Kenya National Plan (2005) - Avian Influenza and the Pandemic
advertisement
 - Avian Influenza and the Pandemic")
Table of Contents
INTRODUCTION AND BACKGROUND ..................................................... 1
BACKGROUND INFORMATION - DVS ...................................................... 1
Poultry Production Systems ........................................................................ 2
Situation Analysis ................................................................................... 2
PANDEMIC PREPAREDNESS .................................................................. 5
CO-ORDINATION AND RESOURCES MOBILISATION ................................. 10
EPIDEMIOLOGY AND SURVEILLANCE EMERGENCY PREPAREDNESS PLAN ... 17
EPIDEMIOLOGY AND SURVEILLANCE (DOMESTIC BIRDS) WORK PLAN ........ 20
EPIDEMIOLOGY AND SURVEILLANCE (HUMANS) WORK PLAN ................... 23
EPIDEMIOLOGY AND SURVEILLANCE (WILD BIRDS) WORK PLAN ............... 24
LABORATORY AND RESEARCH ............................................................ 29
INFECTION PREVENTION AND CONTROL ............................................. 37
CASE MANAGEMENT ........................................................................ 43
INFORMATION, EDUCATION AND COMMUNICATION ............................... 48
SUMMARY AVIAN FLU GUIDELINE ....................................................... 54
i
ii
Executive summary
1
ACRONYMNS AND ABBREVIATIONS
WHO
FAO
USAID
OIE
AU-IBAR
MOH
MOLFD
IEC
IPC
UNDP
DANIDA
1
THE NATIONAL AVIAN INFLUENZA STRATEGIC EMERGENCY
PREPAREDNESS AND RESPONSE PLAN
INTRODUCTION AND BACKGROUND
THE COUNTRY
The contemporary Republic of Kenya was founded on 12th December 1963 when the country
gained her independence. It lies on the eastern part of the African continent East Africa and is
bisected by the Equator. It covers an area of some 582,000 Sq Km and has a human population
of 32 million persons. It is classified as a developing country and is characterized by a continuing
search for solutions to problems of poverty, ignorance and disease inherited from the past and
exacerbated by a plethora of international and local circumstances that are sometimes beyond its
capacity to resolve fully at the present time. At the international level some of the problems arise
from disadvantaged historical position in trade, investment, finance, development and political
economy. At the nationnal level, problems have arisen from leadership and governance systems
that leave quite some room for improvement. The country has however continued to grapple
with these problems and has received tremendous support from the international community
while still addressing local level problems in all sectors of the economy, health included, in order
to ensure a better future for its contemporary citizens and residents and visiters and for posterity.
BACKGROUND INFORMATION - DVS
THE DISEASE
Avian influenza is a viral disease of poultry caused by RNA viruses. There are three main groups
of influenza viruses: Type A, B, and C. Avian variants of influenza virus are classified as type A.
These naturally occur in domestic fowls, ducks, geese, turkeys, guinea fowl, quail and pheasants.
Disease outbreaks occur most frequently in domestic fowl and turkeys. Influenza B and C viruses
are generally restricted to humans. Influenza A viruses are widespread in birds and mammals
although most avian and other non-human variants do not infect humans.
There are two known pathotypes of Avian Influenza:
Highly Pathogenic Avian Influenza (HPAI)
This pathotype causes severe disease with high mortality of up to 100%.
To date, only (but not all) viruses of H5 or H7 subtype are in this pathotype
1
Low Pathogenic Avian Influenza (LPAI)
mild respiratory disease, depression, egg production problems
may exacerbate other infections/conditions
Influenza A viruses infecting poultry can be divided into 2 distinct groups. The most virulent
viruses cause fowl plague, now referred to as highly pathogenic avian influenza (HPAI) while
other viruses cause a milder, primarily, respiratory disease designated low pathogenic avian
influenza (LPAI). HPAI can cause up to 100% mortality. LPAI may under certain conditions
cause a more serious disease depending on environmental conditions and other concurrent
infections.
Most outbreaks in domestic poultry probably start with direct or indirect contact with water birds
and migratory birds in which the disease is inapparent. Many of the strains that circulate in wild
birds are either non pathogenic or mildly pathogenic for poultry and may become virulent
through either genetic mutation or re-assortment. 0nce AI is established in domestic poultry, it is
a highly contagious disease and wild birds are no longer essential for spread. Infected birds
secrete the virus in high concentration in their faeces, nasal and ocular discharges. Within a flock,
the disease spreads rapidly by direct contact and airborne transmission. The virus is then spread
from flock to flock by the usual methods involving the movement of infected birds,
contaminated equipment, egg cartons, feed trucks, human traffic and airborne transmission for
birds in close proximity. There is a possibility of vertical transmission though this has not been
resolved.
Clinical signs are variable and are influenced by factors such as virulence of the infecting virus,
species affected, age, sex, concurrent disease and environment. In HPAI, infected birds show
signs of depression, inappetence, ruffled feathers, fever, cyanotic and oedematous combs and
wattles, profuse watery diarrhoea and respiratory distress. Neurological signs may also be
observed.
VIRULENCE OF AVIAN INFLUENZA VIRUSES
• The presence of multiple basic amino acids at the HAO cleavage site means the viruses
are able to spread systemically in all tissues
• Without additional basic amino acids at the cleavage site the viruses are restricted to
replication in the respiratory and intestinal tracts
Poultry Production Systems
The poultry population in Kenya is estimated at 30,000,000, 80% of which are indigenous
chicken under backyard production, 19% commercially reared broilers and layers, and 1% made
up of other poultry (ducks, turkeys, geese etc). Commercially poultry keeping is mainly practiced
in urban and peri-urban areas of the country. On the average, every rural Kenyan household has
2-3 backyard chicken.
Poultry is mainly kept for supply of domestic protein, income generation and for social purposes.
Situation Analysis
Avian influenza has not been diagnosed in Kenya. However, Kenya is at high risk because it lies
along the migratory route of birds from Europe to Southern Africa and its water points serve as a
stop-over. Virus excreted by these birds can survive in the environment for long, especially in
ponds, waterways and cool damp areas.
However, the low population of intensively farmed turkeys, ducks or water fowls reduces the risk
of spread of the virus if introduced. In contrast, pigs and poultry are kept in close proximity and
thereby pose a public health risk.
2
Retrospective analyses of avian diseases diagnosed at the Central Veterinary Laboratory, Kabete
between 1935 and 2004 do not indicate the occurrence of avian influenza in poultry in the
country. Studies looking for heamagglutinating viruses in wild birds, water fowls, domestic and
indigenous chicken only showed presence of Avian Paramyxovirus (APMV) type 2 in migratory
birds, APMV type 2,3 and 8 in ducks, APMV type 3 in chickens and APMV type 4 in flamingos
(Kasiti J. L, MSc Thesis 2000).
Avian influenza was declared a notifiable in Kenya, with effect from 1996 through a gazette
notice. Following recent outbreaks in different parts of the world, Kenya has placed a ban on the
importation of poultry and their products from South Africa , Asia, Turkey, Greece, Romania
and any other country reporting avian influenza. Veterinary personnel at ports of entry have been
placed on high alert over possible entry of poultry and their products. A circular on disease
recognition and the need for prompt reporting of suspicious cases has been sent to all field
offices.
Kenya has an elaborate national epidemiological surveillance network comprising both public and
private veterinary professionals (veterinarians and paravets) and other stakeholders including
livestock keepers and traders. The public structures include District and Provincial offices,
Abattoir inspectorate, National and Sub-national Veterinary Laboratories and a Central
Epidemiology Unit. Other collaborators are Kenya Wildlife Services and Research institutions.
Though the National Veterinary Laboratory has some capacity to diagnose avian influenza, it
requires reagents, consumables, training and some equipment to be able to confirm avian
influenza cases. The Sub-national laboratories are poorly equipped for diagnostic work.
BACKGROUND INFORMATION - HEALTH
Kenya faces with a burden of communicable diseases that comprise 70% of all outpatient
morbidity. The country has adopted The Integrated Diseases Surveillance and Response (IDSR)
Strategy for the purpose of promptly detecting priority diseases, re-emerging and emerging
diseases. The country’s health system is beset with severe inherent weaknesses, among them the
following: Poor disease surveillance system (in terms of timeliness, completeness, human
capacity),
Inadequacy of emergency stocks of vaccines, anti viral drugs and protective gear &
other non-pharmaceuticals
Limited laboratory capacity
Inadequate funding for research
Past Influenza Pandemics
The following are milestones in the outbreak of influenza pandemics:
•Before 1880: Influenza was thought to be‘The Influence of Stars on epidemics of
Cough and Fever’
•1880-1933 : H. Influenza thought to be the causative agent for the disease
•1918:
Pandemic Alerts world on potentials of influenza
•1933:
First Isolation of influenza virus
•1946:
First Vaccine against influenza developed and tested in USA
•1947:
WHO: Establishment of first influenza Centre in London
Influenza pandemics are associated with high mortality, morbidity, social & economic disruption.
