi H, Owiti FR, Fukuda M, Tamada MY, Kulundu J, Tukei J and Okoth FA. 2008. Prevalence of hepatitis C virus and its genotypes among a cohort of drug users in Kenya. East Afr. Med. J. 85 (7): 318-25. Saleem NH, Adrien A, Razaque A. 2008. Risky sexual behavior, knowledge of sexually transmitted infections and treatment utilization among a vulnerable population in Rawalpindi, Pakistan. Southeast Asian J Trop Med Public Health. 39:642-648. Senevirathna D, Ranaweera D, Abeysekera D, Kanakarathana N, De Silva D, Abeysundara S, Samaraweera P, Jayasinghe S and Fernandopulle N. 2008. Genotypes of hepatitis C virus (HCV) in liver disease patients in Sri Lanka. Southeast Asian J. Trop. Med. Public Health. 39 (6):10541056. Tunveer A, Batool K, Qureshi WA. 2008. Prevalence of Hepatitis B and C in university of Punjab, Quaid-e-Azam campus, Lahore. ARPN J Agri and Bio Sci. 3: 30-32. Abraham .L, Yang T, Blair M, Roden DM and Darbar D. 2009. Augmented potassium current is a shared phenotype for two genetic defects associated with familial atrial fibrillation. J. Mol. Cell Cardiol. 48 (1): 181-190. Akbar, H., Idrees, M., Manzoor, S., Rehman, I.U., Butt, S., Yousaf, M.Z., Rafique, S., Awan, Z., Khubaib, B., Akram, M., Aftab, M., 2009. Hepatitis C virus infection: a review of the current and future aspects and concerns in Pakistan. J. Gen. Mol. Virol. 1 (2), 12–18. Alter MJ. December 7, 2009. Hepatitis C virus infection in the United States. J 5652 ISSN 10079327 CN 14-1219/R World J Gastroenterol.15,4. Ayesh BM, Zourob SS, Abu-Jadallah SY and Shemer-Avni Y. 2009. Most common genotypes and risk factors for HCV in Gaza strip: a cross sectional study. Virol. J. 16 (6): 105 17 Conca P and Tarantino G. 2009. Hepatitis C virus lymphotropism and peculiar immunological phenotype: effects on natural history and antiviral therapy.World Journal of Gastroenterology. 21:15(19):2305-2308. Narahari S, Juwle A, Basak S and Saranath D. 2009. Prevalence and geographic distribution of Hepatitis C Virus genotypes in Indian patient cohort. Infect Genet Evol. 9(4): 643-645. Platt L, Vickerman P, Collumbien M, Hasan S, Lalji N, Mayhew S, Muzaffar R, Andreasen A, Hawkes S. 2009. Prevalence of HIV, HCV and sexually transmitted infections among injecting drug users in Rawalpindi and Abbottabad, Pakistan: evidence for an emerging injection-related HIV epidemic. Sex Transm Infect. 85 Suppl 2: ii17-ii22. Suresh D Sharma. 2009. Why No Vaccine For Hepatitis C Virus Yet? J.K. Science. 11: 99-101. Waheed Y, Shafi T, Safi SZ and Qadri I. 2009. Hepatitis C virus in Pakistan: a systematic review of prevalence, genotypes and risk factors. World J. Gastroenterol. 15 (45): 5647-5653. Akkarathamrongsin S, Praianantathavorn K, Hacharoen N, Theamboonlers A, Tangkijvanich P, Tanaka Y, Mizokami M and Poovorawan Y. 2010. Geographic distribution of hepatitis C virus genotype 6 subtypes in Thailand. J. Med. Virol. 82 (2): 257-262. Lee YM, Lin HJ, Chen YJ, Lee CM, Wang SF, Chang KY, Chen TL, Liu HF and Chen YM. 2010. Molecular epidemiology of HCV genotypes among injection drug users in Taiwan: Full-length sequences of two new subtype 6w strains and a recombinant formb2b6w. J. Med Virol. 82 (1): 5768. 18