EXTERNAL Safety Report Submission Cover Sheet
advertisement

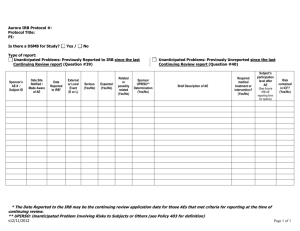
Hospital for Special Surgery ¤ Institutional Review Board EXTERNAL SAFETY REPORT SUBMISSION COVER SHEET Submit an original and 1 copy of the entire submission packet (inc. supporting documentation) Date HSS IRB#: Protocol Title: Principal Investigator: Sponsor: Sponsor Protocol#: IND/IDE # (if applicable): Safety Reports regarding events at sites other than HSS must be reported to the HSS IRB as follows: Drug: Adverse event is (1) SERIOUS and UNEXPECTED and ASSOCIATED WITH THE USE of the experimental study drug, or (2) an unanticipated problem involving risks to subjects or others. Device: Adverse event is unanticipated. **** To facilitate submission, you may list up to 10 separate EXTERNAL reports on this form. **** Please attach corresponding reports to this form. Date of Report Adverse Event Unique Identifier or Manufacturer’s Report # Are you requesting a consent revision as result of this report? [Must complete] Yes* No 1 2 3 4 5 6 7 8 9 10 *If you are requesting an informed consent form revision, you must specify language. Please provide a copy of the consent form with changes indicated. __________________________________________________________________________________ PI Signature Date IRB Reviewer Use Only IRB Requested Modifications (if any): No Requested changes as a result of this submission Jacques Yadeau, MD, PhD – ViceChairman, IRB Page 1 of 1 Date