Deaths in pandemics are usually caused by Primary Viral Pneumonia and Pneumonia caused by
secondary Bacterial Infections. Three pandemics were reported in the 20th C at intervals of 103
50 years. The 1918 pandemic is regarded as the most deadly event in human history. It is
reported to have killed more than 40 million people in one year compared to total military deaths
of 8.3 million over 4 yrsof the First World war Most pandemics have originated from Asia where
humans live close to pigs and ducks.
The main challenge is provision of adequate hospital and medical facilities due to a surge in
medical care needsThe capacity of the virus to cause severe disease in ‘non traditional age groups’
e.g. young adults determines overall impact. Milder pandemics cause excess mortality in the very
young and old and in those with underlying chronic conditions (at risk groups for seasonal
epidemics). Countries with good vaccination programs expect better outcome due to experience
in logistics of vaccine delivery and conversely.
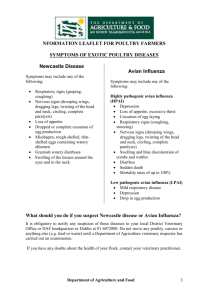
Influenza Surveillance
Influenza trend in Kenya Monitored by Surveillance Network in Nairobi
Nairobi
2001 - 03
flu +ve
25
20
15
flu +ve
10
5
N
ov
.0
1
F
eb
M
ay
A
ug
N
F ov
eb
.0
3
M
ay
A
ug
N
ov
0
Type ‘B’ constitute 94% of all detected cases while type ‘A’ 6%
Avian Influenza Risk Information
The main sources of avian Flu risk arises from importation of wild birds, poultry and their
products from affected countries, migratory birds flying from affected countries an international
tourism as Nairobi is a hub for international travel. This may be exacerbated by risk behaviour
inherent in local cultural practices such as consumption of inadequately cooked poultry and their
products, consumption of birds when signs of illness appear and living in the same dwellings
with poultry. These practices may expose our population to H5N1 virus infection.
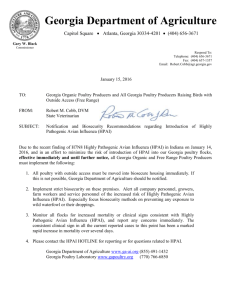
Kenya lies along the migratory birds route from Europe to Southern Africa and is a stop over
point for many species thereof. Birds start to arrive in mid September and peak in mid
November. Migratory birds stop at water points and mix freely with local water birds. Water
birds mix freely with domestic poultry. It is estimated that some 270 species of birds migrate
into Kenya. Kenya’s poultry population is estimate at 30 million of which indigenous birds
account for 70%, commercial birds 28% and others such as (geese, turkeys, ducks etc.) 2% of the
total bird population. The figure below shows the migratory bird routes.
H5N1Outbreaks in 2004 have become a major global concern since January 2004 when Thailand
and Vietnam reported their first case of human infection with avian Influenza previously
reported in chicken . These cases are directly linked to outbreaks of highly pathogenic H5NI
4
avian Flu reported in 2003. The fear is that the virus may improve transmissibility in humans and
therefore represents a serious pandemic in waiting.
H5N1 is mainly feraed for its documented ability to pass from birds to humans. It also has the
ability to cause severe disease conditions with high mortality (42/55 have reportedly died, and
only 13 recovered). It ha the undoubted potential to ignitea pandemic. Available vidence
indicates that H5N1 is now endemic in parts of Asia and the risk fis that the virus may expand its
range of mammalian hosts. For example the Oct 2004 outbreak in captive tigers and domestic
cats in Thailandin which some 147 tigers were affected. H5N1 is also being excreted by
asymptomatic ducks in highly pathogenic form maintaining silent transmission. Studies in the
outbreak for the first time show H5N1 strain can infect humans directly who serve as the mixing
vessel for exchange of virus genes. The first probable case of human to human transmission was
reported from in Thailand in December 2004.
Migratory Bird Flyways
Main issues facing Kenya’s Response system
The Kenyan response system is characterised by
Weak surveillance system
Inadequate support to laboratory
Inadequate human resources
inadequate research funding
Inadequacy of supplies of
Anti-viral drugs
Vaccines
Protective material
PANDEMIC PREPAREDNESS
Main objectives of the WHO global agenda for FLU are:•To strengthen the WHO Global influenza Surveillance Network
•To assess the burden of influenza and benefits of prevention and control
•To generate Global and National influenza pandemic preparedness
5
•To develop policies for influenza vaccine and antiviral usage during influenza pandemics
and epidemics
•To increase influenza vaccine usage and support acceleration of vaccine development
WHO urges all countries to develop/update their Influenza pandemic preparedness plans. It is
recognised that global spread is impossible to stop but preparedness will undoubtedly reduce
impact the final death toll. Planning should include estimates of the nunber of people to be
affected and likely deaths. Estimates of deaths are expected to range from 2-50 million based on
extrapolations from past pandemics.
National preparedness
National preparedness for the pandemic is being addressed from the vantage point of this
strategic preparedness plan which aims to facilitate mobilisation of resources needed to mount an
efficient and effective response. The plan has been developed by an ad hoc multi-sectoral task
force which has been set up to respond to the impending threat of the Avian Influenza outbreak.
The task force has followed WHO guidelines in developing the National emergency
preparedness and response plan
The plan focuses on the following issues:
1. Co-ordination, Resource Mobilisation and Human Resource Management
2. Epidemiologial Surveillance
3. Laboratory and Research
4. Case Management
5. Infection Prevention and Control
6. Information, Education, Communication and Social Mobilisation
The purpose of this plan is to mobilise resources and crystallise action to facilitate effective
surveillance, research, coordination, diagnosis, infection control, case management and
information dissemination and hence handling of the problem.
Main Assistance needed from the International Community
Response activities are coordinated by the multi-sectoral task force through its 6 technical
working groups. International community are partners in the National Avian Influenza MultiSectoral Task Force. The main forms of assistance expected from the international community
include :
Technical assistance and information
Mobilisation of resources and funding
International liaison & coordination
Harmonisation of monitoring and evaluation indicators
Strengthen at least one of the existing laboratories to the level of a regional Influenza
reference facility
ACTION TAKEN OR COMPLETED BY STAKEHOLDERS
Various stakeholders from the privare, pubic, civil society and development partner sectors have
taken, planned and/or contemplated some activities geared towards addressing the Avian Flu
problem among them the following:i)
Ministry of Health
Multisectoral Taskforce in place, formed during the first avian influenza WHO alert in
2004.
Integrated disease surveillance being implemented by the in all districts and will be
strengthened for influenza surveillance.
6
ii)
MOH in collaboration with KEMRI is currently undertaking the Flu surveillance through a
Flu surveillance network of private medical practitioners. This surveillance is limited in
Nairobi & will be expanded through additional sentinile sites.
Diagnostic laboratory capacity to identify the virus is available in the country at KEMRI.
Additional facilities will however be required.
An alert issued to all health facilities with instructions to start preparing isolation units
should need arise.
Treatment: There is currently no vaccine available for H5N1 virus strin.
The drug for treatment is Tamiflu but is not available in the country and supply not
adequate. Discussed with WHO to assist in availing it to the country
Infection Prevention and Control: Protective gear ordered in advance, but there is need to
establish requirements for the current response & gaps. Some materials available for normal
preparedness.
The workload in health facilities is anticipated to be very high. The health facilities should
be stocked with all necessities for response.
All ports of entry have been alerted. Wild birds would still migrate into the country with or
without immigration controls. Winter is approaching in Europe and birds are expected to
fly into the country.
Importation of poultry and poultry products will be contained through the ports.
KEMRI - the personnel is available, but need upgrading of the lab to protect staff.
Ministry of Livestock and Fisheries Development
Addressed a press conference on 18th October 2005 stating government position.
Mobilised all veterinary officials for a technical briefing on Avian Flu and actions required
of them.
Established a hotline for the public to ask questions on Avian Flu manned by technical
staff at Kabete. The Numbers are 020-631639 and 0722-726682
Prepared IEC materials for electronic and print media, for use in public education.
Assessed the laboratories at the headquarters and regionally to see whether they meet
surveillance requirements with requirements & costs.
Assessed the available veterinary expertise and found adequate
Assessed required funds and set priorities thus:.
