09_fois06
advertisement

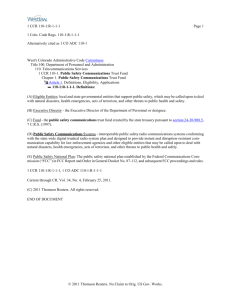
The Image as Spatial Region: Location and Adjacency within the Radiological Image James M. FIELDING a,b,1, Dirk MARWEDE a,c a Institute for Formal Ontology and Medical Information Science, Saarland University, Germany b Centre for the Study of Pragmatism and Analytic Philosophy, University of Paris I, France c Department of Diagnostic Radiology, Leipzig University Hospital, Germany Abstract. Biomedical ontologies define entities and relations in order to represent knowledge in the biomedical domain. In this paper we concentrate on the domain of medical imaging. In previous work, we analyzed a representative sample of computed tomography reports in order to determine to which entities and relations the terms used in such reports refer (with regard to the Foundational Model of Anatomy (FMA) and the recently published Open Biomedical Ontology (OBO) Relation Ontology, respectively) in order to construct an imaging ontology for electronic reporting in radiology. In this paper we expand the role of two OBO relations in particular, as they may be applied to radiological image information: the relations located_in and adjacent_to. Defining these relations in terms of the basic topological relations of Region Connection Calculus (RCC), we show how the qualitative description of image feature locations in radiological reporting may be formalized for reasoning. Keywords. Biomedical Ontology, Radiology, Imaging, Qualitative Spatial Reasoning. 1. Introduction In previous work [1], we analyzed a sample of typical CT reports to determine the entities and relations referred to there (with regard to the Foundational Model of Anatomy (FMA) [2], and the OBO Relation Ontology [3], respectively). On the basis of this work, and the ontological principles of Basic Formal Ontology (BFO) [4], we created a prototype application ontology, called RadIO [5], for the electronic management of radiological reporting, capable of integrating the RSNA’s RadLex lexicon [6] with the canonical anatomical knowledge of the FMA. In this application ontology, we supplemented the OBO relations with a set of radiology-specific relations for ascribing image features like shape, morphology, size and signal to the entities appearing in these images. However, since these relations were generally hold between entities and their atomic properties, the reasoning capability afforded was minimal at best. In what follows, we return to the domain of medical imaging, adapting the OBO relations of located_in and adjacent_to to the two-dimensional realm of the 1 Corresponding Author: James Fielding, IFOMIS, Universität des Saarlandes, Postfach 151150, D66041 Saarbrücken, Germany; Email: matthew.fielding@ifomis.uni-saarland.de. radiological image, in order to demonstrate how these relations may afford a significantly greater degree of reasoning in the imaging domain. 1.1. Clinical Radiology Radiology departments nowadays are highly computerized environments. Apart from the image acquisition process, images are reconstructed after acquisition (postprocessing techniques), stored in huge database repositories (or PACS, picture archiving communication systems), and distributed within networks which allow the images to be displayed on dedicated workstations to the radiologists or clinicians in remote locations. Radiologists interpret these images and dictate a report of their findings, in recent times via speech recognition software. These reports are then stored in radiological information systems (RIS) as free-text. In general, little is known about the terminology used by radiologists, and consequently (despite the fact that these reports serve as the basis for the communication of diagnostic results across practitioners), the management of radiology reports has not been significantly affected by IT tools such as ontologies [7]. 1.2. Biomedical Ontologies Today, the word ‘ontology’ enjoys two different meanings. In the context of knowledge representation, ontology is frequently used to describe concepts modeled in a specific domain and the relations which are supposed to exist between those concepts. In the context of philosophy, ontology is concerned with the types of entities existing in reality and with the relations that exist between these types and their corresponding instances. From this philosophical point of view, the representation of entities and relations in reality is not restricted to the definition of the concepts used by experts in a specific domain. These definitions employ a terminology specific to the domain in question, which only hinders the understanding of these concepts from a view outside of that domain, and thus the interoperability of the resultant ontology when interfaced with ontologies from other neighbouring domains. In order to realize interoperability, these various domain-specific application ontologies require a reference, according to the principles of which they are standardized; for example, the FMA, which may be commonly applied across the various biomedical subdomains that require recourse to anatomical knowledge. This distinction between application and reference ontologies applies not only to entity types, but to relations as well. One major obstacle to the interoperability of currently existing ontologies is that, to date, no standard set of formal ontological relations has been universally accepted. Within the Open Biological Ontology framework (OBO), however, a set of top-level ontological relations has recently been published to address this problem. These relations give ontology researchers the tools required for the development and integration of biomedical ontologies: clear definitions for a set of relations commonly applicable throughout the biomedical domain. 