Policy - Tairawhiti District Health
advertisement

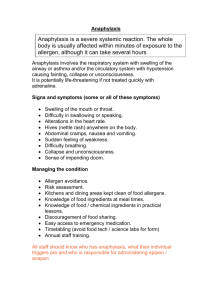
Sponsor: Clinical Board Name: Anaphylaxis Policy ORGANISATIONAL POLICY: ANAPHYLAXIS POLICY Immediate management plan for a patient suffering from an anaphylactic reaction AUTHOR: Resuscitation Coordinator AUTHORITATIVE SOURCES: New Zealand Resuscitation Council United Kingdom Resuscitation Council Tairawhiti District Health (TDH) Resuscitation Committee Clinical Board PURPOSE: To ensure all patients who are experiencing an anaphylactic reaction are cared for using a standardised management plan based on contemporary best practice guidelines To enable the healthcare professional to treat immediately to prevent further deterioration in the patients condition To highlight the differences in the resuscitation management of a patient who has arrested due to anaphylaxis SCOPE OF POLICY: The following policy applies to all staff of TDH who administer or use substances likely to cause an allergic reaction or who are responsible for caring with those with an anaphylactic reaction during their usual clinical role. POLICY STATEMENTS: TDH will regard an anaphylactic reaction as a medical emergency and will treat it with the same urgency as a cardiac arrest TDH will adopt the current recommended management principles and guidelines of the New Zealand Resuscitation Council in regard to treating patients experiencing anaphylaxis. TDH acknowledge that individuals will work within their scope of practice as health professionals TDH recognise that the exact treatment will depend on the severity of the patients condition, their location and the expertise, equipment and drugs available Author: Resuscitation Co-ordinator Authorised By: Chief Executive Date of first approval: November 2008 Date last review completed: November 2008 Page:1 of 9 Sponsor: Clinical Board Name: Anaphylaxis Policy DEFINITIONS: Anaphylaxis: ‘Anaphylaxis is a severe life threatening generalised, systemic hypersensitivity reaction that involves an abnormal/antibody response to a trigger. It is characterised by rapidly developing life-threatening airway and/or breathing and/or circulation problems usually associated with skin and mucosal change’ – World Health Organisation 2003(1) Severe anaphylaxis may lead to respiratory arrest due to bronchoconstriction. Anaphylaxis can cause cardiac arrest within minutes of initial reaction, where PEA (Pulseless Electrical Activity) rapidly deteriorates into asystole due to severe hypovolaemia and hypoxia. Causes: Common precipitating agents are stings, food, antibiotics, contrast media, thrombolytics, non steroidal anti-inflammatory drugs and anaesthetic agents Influencing Factors: Conditions such as asthma, pre-existing hypovolaemia, heart failure and coronary disease predispose the patient to increasing levels of severity and potentially fatal complications. Some drugs also emphasise the anaphylaxis or the effects of adrenalin, for e.g. betablockers, tricyclic anti depressants, MAOI For the purpose of this document, the following definitions apply: Hypotension: systolic blood pressure below 90mmHg Hypovolaemia: decrease in the volume of circulating blood Bronchospasm: constriction of small airways Angioedema - swelling of deeper tissues. Most commonly in the eyelids and lips, and sometimes in the mouth and throat Erythema – a patchy or generalised red rash Urticaria – also known as hives, weals or welts. Pale pink or red nettle sting type rash. Can be different shapes and sizes. Usually itchy Trigger/ Allergen - the substance that is the cause of the reaction – for example drug, sting, food type Cardiovascular collapse - A sudden loss of effective blood flow due to cardiac and/or peripheral vascular factors PEA - Pulseless Electrical Activity - Cardiac arrest in the presence of ECG complexes but no palpable pulse Author: Resuscitation Co-ordinator Authorised By: Chief Executive Date of first approval: November 2008 Date last review completed: November 2008 Page:2 of 9 Sponsor: Clinical Board Name: Anaphylaxis Policy Differential diagnosis – other potential causes for signs and symptoms AVPU – a tool used for assessing conscious levels. (Alert, Voice, Pain, Unresponsive) DRS ABC – the systematic approach used when dealing with a collapse. (Dangers? Response? Send for help, Airway? Breathing? Circulation?) Diagnosing Anaphylaxis Anaphylaxis is likely when the following criteria are met: Sudden onset and rapid progression of symptoms Life-threatening Airway and/or Breathing and/or Circulation problems +/- Skin and/or mucosal changes (flushing, urticaria, angioedema) The following supports the diagnosis: Exposure to a known allergen for the patient Remember Skin or mucosal changes alone are not a sign of an