1. Materials for professionals, media & public sensitisation;
2. protective clothing for professionals safety and
3. laboratory reagents that may cost Ksh 1 million
A Veterinary preparedness task force of 7 is meeting at Kabete and a vehicle has been made
available to it.
An AU-IBAR ymposium was held in Sept to inform stakeholders on the threat from Avian
flu and adopt a strategy to enable the region to cope. Country delegates were asked for
proposals on disease control and review of epidemiology. During the neeting it was
reported that:
Africa is estimated to have 1.1billion chicken population and 2% may get affected
and require to be culled.
An animal vaccine produced in China is available at the cost US$ 0.1 per bird.
Africa has had previous Avian Flu outbreaks; 8 outbreaks were recorded in South
Africa in 2004. Other countries include Egypt and Morocco.
University of Nairobi
There exists capacity for training at the University of Nairobi Faculty of Veterinary Medicine and
laboratory facility that may need some refurbishment and be available to flu surveillance.
7
ILRI
ILRI that has global operations is headquartered in Nairobi. ILRI has also set up a taskforce and
is currently compiling a synthesis of information from experiences in Asia that will be available
for information and knowledge in various websites.
On research, ILRI has capacity that could benefit Avian flu surveillance. GIS services could be
made available to map out areas where migratory birds land.
International Emerging Infections Programme (IEIP)
The US Embassy has set up a taskforce to check out what help could be made available. The area
of surveillance on humans and birds will be strengthened in early 2006. Some sites will be in
Nairobi, Mombassa, Western and Northern regions. Surveillance on migratory birds is expected
to start in November.
A recommended primary strategy is to avoid contact of migratory birds with flocks of domestic
birds. There should also be surveillance on birds deaths, an early warning sign.
The importance of strengthening communication cannot afford to be underexpressed. It is
essential to know about the work of neighbouring countries. CDC communicating with their
counterparts in neighbouring countries .Communication to health care workers on how to
suspect suspicious respiratory symptoms.
Kenya Red Cross Society (KRCS)
KRCS is a grass root organisation with 57 branches and 69,000 volunteers. It has strengths in
mobilisation and awareness creation and shall make available this social resource at the disposal
of the Avian Flu preparedness taskforce.
WHO
WHO is closely working with MoH. The DPC stressed that WHO is keen to collaborate with
MoH on strengthening surveillance for early detection of cases and the virus. WHO will support
in development of surveillance tools for avian influenza. This is a good opportunity for
strengthening integrated disease surveillance & response in the country.
As we are in the pre-pandemic phase, the influenza pandemic virus is still unknown and main
intervention strategy remainsto be rapid virus identification and stoppage of transmission.
WHO providing technical guidelines & provision of technical support from the Global alert
network
On stock pilling of anti–viral drugs, WHO is building strategic stocks, one million doses of
Tamiflu by end of 2005 and three million doses by end of March 2006 for use once an outbreak
diagnosed
Countries with resources can stockpile some, problem being low production.
FAO
FAO sent apologies through Mr. Langat. The organisation indicated support to the taskforce and
requested to be updated with all developments.
National Museums of Kenya – Ornithology Dept
NMK called for urgent measures to initiate monitoring the distribution of waterbuck & where
they at different times. However, resources minimal at the institution to undertake this exercise.
The migratory birds flying into the country arrive from September peaking in November. Some
flocks from European countries that could have been infected could start arriving in mid
November.
Sanofi Pasteur
The company has been supporting the Influenza Flu network for the last 5 years based on
sentinel sites of private medical practitioners. It has been established that Flu epidemic seasons in
8
Kenya are mainly from March to July and again in a less scale in November. Dr. Mwangi
underscored the need and urgency to scale up the surveillance network.
The company has in stock the inter-pandemic vaccine in the country.
9
CO-ORDINATION AND RESOURCES MOBILISATION
VISION
An adequately and effectively coordinated emergency preparedness and response to avian
influenza and pandemic flu.
MISSION
To ensure an effective emergency preparedness and response system is in place.
OBJECTIVES
1. To set up and strengthen the National Secretariat for Avian Influenza.
2. To oversee and coordinate the activities of the sub-committees of the National Avian
Influenza Task Force.
3. To mobilize required resources locally, regionally and internationally.
4. To coordinate international communication and dissemination of vital information and
give periodical updates on Avian Influenza in Kenya.
5. To ensure that a country emergency preparedness and response plan is in place and
implemented.
6. To monitor and evaluate the implementation of the country preparedness plan.
SITUATIONAL ANALYSIS
A multi-sectoral Task Force was set up encompassing all the major stakeholders. The
membership of this Task force is as follows:
1. Ministry of Health
2. Ministry of Livestock and Fisheries
3. Ministry of Special Programmes- Office of the President.
4. WHO
5. African Union-International Bureau of Animal Resources (IBAR)
6. Ministry of Finance
7. UNDP
8. Centre for Disease Control
9. USAID/Kenya
10. Walter Reed Project
11. Faculty of Veterinary Medicine-UoN
12. Ministry of Tourism and Wildlife
13. Disaster Management Unit-MOH
14. International Livestock Research Institute
15. National Museums of Kenya
16. Sanofi Pasteur
17. KEMRI
18. Centre for Virus research- Flu surveillance Network
19. UoN-Department of Community Health
20. Department of Immigration
21. Kenya Wildlife Services
22. UNICEF
23. Kenya Red-Cross Society
The task force has established 6 subcommittees. These are:
1.
Epidemiological Surveillance Committee
To screen birds and humans to determine whether the disease is present in the country or not. Its
activities include the following:10
Carry out targeted surveillance in domestic birds and animals.
Carry out targeted surveillance in wild birds (migratory & resident)
Strengthen active surveillance.
Carry out prompt outbreak reporting and investigations
Focus surveillance on high-risk groups.
Train health workers on disease surveillance especially Avian Influenza.
2.
Information, Education, Communication and Social Mobilization committee
It ensures that timely and useful information on avian flu is disseminated to the public and all the
stakeholders in health. Currently it is working with districts so as to get the information to
grassroots levels.
3.
Case Management Committee
It has the responsibility of setting up clear guidelines on the treatment of sick people in case the
pandemic occurs. It should also strengthen hospitals (especially referral ones) to improve their
capacity to meet the challenge. Its greatest task is to procure anti-viral drugs (Tamiflu) in
readiness for any outbreak in humans. Bird handlers and health workers are especially at high risk
of infection.
Its immediate activities include: Purchase of Antiviral drugs (Tamiflu) for at least 2000 people.
Purchase of protective clothing for the high risk groups.
Purchase non-pharmaceutical commodities (e.g. gloves, cotton wool, needles,
syringes)
4.
Laboratory and Research Committee
It has the responsibility of collecting and testing specimens from birds and humans for avian
influenza infection. This will help in diagnosis of the disease and further research.
Its immediate activities include the following: Upgrade KEMRI human influenza laboratory and Central Veterinary Laboratories
to BL3 level.
Buy reagents for both laboratories.
5.
Infection Prevention and Control Committee
Its responsibility is to prevent entry of the virus into the country and respond appropriately
should entry occur. The immediate activities include the following:
Establish quarantine facilities for birds and humans at the ports of entry.
Procurement of protective gear (for both health workers at institutions & veterinary
workers)
Purchase of disinfectant for use in contaminated areas.
Culling of birds once infection is detected to prevent spread.
Work with the office of the Attorney General on the review of laws on
compensation after the culling of birds.
Purchase of the seasonal flu vaccine.
Control of movement of poultry
6.
Co-ordination and Resource Mobilization Committee
It coordinates all the other committees. It also has the responsibility of mobilizing resources
(Both financial and human). It also supports the secretariat of the task force.
Its immediate activities include the following:-
11
Establish logistics for proper communication of the task force- purchase stationery,
computers, printers, scanners e.t.c and cater for the upkeep of the secretariat.
Coordinate transport for the task force- procure 2 vehicles especially for disease
surveillance, fuel and drivers’ upkeep.
A secretariat of the National task force is in place.
Both the ministry of health and the ministry of livestock and fisheries development have teams in
place dealing with the specific coordination of AI activities in their respective departments. These
ministries also have technical capacity to handle Avian Influenza activities. However this
technical capacity needs strengthening.
There is infrastructure in place. This includes hospitals, labs, research institutes, abattoirs, and
institutions of higher learning. These are spread out between the govt and the private sector,
including regional and international institutions.
Currently the on going activities include surveillance in both birds and humans, laboratory
diagnosis, enforcement of bans on importation of poultry and its products from affected
countries, and awareness creation.
The available financial resources are inadequate. The on going activities have so far been funded
by through the recurrent govt allocations from parent ministries and departments.
The existing legal framework includes the Public Health Act and the Animal Diseases Act. They
need to be reviewed to cater for:
Notification of HPAI
Compensation issues during the culling of birds in case of an outbreak.