2. Ontological Foundations of the Medical Imaging Domain 2.1 Types and Instances The term ‘type’ is here used to refer to what in the knowledge representation community is occasionally expressed under the heading of ‘concept’ or ‘class’ and what in the philosophical literature are called ‘universals’ or ‘kinds’. A type is that which is general in reality. By contrast, instances are those things that are particular individuals. Instances exist in time and space and relate to each other in a variety of instance-level relations. The type abdomen is a universal in the biomedical domain; an instance of this type is the particular abdomen of a particular patient at a particular time and place. Similarly, the type image of abdomen is a universal in the biomedical imaging domain; an instance of this type is a concrete image that can be viewed and described in its particular reality. 2.2. Continuants and Perdurants Continuants and processes are two sorts of entities that relate in different ways to time [4]. Continuants are those entities that continue through time, wholly present at each moment of their existence. Examples of biomedical continuants are entities such as organs, cells, and medical devices, as well as their properties. Examples of biomedical image continuants are static images of the lung, or liver, etc, but also the particular properties present in these images such as colour patches, or image shadows. Processes, on the other hand, are those sorts of entities that are never fully present at any one moment in time, but instead unfold themselves in successive phases or temporal parts. Entities such as these, which perdure through time, are events such as the heart’s pumping of blood, a surgery session, or the many processes by which an image of the human body is attained, such as the application of x-rays. In our current work, we deal only with static images, although in principle, such an analysis could extend to dynamic video as well. 2.3. Fiat and Bona Fide Entities Not all the boundaries between entities in reality correspond to some absolute determinable location, such as the boundary between one’s teeth, between the lungs and mediastinum, or between one kidney and another. In biomedical reality, the boundaries between many entities and regions do not always correspond to any genuine qualitative or numeric change; as Germany and France have been divided from one another by political agreement, so too have the exact boundaries between the right pulmonary artery and truncus pulmonaris, for example, been established by the convention of medical practitioners. With entities of this sort, given any particular region at some arbitrarily small level of granularity, it may not be possible to determine whether this region belongs to one entity or the other; however, (like Germany and France) this does not mean that there exists no real boundary between them. Following [8], we call entities and boundaries of the first type bona fide, and entities and boundaries of the second type fiat. 2.4. The Radiological Notion of ‘Finding’ The assertions made by a radiologist when reporting, for example ‘normal liver,’ signify that the liver in an image appears to be normal. This is particularly important to note since not all pathologies are susceptible to all imaging techniques at all times (cancer on the cellular level, for example), and a liver that appears normal in an image may not in fact be so. The ways bodily entities appear on the image depend on the imaging technique applied, and the right technique must be applied to return the proper results; a lung imaged with magnetic resonance (MRI), for example, appears differently than the same lung imaged with a computed tomography (CT). In the context of reporting imaging observations, radiologists have introduced the notion of finding for any appearance that is not considered normal. In radiological practice, a finding can range from simple features like density or shape to highly interpretative diagnoses like pneumonia or malignant neoplastic tumour [9]. Independently of how radiologists look at body entities projected on an image, or what techniques are employed, it is necessary to make the distinction between these two domains of reality explicit: the domain of the body and the domain of the image. 