anaphylactic reaction Skin and mucosal changes can be subtle or absent in up to 20% of reactions (some patients can have only a decrease in blood pressure, i.e. a Circulation problem) There can also be gastrointestinal symptoms (e.g. vomiting, abdominal pain, incontinence) Management Principles The exact treatment will depend on the severity of the patient’s condition, their location and the expertise, equipment and drugs available- but the main stays of the treatment are administration of Adrenaline Fluid therapy Antihistamines Corticosteroids Author: Resuscitation Co-ordinator Authorised By: Chief Executive Date of first approval: November 2008 Date last review completed: November 2008 Page:3 of 9 Sponsor: Clinical Board Name: Anaphylaxis Policy Management guidelines Due to the potential rapidity of patient deterioration it is essential to adopt a rational systematic approach –‘DRS’ A B C D E’ and it is necessary to treat life threatening problems as they are recognized For staff working in the community setting the emphasis is on removal of the allergen, early call for help by dialling 111, laying the patient flat, administration of IM Adrenaline and continual reassessment of the patient’s airway, breathing and circulation until help arrives If the diagnosis of anaphylaxis seems most likely: Stop the administration of any intravenous drug or remove the direct exposure to the allergen. (For e.g. if latex suspected wash out wound/skin that had contact, or removal of the bee sting) Call for help and activate the 777 alarm. Lie the patient flat Give high flow oxygen as soon as it becomes available and monitor oxygen saturations Assess the degree of Angioedema (A) - presence of hoarse voice, stridor, feeling of throat closing over Assess the degree of Bronchospasm (B) – signs of breathing difficulty, wheeze and respiratory distress Attach patient to a cardiac monitor. Assess the degree of Cardiovascular collapse (C) –evidence of tachycardia, hypotension, pallor, clamminess. Disability (D) - Assess patients conscious level by using the AVPU scale Exposure (E) – Check the patient for any signs of rash or mucosal swelling Exclude other life threatening and non life threatening differential diagnoses: e.g. asthma, meningococcal sepsis, heart failure, tension pneumothorax, panic attacks. If the patient shows signs of angioedema, bronchospasm or cardiovascular collapse immediately: Administer IM Adrenalin 0.5mg (or 0.5ml) of 1:1000 into the thigh muscle If hypotensive, tilt the patients bed so that legs are raised Attempt to insert a large size 14 gauge cannula, into the antecubital fossa or other available large vein, if this is difficult any size cannula is better than no cannula at all. If this is not possible – IO access is a viable option in children and adults Commence rapid intravenous fluid infusion of either colloid, preferably Starquin, or normal saline. Adjust the following fluid requirements according to patient’s needs – aim for systolic BP above 90 mmhg. Between 1-3 litres of saline and 500-1500ml of colloid is usually needed Author: Resuscitation Co-ordinator Authorised By: Chief Executive Date of first approval: November 2008 Date last review completed: November 2008 Page:4 of 9 Sponsor: Clinical Board Name: Anaphylaxis Policy If time allows go ahead and administer the antihistamine – IV Promethazine 25mg by slow intravenous injection and the corticosteroid – IV Hydrocortisone 250mg (both can be given IM/IO if IV access unavailable) NB IV promethazine and IV hydrocortisone will not affect the haemodynamic or the respiratory state of critical condition- so although important do not let them delay other lifesaving treatments, for e.g IV fluids, if they have not been commenced or second dose of Adrenaline if 5 minutes have already passed since the first dose Reassess after 5 minutes of first dose of Adrenaline and if continuing signs of angioedema, bronchospasm and cardiovascular collapse: Commence titration of IV Adrenaline if the expertise is available (see box below). Intra osseus Adrenaline can also be used if the equipment is obtainable. If not repeat IM Adrenaline 0.5mg (or 0.5ml) of 1:1000 into the thigh muscle IV Adrenaline Titration – If expertise and facilities allow, careful titration of IV Adrenaline can be considered as an alternative route to IM adrenaline. Before administration, IV access must be secured, ECG monitoring attached and continual BP monitoring in situ. If the systolic BP is less than 80mmhg then IV titration can begin. Using a 1:10,000 solution, administer small increments of 1ml (100mcg) every one minute and observe the response. Do not give as a bolus but as a slow infusion using the hand held syringe. If BP does not respond to this after 3 minutes double