This will put the put the legal framework in line with the provisions of the international
regulations.
Communication networks exist for the Secretariat that is currently housed in the Ministry of
Health. These include telephone, fax and e-mail services. These facilities are inadequate due to
competing tasks with other ministry departments. The services are not networked with the
districts hence the channelling of surveillance data and general communication with the field is
not efficient.
Institutional vehicles are currently being used for transport. Most of the time the vehicles are in
use by the respective departments thus not readily available. Some of them are old and unreliable.
Therefore two 4WD vehicles are needed specifically for the AI secretariat to be used for
monitoring and evaluation of the sub-committee activities.
There is political goodwill from the government. The office of the president-special programmes
is a member of the multi-sectoral task force. It has been very supportive in the generation of an
emergency preparedness plan.
JUSTIFICATION
Communication
For effective coordination of the activities on avian influenza, this team needs to hold weekly
meetings, to communicate with other stakeholders locally and internationally. .Stationery to
generate minutes and reports, computers and their accessories for the generation and storage of
data are required. Airtime and telephone services are needed due to the constant communication
with the sub-committees.
12
The Task Force has diverse membership. It has been meeting weekly with most of these
meetings taking most of the day. The Secretariat will be expected to work daily from Monday to
Friday. These teams need allowances to cater for their upkeep including transport costs.
Transport
The task force has no specific vehicles for its work. Currently it has been relying on vehicles from
govt departments. These vehicles are inadequate due to competing tasks. Some of them are very
old and unreliable. The team therefore needs at least two 4WD vehicles for its work.
Human Resources Mobilization
The staff two ministries require to respond to outbreaks of avian flu is a lot more than those in
place. The ministries will need to involve the private sector who will have to be paid. The budget
for this has been included.
Monitoring and Evaluation
The subcommittee will be monitoring all the activities of the other subcommittees to ensure that
they are on schedule and are carrying out activities as per the set budgetary limits.
Preparation of Sessional Papers and Legal Review
A policy on the modalities of how all the stakeholders will work together should be put in place
to ensure effective and efficient running of the programme.
Issues of compensation and prosecution charges in the present Acts (Animal diseases Act and
Public health Act) are very outdated. These Acts have to be reviewed so as to address the
relevant legal issues. The process of preparing the sessional paper and review the Acts will
require holding several retreats where stakeholders will be represented.
13
COORDINATION AND RESOURCE MOBILISATION WORKPLANS
1
2
Activity
Sub-activity
Convening of
National Task Force
meetings
Purchase of
stationery
Facilitation of the
coordination &
resource mobilisation
subcommittee
3
Monitoring and
Evaluation
4
Preparation of
sessional paper
Responsibility
(Who?)
DMS DVS
By When
Purchase of
airtime
Telephone
expenses
DMS
DVS
Mid-Dec
DMS
DVS
Mid Dec
Internet services
DMS
DVS
Mid-Dec
Purchase of
computers and
accessories
DMS
DVS
Mid-Dec
Secretariat
allowances
Entertainment
allowances
Purchase of 2
4WD vehicles
Fuel for vehicles
DMS
DVS
Mid-Dec
DMS
DVS
Mid-Dec
DMS
DVS
DMS
DVS
March
2006
Mid-Dec
Vehicle
maintenance
Supervision
DMS
DVS
Mid-Dec
DMS
DVS
On- going
Hold planning
retreats
DMS
DVS
Jun 2006
Mid-Dec
Expected
output
Stationery
purchased
Airtime
purchased
Official
telephone
calls made
Official
internet
communicati
on made
Computers
and
accessories
purchased
Allowances
paid
Allowances
paid
Vehicles
purchased
Fuel
procured
Vehicles
serviced
Supervision
of subcommittees
done
Sessional
paper on
coordination
of Avian
Influenza in
place
Indicator
Verification
Assumptions
Amount of
stationery
purchased
Value of airtime
cards purchased
Value of calls made
Recipts/LPOs
Funds will be available by Mid Dec 2005
Receipts
Funds will be available by Mid Dec 2005
Telephone
bills/Records
Funds will be available by Mid Dec 2005
Amount of
communication
done
Internet bills
Funds will be available by Mid Dec 2005
No. of computers
and accessories
purchased
Receipts/LPOs
Funds will be available by Mid Dec 2005
No. of members
paid
No of members
paid
No. of 4WD
vehicles purchased
Amount of fuel
procured
No. of service
sessions
No. of supervisory
visits
Records
Funds will be available by Mid Dec 2005
Records
Funds will be available by Mid Dec 2005
Log books/records
Funds will be available by March 2006
Fuel
ledgers/records
Log books/Records
Funds will be available by Mid Dec 2005
Records
Extra funds will be available by Mid Dec 2005
No. of retreats
undertaken
Sessional paper
14
Funds will be available by Mid Dec 2005
5
6
Activity
Sub-activity
Review of legal
statutes
Collaboration and
liasing with
international
communities
Hold planning
workshops
Attendance of
international and
regional meetings
and conferences
Responsibility
(Who?)
DMS DVS
By When
DMS
0-5 years
DVS
Jun 2005
Expected
output
Amended
Acts in place
Good
international
collaboration
Indicator
Verification
No. of workshops
undertaken
No. of meetings
and conferences
attended
Amended Acts
Assumptions
Meetings and
conference
proceedings
BUDGET REQUIREMENTS
1
Activity
Convening of National
Task Force meetings
Sub-activity
Purchase of Stationery
Provision of phone
services
Details
As in annex
Prepaid Airtime for
sub-committee
members
Post-paid Airtime for
DMS and DVS
Prepaid Calling Cards
(Telecom)
Provision of Internet
Services
Connection to DMS
Connection to DVS
2
Facilitation of the
coordination & resource
mobilisation
Procurement of ICT
Equipment and
accessories
Allowances
As in annex
Allowances for
Secretariat members
Quantity
See Annex
25
25
25
2
2
2
25
25
25
1
1
1
1
1
1
See Annex
Cost
(KShs)
See Annex
5,000
5,000
5,000
7,500
7,500
7,500
5,000
5,000
5,000
30,000
30,000
30,000
30,000
30,000
30,000
590,000
Immediate
Budget KShs
768,080
750,000
25
25
25
2,500
2,500
2,500
5,625,000
15
Medium Term
Budget KShs
2,038,400
Long Term
Budget KShs
4,527,975
2,250,000
4,500,000
90,000
270,000
540,000
125,000
2,250,000
4,500,000
180,000
540,000
1,080,000
180,000
540,000
1,440,000
360,000
1,080,000
100,000
16,875,000
33,750,000
Action by
DMS
DVS
Activity
subcommittee
Sub-activity
Office entertainment
Lunch allowance
Vehicles
Other sub-committees
Fuel for vehicles
Maintenance
3
4
5
6
Human Resource
Mobilisation
Implementation and
Monitoring
Preparation of sessional
paper
Review of legal statutes
7
Collaboration and
liasing with international
communities
TOTAL
Hiring of staff
Supervision of Subcommittees
Hold planning retreats
Hold planning
workshops
Attendance of
international and regional
meetings and
conferences
Details
Allowances for drivers
Beverages
Allowance for
Secretariat members
4WD Double cabin
Petrol for two
vehicles
Servicing of motor
vehicles. One service
monthly for two
vehicles
Cost
(KShs)
Quantity
2
2
2
500
500
500
assorted
10
10
10
2
500
500
500
2,500,000
30
30
30
12
18
78
80
85
5,000
5,000
36
7,500
1,200
25,000
Supervisory visits to
the field for 3 teams
3
104,000
Five retreats
5
Three retreats
A total of eleven
meetings
Immediate
Budget KShs
120,000
Medium Term
Budget KShs
Long Term
Budget KShs
360,000
120,000
450,000
360,000
720,000
720,000
1,350,000
2,700,000
5,000,000
561,600
1,728,000
3,672,000
60,000
90,000
270,000
540,000,000
1,080,000,000
624,000
1,572,000
4,192,000
649,700
649,700
2,598,800
3
649,700
649,700
1,949,100
1
300,000
600,000
12,993,080
2,400,000
582,531,300
16
Action by
3,600,000
1,145,951,975
1,741,476,355
EPIDEMIOLOGY AND SURVEILLANCE EMERGENCY PREPAREDNESS PLAN
STATEMENT OF FUNCTION, PURPOSE AND MANDATE
It has long been known that wild birds represent a resoervor of avian influenza virus worldwide.
This is a concern because many of these birds are migratory and travel long distances across
international borders.
Currently there is pandemic of the avian flu in the palearctic region and some of the bird species
that are reservoir for this virus are migrating into Kenya. The arrival of these birds started in
september this year and is expected to peak in December. Return journey starts from March to
April next year.