2.5. Image Entities The ontological category of image entity is our solution to this distinction. Image entities, like all other entities, are divided according to the type/instance (i.e. universal/particular) and continuant/perdurant (i.e. static/dynamic) distinctions. Similarly, they are susceptible to both bona fide and fiat boundaries. In our radiological image ontology, we distinguish three image entity types: anatomical image entity, pathological image entity, and visual feature. Anatomical Image Entity. Most terms found in radiology reports referred to the appearance of anatomical entities. These terms include those referring to the appearance of bona fide anatomical entities, i.e. those entities physically delimited by the object itself, like anatomical structures such as organs and some organ parts (e.g. lung, or left lung), anatomical spaces (e.g. thoracic cavity, perirenal space), and body substances (e.g. blood). Also included are terms that refer to the appearance of fiat entities, i.e. entities which reflect human demarcation, such as some organ parts (e.g. liver segment) and body regions (e.g. upper abdomen). The anatomical image entities of this category are images of those types of entities typically represented in canonical anatomy ontologies such as the FMA. Pathological Image Entities. The non-anatomical image entities referred to in radiology reports are of two sorts: 1. the appearance of pathological structures and spaces, and 2. the appearance of biomedical artifacts such as medical devices and implants. Of the pathological sort, are terms referring to the appearance of pathological structures (e.g. tumour), substances (e.g. pleura effusion), and spaces (e.g. bulla). The corporeal entities that correspond to the image entities in this category are those typically represented within disease classification systems like SNOMED-CT [10] or the International Classification of Diseases (ICD) [11]. Image Features. Image features are visual properties of anatomical and pathological image entities that further qualify them. Terms such as ‘round,’ ‘large,’ or ‘dense,’ are used by radiologists to describe the various visual characteristics of entities as they appear in the image. It is on the basis of these features that a radiologist interprets an image and asserts whether it indicates a normal or pathological condition. 3. OBO and RCC Relations Applied to the Radiological Image In our previous work, we have shown that a number of radiology-specific relations can be provided (in particular, the relations has_shape, has_size, has_composition, has_coordinate, and has_signal). However, since these relations are generally used solely for ascribing atomic properties to image entities, their reasoning capacity is severely limited. Despite this limited reasoning capacity however, applying the OBO relations of located_in and adjacent_to to the imaging domain, we may define these relations in terms of the basic set of definitions of Region Connection Calculus (see, for example, [12]). These definitions may subsequently be used for reasoning about the specific location and orientation of 2D image entities. 3.1. OBO Primitive Relations Not all relations can be defined, for otherwise we risk infinite regress. Hence, some relations have been declared as primitive in the OBO framework; these relations are domain-neutral, and as far as possible, self-explanatory. This category includes relations such as has_part, has_participant, has_agent, and derives_from, among others. The two primitive OBO relations most frequently found in the reports we examined are located_in and adjacent_to. In the radiological domain, these relations are most frequently used to relate pathological image entities to the anatomical image entities that serve as their ‘host,’ and thus form a large portion of the information required by radiologists. The relation of located_in is formulated in the OBO framework as follows: c located_in r at t: a primitive relation between a continuant instance and a spatial region which it exactly occupies at a time. As stated in the OBO documentation, this relation thus ‘reflects the fact that each continuant is at any given time associated with exactly one spatial region, namely its exact location,’ though this may subsequently be expanded to include location relations holding between two continuant instances or two spatial region instances. As with the OBO framework, we have adapted this basic location relation to hold between spatial regions located within each other; however, in our adaptation this relation holds independently of time, as the image is in fact a “snap-shot” and does not change relative to this time. The relation of adjacent_to is formulated in the OBO framework as follows: c adjacent_to c1 at t: a primitive relation of proximity between two disjoint continuants at a time. Adapting these relations to the biomedical imaging domain allows us to define a set of more specific relations that fall under these as subtypes. For example, the image of the lumen of the right pulmonary artery in a radiograph such as a CT-scan (see Image 1) forms an extended space, which passes out of the space of mediastinum and into the space of the right lung. Defining a set of more specific location relations, allows us, for example, to specify the exact location of the thrombus referred to above in relation to either the mediastinum or the right lung, or both. 3.2. RCC Basics RCC is based on a single primitive: the ‘connection’ relation (C). At