the dose to 2ml (200mcg) every one minute. Continue until BP above 90 mmHg. Thereafter small 0.5ml doses may be needed to maintain BP above 90. Further dilution to 1:100 000 may be useful to allow finer increments doses. NB If adrenaline is causing any ventricular arrhythmias, chest pain or severe tachycardia >150 bpm or if the heart rate is above 150 bpm prior to adrenaline administration consider using the alpha agonist, IV Metaraminol 1mg – dilute the 10mg in 1ml ampoule with 9mls of water. It can be then be given in 1mg /1ml increments every 2 minutes until the blood pressure rises above 90 mmHg If angioedema (A) persists consider nebulised adrenaline 1mg, i.e. 1ml of 1:1000 mixed with 5ml Normal Saline. If no improvement consider early intubation by a skilled practitioner – it may be useful to use an ET tube that is 2 sizes smaller due to obstructive swelling If bronchospasm (B) is still persisting, administer salbutamol 5mg nebulizer and monitor heart rate - treat as an asthmatic emergency Continue to assess cardiovascular collapse (C) – IV adrenalin should be being titrated but if resources do not allow, i.e. a community setting a third IM dose of Author: Resuscitation Co-ordinator Authorised By: Chief Executive Date of first approval: November 2008 Date last review completed: November 2008 Page:5 of 9 Sponsor: Clinical Board Name: Anaphylaxis Policy IM Adrenalin 0.5mg (or 0.5ml) of 1:1000 may be repeated after 5 minutes from previous dose If hypotension continues administer an H2 antihistamine – IV Ranitidine 50mg slowly. The patient’s condition can deteriorate rapidly into P.E.A cardiac arrest. There can be a delay in recognizing this as the cardiac monitor will still show electrical activity. The patient however will have no output and no pulse, and be in cardiac arrest. If patient becomes unresponsive, commence standard NZRC collapse guidelines using the ABCDE approach. If patient is unresponsive, with no breathing and no circulation commence CPR – 30 chest compressions/ 2 ventilations If cardiac arrest occurs: In addition to standard guidelines Elevate the legs Give early escalating doses of IV adrenaline. Give 1mg of Adrenaline initially and then double every 3 minutes until 4mg reached and continue – 1mg, 2mg, 4mg, 4mg… Insert 2 large bore cannulae and administer 2-4 litres of Normal Saline or 2 litres of colloid Give H1 and H2 antihistamines IV Give extended CPR - so that correction of hypovolaemia and vasodilation can be achieved If not responding to adrenaline consider boluses of Noradrenaline 4mg (2 x 2mg/2ml ampoules) to improve vasoconstriction LEGISLATION, STANDARDS AND POLICIES: New Zealand Resuscitation Council Guidelines 2006 TDH Cardiopulmonary Resuscitation policy TDH Safe use of Medicine policy Author: Resuscitation Co-ordinator Authorised By: Chief Executive Date of first approval: November 2008 Date last review completed: November 2008 Page:6 of 9 Sponsor: Clinical Board Name: Anaphylaxis Policy TRAINING: 1. Staff of TDH completing their CORE level 5–7 will update their knowledge of anaphylaxis every two years. 2. Independent learning sessions on anaphylaxis will be arranged at managers request OUTCOME STANDARDS: Staff of TDH will be able to deliver high standard of care, using current best practice guidelines while caring for patients experiencing anaphylaxis. EVALUATION METHOD: 1. All incidents resulting in an unexpected patient outcome will be reported using the TDH incident reporting mechanism and adherence / variance to this policy will be audited 2. Resuscitation audit forms will be completed for patients suffering severe reactions and sent to the Resuscitation Coordinator. These will be further considered by the Resuscitation Committees to be able to review practice Authorised By Date of Approval: November 2008 Next Review Date: November 2010 References: 1. Johansen SG et al – Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. Journal of Allergy and Clinical Immunology 2. New Zealand Resuscitation Council – Advanced Resuscitation for Health Professionals, February 2007 3. UK Resuscitation Council – Emergency treatment of Anaphylactic Reactions – Guidelines for health providers, January 2008 Author: Resuscitation Co-ordinator Authorised By: Chief Executive Date of first approval: November 2008 Date last review completed: November 2008 Page:7 of 9 Sponsor: Clinical Board Author: Resuscitation Co-ordinator Authorised By: Chief Executive Name: Anaphylaxis Policy Date of first approval: November 2008 Date last review completed: November 2008 Page:8 of 9 Sponsor: Clinical Board Author: Resuscitation Co-ordinator Authorised By: Chief Executive Name: Anaphylaxis Policy Date of first approval: November 2008 Date last review completed: November 2008 Page:9 of 9