Although HPAI has not been diagnosed in Kenya either in wild birds or domestic birds, there is
a great risk of the virus being introduced into the country particularly because of its ability to
survive in envirronment for long periods especially in ponds, waterways and cool damp areas.
These are the same areas where our domestic birds go for watering.
There is therefore a critical and urgent need to detect the virus in the wildbirds and domestic
birds basically to answer the question as to whether or not we have HPAI in Kenya.
SITUATION ANALYSIS
Of the approximatelly 25 million poultry in Kenya, 81% are indiginieous birds which are reared
under back yard production. These are the birds that at risk since they roam freely and can easily
come in contact with wild bids or their secretions.
Retrospective surveys of avian diseases diagnosed at Central Veterinary Laboratory, Kabete
between 1935 and 2004 mention no avian influenza in the Kenyan poultry. However, no active
for avian influenza has been carried out so far.
In spite of that, Kenya has regarded avian influenza as a high risk disease and in fact declared it to
be a notifiable disease through a gazette notice in 1996. Subsequent to the reported outbreaks in
South East Asia, Kenya imposed a ban, through another legal notice in 1998, on importation of
poultry or poultry products from Asia and any other country reporting HPAI.
STATEMENT OF STRATEGY
Kenya is on the migratory route of wild birds. It is therefore necessary to establish mechanisms
and systems to detect cases of HPAI in domestic and wild birds, as well as other domestic
animals such as pigs and also in humans.
Adequate resources need to be set aside to reduce close contacts between humans and domestic
poultry, and wild birds through scientific approaches. This makes it necessary to carry out
surveillance in domestic birds, wild migratory birds and humans.
VISION
To be the leading African country in HPAI infection detection and early response.
MISION
To have a functional and efficient epidemiosurveillance system for HPAI.
GOALS AND OBJECTIVES
Goal
To detect promptly outbreak of H5N1 in migratory, domestic and wild birds and humans
and provide information on H5N1 pandemic.
Objective
To strengthen the existing surveillance structures
To ensure that all the reported case are thoroughly investigated
17
Train human and animal health workers on disease surveillance and response with special
focus on HPAI
Collect, analyze interpret data and disseminate the information for appropriate action
SWOT ANALYSIS
Strengths
An Epidemiosurveillance system (ESS) is in place for humans, domestic and wild birds
Linkages with other organization in place
For humans, there is an operational IDSR system in place and an available HMIS
Trained technical staff in the fields
Weakness
Health workers poorly understand Avian flu
Logistical support not adequate
Inadequate resources
Opportunities
Global interest in the HPAI
The threat of the pandemic
Threat
Sustainability
Insecurity in the field
Mutating nature of the virus involved
PROGRAMME DEVELOPMENT
TERMS OF REFERENCE
In the light of the background information on HPAI given, the members developed the
following TORs:
1. Define practical approaches to determine whether HPAI (H5N1) is present in the country or
not.
2. Define steps that are needed for early and rapid detection of HPAI in birds and other animals
3. Create a plan of action for surveillance of HPAI (H5N1) in humans
4. Determine means for early and rapid detection of person to person HPAI (H5N1)
transmission
5. Develop mechanisms for data storage and analysis and rapid communication of information
with other national sub-committees on HPAI
6. Develop mechanisms for coordination and harmonisation of activities related to foregoing
TOR.
1. Define practical approaches to determine whether HPAI (H5N1) is in the country
Domestic Birds
Carry out targeted surveillance
Map high-risk areas based on agreed criteria
Carry out targeted surveillance in identified high-risk areas
o Clinical on species exhibiting signs (chicken)
o Serological and viral for all species
Carry out random surveys- appropriate accuracy
18
Develop sampling frame, else opt for random coordinates
o Clinical on species exhibiting signs (chicken)
o Serological and viral for all species
Wild birds
Carry out targeted surveillance
Migratory – focus on water birds (ducks and geese)
Resident birds- focus on water birds: before and after migration
2. Define steps that are needed to identify HPAI in birds and other animals
Domestic Birds
Carry out passive surveillance in individual flocks, bird markets, borders
Case definition: Increased mortality, reduced feed and water consumption, presence
of signs of respiratory disease or a drop in egg production
Awareness creation among AHSPs, poultry keepers & breeders, traders, butchers,
slaughter-house operators and the general public
Maintenance of rumour registers + verification of reports
Prompt reporting (telephone, email, SMS, VHF radio) of suspicious cases with
follow-up investigations leading to a logical conclusion (In the absence of suspicious
cases, zero report and at what frequency?)
Wild Birds
Carry out passive surveillance in individual flocks, bird markets, borders
Tentative case definition: Increased mortality
Determine HPAI status in wild migratory birds
Create awareness among rural population, hunters, rangers, and general public
Prompt reporting
3. Surveillance of HPAI (H5N1) in humans
Case definition:
Focus on ports of entry and persons/ institutions in high-risk areas identified for passive
and targeted surveillance in birds
Continuously educate health workers about HPAI
Provide health workers with fact sheets about HPAI
4. Determine means for early and rapid detection of person to person HPAI (H5N1)
transmission
Follow up all in-contacts with index cases
Persons once infected should be isolated
Scale-up the integrated disease surveillance and control to include influenza
5. Develop mechanisms for data storage and analysis and rapid communication of
information with other national sub-committees on HPAI
Share information with other national HPAI sub-committees
6. Develop mechanisms for coordination and harmonisation of activities related to
foregoing TOR
DVS to coordinate activities related to foregoing TORs
19
EPIDEMIOLOGY AND SURVEILLANCE (DOMESTIC BIRDS) WORK PLAN
No
Activity
Sub-activity
Action
By
DVS
By
when
Dec-Jan
Mar-Apr
Expected output
Indicators
1
Carry out targeted
surveillance in domestic
poultry and other domestic
animals.
To clinically inspect up to
400 poultry flocks/ markets
and collect sera and
virological material from up
to 10,800 poultry, plus sera
from up to 3600 pigs per
field mission
DSA for field mission- 14
teams each composed of
2 vets, 1 technician, and 1
driver- 19 days inclusive if
travel
Number of –ve &
+ve cases of HPAI
diagnosed
10,800 poultry
samples and 3,600
pig samples
collected and
analysed
Vehicle servicing,
maintenance, fuel and
lubricants for 14 vehicles
DVS
Dec-Jan
Serviceable vehicle
Operational vehicle
Tires and batteries
DVS
Jun 2006
Tires and batteries
No. purchased
Field sampling kit for 14
teams
DVS
Dec
2005
Sampling kits
No. Purchased
Briefing & debriefing of
14 teams (DSA, transport
refunds, stationery)
DVS
Dec
2005
Officers
briefed/trained
Short-term training (local)
DVS
Dec
2006
Trained officers
Imprest warrant
forms; work tickets;
bus fare tickets;
reords of the
meeting
Efficiency in
carrying out duties
Short-term training
(external)
DVS
Dec
2006
Trained officers
Purchase of motorized
cool boxes for field work
DVS
Motorised
boxes
Purchase of portable
computers
DVS
Dec
2005
and
Dec
2007
Jun 2006
Assumptions
Log book
entries
Payments for
services
Stores records
S3 cards and
S11
Stores records
S3 cards and
S11
Report
generated
Adequate and timely release of
funds
HPAI Continues to be a threat
Cert of
attendance
MTC minutes
Cert of
attendance
MTC minutes
Adequate and timely release of
funds
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
No. purchased
Stores ledger
S3 cards and
S11
Adequate and timely release of
funds
HPAI Continues to be a threat
No. purchased
Stores ledger
S3 cards and
Adequate and timely release of
funds
Efficiency in
carrying out duties
cool
Portable computers
20
Means of
Verification
Reports
Field visits
made
Adequate & timely funding from
GoK and partners
Cooperation from poultry and
domestic animal owners
Functional laboratory facilities
HPAI Continues to be a threat
Adequate and timely release of
funds.
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
No
2
3
Activity
Carry out random surveys in
poultry and other domestic
animals.
To clinically inspect at least
600 poultry flocks/ markets
and collect sera and
virological material from at
least 20,000 poultry, plus
sera from at least 5,000 pigs
per field mission
To Strengthen passive
surveillance in both poultry
and wild birds.