its most basic level, this relation is reflexive and symmetric, formalized as follows: xC(x,x) x,yC(x,y) C(y,x) reflexivity: all spatial entities are connected to themselves symmetry: if x is connected to y, then y is connected to x Additional relations that may hold between two regions may be defined in terms of C using the following simple set of definitions: DCxy = def. C(x,y) Pxy = def. z[C(z,x) C(z,y)] Pixy = def. Pyx PPxy = def. P(x,y) & P(y,x) EQxy = def. P(x,y) & P(y,x) Oxy = def. z[P(z,x) & P(z,y)] DRxy = def. O(x,y) POxy = def. O(x,y) & P(x,y) & P(y,x) ECxy = def. C(x,y) & O(x,y) TPPxy = def. PP(x,y) & z[EC(z,x) & EC(z,y)] TPPixy = def. TPPyx NTPPxy = def. PP(x,y) & z[EC(z,x) & EC(z,y)] NTPPixy = def. NTPPyx x is disconnected from y x is part of y Inverse of Pxy x is a proper part of y x coincides with y x overlaps with y x is discrete from y x partially overlaps y x externally connects with y x is a tangential PP of y Inverse of TPPxy x is a non-tangential PP of y Inverse of NTPPxy This set of definitions provides the foundation for what is known as the ‘RRC-8’ set, comprising PO, TPP, NTPP, EQ, TPPi, NTPPi, EC, and DC (cf. Fig. 1). As these relations provide a basic foundation for reasoning about spatial regions, we focus our efforts here. Subsequent work will involve expanding this set to include more complex relations, and validating the utility of these formalisms for the imaging domain. The upper part of Figure 1 shows the subsumption lattice of possible relations holding between pairs of regions, all of which are definable purely in term of C; these lines connect the set of more restrictive relations (lower) to more inclusive ones (higher). For example, two regions standing in the mid-level relationship DR (i.e. are discrete from each other) can stand in either of the two more expressive, lower-level relations EC or DC (i.e. external connection or disconnection). The middle part of Figure 1 shows the standard graphic representation for each of these relations defined for two regions, a and b. C O P Pi PP PO TPP a b a PO(a,b) NTPP b TPP(a,b) a b NTPP(a,b) PPi EQ DR NTPPi TPPi EC a b a b a b a b EQ(a,b) NTPPi(a,b) TPPi(a,b) EC(a,b) DC a b DC(a,b) Located_In Adjacent_To Figure 1. Subsumption hierarchy with graphic interpretations of the basic RCC-8 relations and OBO alignments 3.3. RadIO-Varieties of the Located_In and Adjacent_To Relations The bottom part of Figure 1 shows the relationship classes of our adaptation of the RCC relations to the OBO relations of located_in and adjacent_to; we call these relations ‘RadIO-varieties’ to highlight the fact that these are not anatomical in the strict sense of the word, but apply only to the spatial regions of the image and not to the anatomical entities themselves. (A tumour, located in the right lung, for example, could never be defined as a part of the right lung, but the spatial region occupied by the tumour in an image would be a proper part of the spatial region occupied by the image of the right lung.) In our radiological adaptation of the basic RCC-8 relations, TPP, NTPP, NTPPi (the inverse of NTPP) and TPPi (the inverse of TPP) belong to RadIO specifications of the located_in relation, and the relations of PO, EC, and DC belong to the RadIO specifications of the adjacent_to relation. While these RadIO specifications do not themselves play any role in the ontology’s spatial reasoning (this is properly left to the RCC relations), they do provide a platform for integrating applications that have need or spatial reasoning (such as RadIO) with other applications also conforming to the OBO standard that do not (and thus still have recourse to the OBO location and adjacency relation). These specifications require that we adapt the basic OBO location relations to reflect the specific ontological structures of the two-dimensional image entities which are our concern here. For instance, because all image entities are of a homogeneous structure no matter what they represent (even hollow spaces such as the lungs are as solid as any other anatomical image entity, ontologically, it is only their signal values that differ), our radiological version of the location relation holds not between a continuant entity and a spatial region which it occupies (as the definition above states), but rather between one continuant image entity and another, so that: An image entity c is RadIO_located_in another image entity c1, when the RCC parthood relation holds between the spatial region r, exactly occupied by the continuant image entity c, and the spatial region r1, exactly occupied by c1, independently of time. We formalize this relation as follows: c RadIO_located_in c1 =def. r, r1 (c located_in r & c1 located_in r1 & P(r,r1)) While the adjacent_to relation (as holding between continuant entities of all sorts) can be imported into the two-dimensional realm of the radiological image quite naturally, we still need to account for a few of the fundamental differences implied in the imaging domain. First, the OBO relation of adjacency states above that two continuants standing in this relation are disjoint; while this definition holds for continuant image entities as well, it is somewhat different for