Sub-activity
Action
By
By
when
Expected output
Indicators
Means of
Verification
S11
Assumptions
Stores ledger
S3 cards and
S11
Stores ledger
S3 cards and
S11
Adequate and timely release of
funds
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
HPAI Continues to be a threat
Purchase of GPS
DVS
Dec
2007
GPS
No. purchased
Purchase of 4 WD
vehicles
DVS
4 WD vehicles
No. purchased
DSA for field mission- 20
teams each composed of
2 vets, I technician, and I
driver- 25 days inclusive if
travel
DVS
Dec
2006
and
Dec
2007
Jun 2006
each
year
Number of –ve &
+ve cases of HPAI
diagnosed
20,000 poultry
samples and 5,000
pig samples
collected
Reports
Rumour
registors
Adequate & timely funding from
GoK and partners
Cooperation from poultry and
domestic animal owners
Functional laboratory facilities
HPAI Continues to be a threat
Vehicle servicing,
maintenance, fuel and
lubricants for 20 vehicles
DVS
Dec-Jan
Serviceable vehicle
Operational vehicle
Adequate and timely release of
funds
HPAI Continues to be a threat
Field sampling kit for 20
teams
DVS
Sampling kits
No. Purchased
Briefing & debriefing of
14 teams (DSA, transport
refunds, stationery)
DVS
Dec
2005
and
Jun 2007
Dec
2005
Log book
entries
Payments for
services
Stores records
S3 cards and
S11
Officers
briefed/trained
Report
generated
Adequate and timely release of
funds
HPAI Continues to be a threat
Lunches and DSA for
district and provincial
offices respectively while
carrying out market
inspection. 115
districts/provinces
Vehicle servicing,
maintenance, fuel and
lubricants for 20 vehicles
DVS
Jul 2006
Number of –ve &
+ve cases of HPAI
diagnosed
Imprest warrant
forms; work tickets;
bus fare tickets;
reords of the
meeting
20,000 poultry
samples and 5,000
pig samples
collected and
analysed
Reports
Field visits
made
DVS
Dec-Jan
Serviceable vehicle
Operational vehicle
Log book
entries
Payments for
services
Adequate & timely funding from
GoK and partners
Cooperation from poultry and
domestic animal owners
Functional laboratory facilities
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
21
Adequate and timely release of
funds
HPAI Continues to be a threat
No
Activity
Sub-activity
4
Carry out prompt disease
reporting and investigation
Running costs for toll free number
5
Develop and run database
for avian influenza for DVS
Action
By
DVS
By
when
Dec
2005
Expected output
Indicators
Toll-free number
The number exists
and operational
Field investigations - DSA
DVS
Dec
2005
Number of –ve &
+ve cases of HPAI
diagnosed
Field investigations—
vehicle maintenance,
servicing, fuels &
lubricants
Purchase of field sampling
kits for 20 districts
DVS
Dec
2005
Serviceable vehicle
20,000 poultry
samples and 5,000
pig samples
collected and
analysed
Operational vehicle
DVS
Sampling kits
No. Purchased
Purchase server
DVS
Dec
2005
and
Jun 2007
Jul 2006
Server
No. purchased
Purchase PCs (with
printer and UPS) for high
risk districts and
provinces
Purchase/develop
software
DVS
Jul 2006
and Dec
2007
Computers
No. purchased
DVS
Jul 2006
Software
No. purchased or
developed
Collate and analyze avian
influenza data, including
GIS mapping – 5
personnel
DVS
Dec
2006
Collated
analysed data
and
Share and disseminate
information (email and
internet running costs)DVS
Hold national workshops
on topical subjects related
to epidemio-surveillance
DVS
Dec
2006
e-mails
downloaded
information
and
DVS
Jan 2006
Harmonised
and
updated information
on HPAI
22
Raw data to be
collated and
analysed in form of
questionnaires and
checklists
ISP charges;
Telephone charges
No. of workshops
Means of
Verification
Bills; list of
calls made
Reports
Field visits
made
Assumptions
Adequate and timely release of
funds
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
Log book
entries
Payments for
services
Stores records
S3 cards and
S11
Adequate and timely release of
funds
HPAI Continues to be a threat
Stores ledger
S3 cards and
S11
Stores ledger
S3 cards and
S11
Adequate and timely release of
funds
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
Stores ledger
S3 cards and
S11
Reports
Adequate and timely release of
funds
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
Copies of emails and
disseminated
information
Workshop
proceedings
reports
Adequate and timely release of
funds
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
Adequate and timely release of
funds
HPAI Continues to be a threat
EPIDEMIOLOGY AND SURVEILLANCE (HUMANS) WORK PLAN
Activity
Sub Activity
Surveillance
Active surveillance on
avian influenza and
monitor pneumonia
trends in hospitals
Responsibility
(Who?)
National, Provincial
and
Districts
surveillance teams
Time frame (By
when?)
Dec 2005 – May
2006
Expected outputs
Means
of
Verifications
Surveillance
Reports
Assumption
No.
of
Surveillance
reports
from
teams
Surveillance
Reports
Availability of funds.
HPAI remains a threat
Surveillance data tools
printed and distribute
No. of disease
surveillance tools
printed
and
distributed
Distribution
report
Availability of funds.
Jan 2008
Dec 2005 – Dec
2010
Sentinel sites established
No. of functional
sentinel sites
Availability of funds.
Functional
emergency
response teams in place
Number of cases
investigated
Influenza
laboratory data
from the sentinel
sites
Surveillance
reports
Early
detection
suspected cases
Indicators
of
Pneumonia
trends
monitored in hospitals
Early
detection
of
suspected cases
No.
of
Surveillance
reports
from
teams
Availability of funds.
HPAI remains a threat
Surveillance
Focused surveillance
in 20 high risk districts
based on migratory
birds pattern
National, Provincial
and
Districts
surveillance teams
2006 Dec 2005 –
May
Strengthening
data
collection
and reporting
Develop, print &
disseminate
Surveillance data tools
DOMU
Jan 2006
Sentinel
surveillance
Scale up Sentinel
surveillance in 10
identified hospitals
KEMRI
Targeted
surveillance
Targeted surveillance
in 8 ports of entry –
Emergency response
teams
Carry out targeted
surveillance
for
poultry and poultry
products
-Food
quality control
Train Health Workers
on Integrated disease
surveillance
with
special focus on Avian
Influenza
Data management and
dissemination
DOMU
Dec
2010
Chief Public Health
officer
Dec
Dec2010
2005-
Poultry
and
poultry
products
surveillance
carried out
Number
of
poultry
and
poultry products
inspected
Inspection reports
Availability of funds
DOMU
Dec-2005
2006
May
Strengthened
district
capacity in IDSR and avian
influenza
Training reports
Availability of funds
DOMU
Dec- 2005 May
2006
Computers and accessories
procured and distributed
No.0f DHMTs
trained, No of
facilities
H/workers
trained
No. of computers
and accessories
procured
and
distributed
Distribution
schedule
Availability of funds
Surveillance on
poultry
and
poultry products
Training
Data
management
Jan 2007
2005-Dec
23
Availability of funds.
HPAI remains a threat
Data
management
Strengthen
logistical support
for surveillance
Strengthen
logistical support
for surveillance
Strengthening
Communication
capacity
Coordinate and
harmonize
all
sub-committee
activities
Develop and install a
data base for HPAI &
human influenza at
National, provincial
and district levels
Transport operations
and maintenance
DOMU
Dec20052006
May
IDSR soft ware installed
and functional
DOMU
PHMTs
DHMTs
Permanent Secretary
Health
Dec
Dec2010
2005-
Vehicles serviced and used
for surveillance activities
Dec 2005 –May
2006
Vehicles procured
distributed
Communication costs
at all levels
DOMU
PDSCs
DDSCs
Dec 2005 –Dec
2010
Effective and Efficient
reporting of cases
Entertainments
DOMU
Dec 2005 –Dec
2010
Subcommittees
done
Strengthen
disease
surveillance in all level
and
meetings
No.
of
programmes,
provinces
and
districts
with
IDSR data base
Inspection reports
Availability of funds
Availability of funds
No. of vehicles
procured
and
distributed
No. of reports
received through
Fax, emails and
SMS
No.
of
Sub
committees
meetings held
Procurement
reports
Availability of funds
Availability of funds
Sub committees
minutes
Availability of funds
EPIDEMIOLOGY AND SURVEILLANCE (WILD BIRDS) WORK PLAN
Activity
Sub-activity
By Who
By when time
frame
Expected output
Indicators
Immediate
targeted
surveillance
Carry out targeted
surveillance focusing
mainly on migratory
bird species in the 7
critical zones
NMK-Ornithology
Dept.
Dec.2005 to May
2006
Specimens samples
for HPAI screening
At least 4000 birds
specimens from all
the seven critical
zones
KWS-Vet.+
Research Depts.
MOV
Assumptions
Lab reports
Funds available
Data base
HPAI threats persists
Specimens
Funds available
Build Capacity
Developing the
existing human
Train bird
ringers/trapper on
methodologies of
collecting the
specimens
Train ornithological
tour guides to collect
NMK-Ornithology
Dept.
KWS-Vet.+
Research Depts.
NMK-Ornithology
Dept.
3rd quarter of
year one
Trained
ringers/trappers
for 3 zones
At least 20
ringers/trappers
trained
Progress report
At least 20
ringers/trapper
trained
Workshop report
three
Trained
ringers/trappers
for 4 zones in
23rd quarter of
first year
Trained
ornithological tour
At least one key
ornithological tour
Workshop report
HPAI reporting
1st quarter of year
24
HPAI threats persists
Training manuals
Ornithological tour
companies provide
Activity
Sub-activity
capacity
and convey
information related to
HPAI to NMKOrnithology Dept.
and KWS-Vet. +
Research Depts. for
quick response
Carry out surveillance
in the seven zones
targeting mainly the
resident bird
Carry out
targeted
surveillance
By Who
By when time
frame
KWS-Vet.+
Research Depts.
NMK-Ornithology
Dept.
May-September
1st to 5th year
KWS-Vet.+
Research Depts.
Expected output
Indicators
MOV
Assumptions
guides able to
provide accurate
information on
HPAI in wild birds
within operational
circuits
guide in each of the
seven key zones
trained
guideline manual for
Tour guides
key persons for
training
Resident birds’
specimen collected
from all the seven
critical zones
At least 800 resident
bird specimens
collected in each of
the seven HPAI
critical zones
Workshop report
Annual report
Carry out
targeted
surveillance
Review and
harmonize the
methods used to
collect specimens
Create
information
exchange and
databases wild
bird surveillances
Carry out surveillance
in the seven HPAI
critical zones targeting
mainly the migratory
water bird
Theoretical and
practical orientation of
the wild birds
surveillance team to
reviewed methods
Establish databases
for information on the
ringed sampled birds
and internet with web
page for exchange of
such information
Carry out passive
surveillance
NMK-Ornithology
Dept.KWS-Vet.+
Research Depts.
NMK-Ornithology
Dept.-.
KWS-Vet.+
Research Depts.
NMK-Ornithology
Dept.
KWS-Vet.+
Research Depts.
NMK-Ornithology
Dept.KWS-Vet.+
Research Depts.
September –April
1st to 5th year
Migratory birds’
specimen collected
from all the seven
critical zones
3rd quarter of
year one
1st quarter of year
three
Wildlife surveillance
team members
trained on the
reviewed methods
At least 1000
migratory bird
specimens collected
in each of the seven
HPAI critical zones
At least one
workshop held
At least one
workshop held
3rd quarter of
year one
Database and
internet web page
functioning at NMKOrnithology Dept.
and KWS-Vet.+
Research Depts.
Two Computers with
sampled birds
information
databases and
internet web pages
functioning
Information on
HPAI status in all
parts of the country
for rapid response
Quarterly Passive
surveillance reports
from all the seven
critical HPAI Zones
plus the rest of the
country
Lab reports
Data base
Water birds will be
available in the all the
zones
Specimens
Lab reports
Data base
Specimens
Workshop report
Migratory Water
birds will be available
and equally dispersed
in the all the zones
Funds will be
available
Training manual
Receipts
Funds are available
Equipment
themselves
HPAI and other wild
bird diseases threat
persists
Funds are available
2nd quarter
Of first year
continuous to
year five
Ornithological tour
guides
25
Quarterly reports
Rumor reports
HPAI and other wild
bird diseases threat
persists
EPIDEMIOLOGY AND SURVEILLANCE BUDGET SUMMARY
Activity
Sub-activity
Carry out targeted surveillance in domestic poultry and other
domestic animals. To clinically inspect up to 400 poultry flocks/
markets and collect sera and virological material from up to
10,800 poultry, plus sera from up to 3600 pigs per field mission
DSA for field mission- 14 teams each composed of 2 vets, 1
technician, and 1 driver- 19 days inclusive if travel
Vehicle servicing, maintenance, fuel and lubricants for 14
vehicles
Tyres and batteries
Field sampling kit for 14 teams
Briefing & debriefing of 14 teams (DSA, transport refunds,
stationery)
Short-term training (10 personnel)
Immediate
Medium Term
Long Term
2,500,000
10,000,000
15,000,000
616,000
1,848,000
3,696,000
1,148,000
2,296,000
916,700
2,750,100
5,500,200
1,000,000
3,000,000
6,000,000
2,500,000
5,000,000
5,000,000
10,000,000
Short-term training (5 personnel)
Purchase of motorized cool boxes for field work
4,000,000
Purchase of portable computers
2,000,000
2,000,000
Purchase of GPS
Carry out random surveys in poultry and other domestic animals.
To clinically inspect at least 600 poultry flocks/ markets and
collect sera and virological material from at least 20,000 poultry,
plus sera from at least 5,000 pigs per field mission
2,000,000
Purchase of 4 WD vehicles
25,000,000
12,500,000
DSA for field mission- 20 teams each composed of 2 vets, I
technician, and I driver- 25 days inclusive if travel
Vehicle servicing, maintenance, fuel and lubricants for 20
vehicles at KShs 55/km
Field sampling kit for 20 teams
15,000,000
75,000,000
6,050,000
12,110,000
2,620,000
3,930,000
2,000,000
5,000,000
Briefing and debriefing of teams (DSA, transport refunds,
stationery)
Purchase of palm tops
Targeted surveillance of migratory and resident birds
Surveillance during the months of Palearctic migration total of
105 days
Surveillance during the months of Palearctic migration total of
384 days (24days/month for 16 months)
26
200,000
3,045,000
11,136,000
Activity
To Strengthen passive surveillance in both poultry and wild birds.
Carry out prompt disease reporting and investigation
Sub-activity
Immediate
Surveillance during no Palearctic migration period total of 96
days (12 days per month for 8 months)
Surveillance during no (144 days) and when there is (576 days)
palearctic migration total 720 days) in three years
Lunches and DSA for district and provincial offices
respectively while carrying out market inspection. 115
districts/provinces
Vehicle servicing, maintenances, fuel and lubricants 115
districts and provinces at ksh 55/km
Running costs for toll - free number at Ksh 60,000 per month
Medium Term
Long Term
2,784,000
20,880,000
36,000,000
90,000,000
6,050,000
69,575,000
34,500,000
360,000
1,440,000
3,600,000
Field investigations - DSA at 80,000 per month
480,000
1,920,000
4,800,000
Field investigations - vehicle maintenance, servicing, fuels &
lubricants at KShs 55/km
Purchase of field sampling kits for 20 districts
300,000
900,000
2,700,00
1,310,000
3,930,000
7,860,000
750,000
750,000
Purchase server
Active surveillance on avian influenza and monitor pneumonia
trends in hospitals
Focused surveillance in 20 high risk districts based on migratory
birds pattern
Strengthening data collection and reporting
Support the National, province and district for surveillance
activities
Rapid response teams by the national, provincial and district
3,800,000
30,000,000
60,000,000
3,000,000
9,000,000
18,000,000
Develop, print & disseminate Surveillance data tools
1,500,000
4,500,000
9,000,000
Sentinel surveillance
Scale up Sentinel surveillance in 10 identified hospitals. Nyeri
PGH, Eldoret Moi refferal, KNH, Mbagathi, Kisumu, Coast
PGH, Rift Valley PGH, Embu PGH, Garissa PGH and
Machakos.
Targeted surveillance in 8 ports of entry – Emergency
response teams
Carry out targeted surveillance for poultry and poultry
products -Food quality control.