the spatial regions which they occupy. Since spatial image regions are created by projecting three-dimensional entities upon a two-dimensional surface, the spatial regions of properly disjoint entities may in fact overlap in the image (i.e., share a part), although they do not do so in reality. To account for this, we are required to generalize the notion of adjacency to include those cases where overlapping of spatial region occurs in the image, so that: An image entity c is RadIO_adjacent_to another image entity c1, when the RCC parthood relation holds between neither of the regions r or r1, exactly occupied by c and c1, and c is adjacent to c1 or r and r1 overlap (i.e. there is a third region r2 which stands in the RCC parthood relation to both r and r1), independently of time. We formalize this relation as follows: c RadIO_adjacent_to c1 =def. r, r1(c located_in r & c1 located_in r1 & (P(r,r1) v Pi(r,r1)) & c adjacent_to c1 v PO(r,r1))) In addition, note that the definition of the OBO adjacent_to relation states that adjacency is ‘a relation of proximity’ and (since this relation is primitive) there are no criteria for determining exactly how proximal two entities must be in order to satisfy this relation. Thus, where the location relations in the RadIO_located_in come more or less for free, the definition governing the RadIO_adjacent_to intrinsically requires that the OBO adjacency relation already holds (unless PO holds, as we have defined this relation). The OBO adjacency does we indeed come for free in the case of the RCC relation of external connection (what connects, but does not overlap, must be adjacent), and as we have seen we can expand our radiological definition of adjacency to include overlap; however, we cannot infer adjacency from the RCC relation of disconnection. Two disconnected regions may or may not be adjacent, and this can only be determined by the examining radiologist based on entities in question, the normal position in which they stand, and the context under which the examination was performed. We qualify this relation therefore with the following disjunction: c RadIO_adjacent_to c1 r, r1 ((c located_in r & c1 located_in r1) & ((PO(r,r1) v EC(r,r1) v (DC(r,r1) & c adjacent_to c1)))) Providing RCC-varieties of the adjacency relation proved slightly more difficult than the location relation, mainly due to ambiguity in the type of language we use to ascribe adjacency, which could be used to describe an image entity’s orientation with or without connection (perhaps a thin membrane or other anatomical boundary separates them), and in some cases, with a partial overlap, where the regions remain distinct enough so as not to be ‘located in’ exactly, but are situated in a proximate space. For a formalism defined in terms of ‘connection,’ these details hold a heavy ontological weight: therefore, attributing adjacency in our application ontology, a radiologist will be required to specify which of these important distinctions holds. 3.4. Reasoning with RCC and Radiological Images The main reasoning mechanism used by RCC is the composition table, containing information about the transitive closure of RCC relation pairs. The composition table for RCC-8 is shown in Table 1. Given three spatial regions, a,b, and c, and two RCC relations, R1 and R2, such that R1(a,b) and R2(b,c) holds, the composition table can be used to determine R3, the set of RCC relationships that may hold between regions a and c. In cases where several alternative relationships might hold, the composition table entry represents a disjunction of these relations. R2(y,z) DC EC PO TPP NTPP TPPi NTPPi EQ R1(x,y) DC no info DR, PO, PP DR, PO, PP DR, PO, PP DR, PO, PP DC DC DC EC DR, PO, PPi DR, PO, TPP, TPPi DR, PO, PP EC, PO, PP PO, PP DR DC EC PO DR, PO, PPi DR, PO, PPi no info PO, PP PO, PP DR, PO, PPi DR, PO, PPi PO TPP DC DR DR, PO, PP PP NTPP DR, PO, TPP, TPPi DR, PO, PPi TPP NTPP DC DC DR, PO, PP NTPP NTPP DR, PO, PP no info NTPP TPPi DR, PO, PPi EC, PO, PPi PO, PPi PO, TPP, TPPi PO,PP PPi NTPPi TPPi NTPPi DR, PO, PPi PO, PPi PO, PPi PO, PPi O NTPPi NTPPi NTPPi EQ DC EC PO TPP NTPP TPPi NTPPi EQ Table 1. RCC-8 Relational Composition Table 4. Informed Reporting via the Imaging Domain Ontology Reporting on anatomical image entities can be performed by evaluating an anatomical image entity as normal, or by describing visual features and pathological image entities located in these anatomical image entities and interpreting those observations. In this section, we take a typical example from the biomedical imaging domain. We demonstrate how the location and orientation of the image entities contained there may be qualitatively described by radiologists and how these may subsequently be used for spatial reasoning concerning the entities involved. 4.1. Example: Acute Pulmonary Embolism Image 1 is one of a series of CT image slices taken from the thorax, a few centimeters above the heart. A typical free-text report documenting these findings, might read something like: Central subtotal thromboembolism with a large thrombus located in the right pulmonary artery and the left lower lobe artery extending through almost the full diameter of the vessels. Bilateral pleural effusion, predominantly on the right side. Degenerative change of the thoracic spine. 1 Truncus pulmonalis 2 Aorta ascendens 3 Aorta descendens 4 Right Lung 5 Left Lung 1 5 2 6 Right pulmonary artery 7 Thrombus in the right pulmonary artery. Thrombus in the left lower lobe pulmonary artery. 8 9 Pleural effusion 10 Thoracic vertebral body. Table 2. Continuant image entities of Image 1. 4 7 6 8 3 10 9 Image 1. CT-Scan of the thorax showing the pulmonary arteries with embolism In our ontology-based report manager, the radiologist, having specified that a thrombus is located in the right pulmonary artery, would be given a series of more specific RCCvariety location relations to choose from (namely, PP, PPi, TPP, TPPi, NTPP, or NTPPi), further specifying the exact location of the thrombus with regard to the right pulmonary artery, at which point, the examining radiologist would in this case select TPP (tangential proper part). This statement would be formalized as follow: TTP(thrombus, right pulmonary artery) a b Since the right pulmonary artery extends beyond the boundaries of the mediastinum into the right lung however, we may determine the location of this thrombus more specifically with regard to the lungs. Given that: c PO(right pulmonary artery, right lung) b From the RCC-8 composition table, we can infer that one of the following relations will hold: a a i) DR(thrombus right lung), or ii) PO(thrombus, right lung), or iii) PP(thrombus, right lung). a c b (i) c b (ii) c b (iii) In other words, the thrombus is either discrete from, partially overlapping with, or a proper part of, the right lung. At this point, the radiologist will be given this selection of possible relations for further specifying the exact location of the thrombus in regard to the right lung – in this case, partial overlap – because some part of the thrombus is located in the region of the lung and some part in the region of the mediastinum, which distinguishes the location of this thrombus from that of the thrombus located in the left lower lobe artery, which is a proper part (i.e. completely contained within the region) of the left lung. 5. Conclusion This paper presents the foundations for developing a robust theory of qualitative spatial location appropriate for reasoning with information about radiographic images. We have shown how the image may be divided up into discrete image entities (anatomical and pathological image entities), and a set of qualitative RCC-based spatial relations that may hold between these entities (connection, parthood, overlap, etc.). The RCC relations are additionally grouped around a pair of primitive OBO relations, located_in and adjacent_to. Adopting the RCC framework for reasoning with these relations and entities allows us to determine additional information about the location and orientation of these entities, information which may not be explicitly provided by radiologists when annotating images in their reports, expanding the scope of our application ontology and the type of information that may be contained therein. Grouping these RCC relations around standard OBO relations provides a platform for integrating applications which require spatial reasoning (like RadIO, presented in part here) with those that do not, while contradicting the principles of neither. Acknowledgements The present paper was written under the auspices of the Wolfgang Paul Program of the Alexander von Humboldt Foundation, the Network of Excellence in Semantic Interoperability and Data Mining in Biomedicine of the European Union, and the project Forms of Life sponsored by the Volkswagen Foundation. References [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] Marwede D, Fielding JM, Smith B. Entities and Relations in Medical Imaging: An Analysis of Computed Tomography Reporting. Forthcoming. Rosse C, Mejino JL, Jr. A Reference Ontology for Biomedical Informatics: the Foundational Model of Anatomy 5. Journal of Biomedical Informatics 2003 Dec; 36(6):478-500. Smith B, Ceusters W, Klagges B, Kohler J, Kumar A, Lomax J, Mungall CJ, Neuhaus F, Rector A, Rosse C. Relations in Biomedical Ontologies. Gnome Biology, 2005. Grenon P, Smith B, Goldberg L. Biodynamic Ontology: Applying BFO in the Biomedical Domain. Studies in Health, Technology, Information 2004; 1002:20-38. Marwede D, Fielding JM. RadiO: A Prototype Application Ontology for Radiology Reporting Tasks. Forthcoming. http://mirc.rsna.org/radlex/services Langlotz CP. Automatic Structuring of Radiology Reports: Harbinger of a Second Information Revolution in Radiology 6. Radiology 2002 Jul; 224(1):5-7. Smith B. Fiat Objects. Topoi: International Review of Philosophy 2001; 20(2):131-148. Bell DS, Pattison-Gordon E, Greenes RA. Experiments in Concept Modeling for Radiographic Image Reports. Journal of the American Medical Informatics Association, 1994; 1(3): 249-62. Spackman K. SNOMED RT and SNOMED CT. Promise of an international clinical terminology. MD Computing 2000 Nov; 17(6): 29. Parman CC. ICD-10-CM. Journal of Oncology Management 2004 Jan;13(1):8. Gotts NM, Gooday JM, Cohn AG. A Connection Based Approach to Common-Sense Topological Description and Reasoning. Monist 1996; 79(1): 51-75.