Public
health inspections and food sampling in 8 ports of entry , 20
high risk districts and 2 for central level (30 sites)
Train Health Workers on Integrated disease surveillance with
special focus on Avian Influenza
Strengthen data collection, reporting, analysis and
dissemination
2,522,000
9,000,000
25,280,000
2,480,000
5,940,000
11,880,000
4,480,000
10,170,000
20,340,000
5,000,000
25,000,000
2,000,000
3,000,000
2,500,000
Targeted surveillance
Training of Health workers
Data management
27
Activity
Sub-activity
Strengthen logistical support for surveillance
Develop and install a data base for HPAI & human influenza
at National, provincial and district levels
Transport operations and maintenance
Strengthen logistical support for surveillance
Purchase 85 surveillance double cabin vehicles
Strengthening Communication capacity
Communication costs at all levels
Develop and run database for avian influenza for DVS
Purchase PCs (with printer and UPS) for high risk districts and
provinces
Purchase/ develop software
Coordination and secretariat
Sampling Kit
Capacity building
Collate and analyze avian influenza data, including GIS
mapping – 5 personnel
Share and disseminate information (email and internet running
costs)- DVS
Hold national workshops on topical subjects related to
epidemio-surveillance
Purchase of sampling Kit
Immediate
Medium Term
Long Term
1,500,000
1,800,000
1,800,000
5,610,000
16,830,000
33,660,000
12,500,000
200,000,000
2,232,000
4,464,000
5,600,000
2,000,000
744,000
1,000,000
375,000
1,125,000
2,250,000
180,000
540,000
1,080,000
360,000
1,080,000
2,160,000
1,959,000
5,887,000
11,754,000
3,130,000
4,560,000
735,480
2,206,440
4,412,880
53,590
160,770
321,540
Communication
Training of human resource on sampling protocols all over the
country
Telephone and administration
Stationery
Purchase of various stationery
Transport
Purchase of vehicles
3,504,045
Passive Surveillance
Transportation to, within and from the field using two land
rovers boats
Carry out passive surveillance
Equipment
Purchase of various equipment
1,762,000
8,773,000
58,380,815
308,373,310
5,000,000
TOTALS
28
14,016,180
35,040,450
1,520,000
1,520,000
581,220,620
LABORATORY AND RESEARCH
INTRODUCTION
Avian influenza is an infectious disease caused by avian influenza viruses. It is highly contagious
among birds and has the potential to cause high mortality. It does not usually infect humans.
However, some 122 people have so far been reported to have been infected by H5N1 subtype
with a 50% mortality rate. Pandemics may be induced when influenza viruses from birds,
humans and pigs grow together. The H5N1 subtype currently infecting chickens in the Far East
has directly infected humans from birds thus sending danger signals for a global pandemic should
it develop capacity for human to human transmission. There is therefore an urgent need for
Kenya, like all other countries worldwide, to develop preparedness plans covering birds, humans
and other at risk animals which should incorporate research to improve understanding of avian
influenza, as well as plans to enhance capacity for laboratory diagnosis of the disease.
Laboratory Diagnosis of Influenza Viruses Infection
During epidemics, a presumptive diagnosis can be made on the basis of the clinical symptoms.
However, influenza A and B can co-circulate, and mixed infections of influenza and other viruses
have been reported. Isolated cases of suspected influenza should be investigated for these may
represent the first cases of an impending epidemic.
Virus Isolation - Throat swabs, NPA and nasal washings may be used for virus isolation. It is
reported that nasal washings are the best specimens for virus isolation. The specimen may be
inoculated in embryonated eggs or tissue culture. 10-12 day embryonated eggs are used for virus
isolation. The specimen is inoculated into the amniotic cavity. The virus replicates in the cells of
the amniotic membrane and large quantities are released back into the amniotic fluid. After 2-3
days incubation, virus in the amniotic fluid can be detected by adding aliquots of harvested
amniotic fluid to chick, guinea pig, or human erythrocytes. Pathological specimens can be
inoculated on to tissue cultures of kidney, chicks or a variety of other species. Rhesus monkey
cells are the most sensitive. Although no CPE is produced, newly produced virus can be
recognized by haemadsorption using the cells in the tissue culture, and haemagglutination using
the culture medium which contains free virus particles. Influenza B virus and occasionally
influenza A will produce a CPE in MDCK cells. Influenza viruses isolated from embryonated
eggs or tissue culture can be identified by serological or molecular methods. Influenza viruses can
be recognized as A, B, or C types by the use of complement fixation tests against the soluble
antigen. (A soluble antigen is found for all influenza A, B or C type virus but antibody against
one type does not cross react with the soluble antigen of the other. The further classification of
influenza isolates into subtypes and strains is a highly specialized responsibility of the WHO
reference laboratories. The HA type is identified by HAI tests, the NA type is also identified.
Rapid Diagnosis by Immuno-fluorescence - cells from pathological specimens may be
examined for the presence of influenza A and B antigens by indirect immuno-fluorescence.
Although many workers are convinced of the value of this technique, others have been
disappointed with the specificity of the antisera and the level of background fluorescence that
makes the test difficult to interpret. EIA tests for the detection of influenza A viral antigens are
available that are easier to interpret than immuno-fluorescence. PCR assays for the detection of
influenza RNA have also been developed but there usefulness in a clinical setting is highly
questionable.
Serology - Virus cannot be isolated from all cases of suspected infection. More commonly, the
diagnosis is made retrospectively by the demonstration of a rise in serum antibody to the
29
infecting virus. CFT is the most common method used using the type specific soluble antigen.
However, the CF test is thought to have a low specificity. A more specific test is the HAI test.
Infection by influenza viruses results in a rise in serum antibody titre, but the requirement for a 4fold or greater rise in titre of HI of CF antibody reflects the inaccuracy of these tests for
detecting smaller increases in antibody. A more precise method for measuring antibody is by
SRH. SRH is more sensitive than CF or HAI tests and has a greater degree of precision. A 50%
increase in zone area represents a rise in antibody and is evidence of recent infection. Sera do not
have to be pretreated to remove non-specific inhibitors which plaque the HAI test. SRH may
well replace CF and HAI tests in diagnostic laboratory in future.
VISION
Kenya attains best practice status in the establishment and operation of centers of excellence for
research, detection and diagnosis for Highly Pathogenic Avian Influenza (HPAI).
MISSION
To provide timely, accurate and reproducible research, detection and diagnosis systems and
mechanisms for HPAI in a safe environment.
GOALS
Build capacity to carry out safe HPAI screening for all suspect cases of avian, human and
other animal sources.
The HPA1 status of the KEMRI, CVL, UON labs are authenticated to conform to BL3
status to ensure that HPAI is safely handled
To promote research to improve understanding of the disease
OBJECTIVES
To develop pertinent research to further understand and control avian influenza in Kenya
To develop sensitive and specific molecular diagnostic techniques for diagnosis AI
To provide adequate bio-safety mechanisms for laboratory and field workers
To demonstrate circulating strain of avian flu viruses including genetic information
To engage properly trained laboratory and field personnel to handle HPAI specimens
To harmonize handling and processing procedures for detection of HPAI
To ensure that all the logistical materials are in place including reagents
STRENGTHS
Well trained and competent personnel in place
Already existing laboratory network
Surveillance teams (both animal and human) already exist in the districts
A measure of cooperation from between public and private sector stakeholders on avian
influenza control
Multidisciplinary approach by various stakeholders in the sector
The ability to detect presence of HPAI
WEAKNESSES
Insufficient staff
Inadequate laboratories supplies and equipment
Inadequate logistical support such as transport
Inadequate bio-safety and bio-security preparedness
30
OPPORTUNITIES
Willing development partners
Collaboration with international laboratories e.g. ILRI, CDC
Training of personnel on emergency preparedness
THREATS
Kenya being on migratory path of migratory birds suspected to carry HPA1 virus
Many species of migratory birds pass through Kenya
Rearing of poultry in close proximity to humans
The HPAI may be introduced before the laboratories have been updated
Use of slow diagnostic procedures
Lack of bio-safety level 3 laboratories
Inadequate capacity of the laboratories to handle a large number of specimens
SITUATION ANALYSIS
HPAI Diagnostic Ability
It is projected that approximately 30,000 specimens from among migratory birds, 23,000 from
domestic poultry, 4000 specimens from pigs, and 5000 human specimens annually.
There are five laboratories in Kenya that can handled avian influenza specimens, namely;
KEMRI, Central Veterinary laboratory (CVL), Centers for Disease Control-International
Emerging Infections Program (CDC/IEIP), University of Nairobi-Faculty of Veterinary
Medicine (UON-FVM), and International Livestock Research Institute (ILRI). The KEMRI,
CVL, and UON-FVM laboratories handle influenza-suspect human or animal cases at the
present. Indeed, the KEMRI laboratory has processed specimens and isolated Influenza type A
strains (low pathogenic) annually, whereas CVL and UON – FVM have processed all animal
(primarily avian) suspect cases of avian influenza using egg inoculation followed by
hemagglutination inhibition (HI) methodologies.
The CDC/IEIP laboratory is a newly built biosafety level-3 facility with technical capability for
performing conventional and real-time PCR for both human and animal specimens. Presently,
this US-funded laboratory provides molecular diagnostic services. The ILRI laboratory is
technically capable of performing molecular diagnosis but it is not a BL-3 facility, thereby making
safety a serious concern. The ILRI is in the process of upgrading the laboratory, which will,
however, take some time to complete.
Experts recommend that human and animal specimens be processed in different laboratories to
minimize cross-contamination. Measures to revamp and upgrade the diagnostic capacity for
HPAI and to ensure that diagnosis is carried out safely are therefore quite urgent.
Recommended Specimen Flow
1. KEMRI laboratory will handle all human AI specimens in Kenya.
2. CVL laboratory will handle all migratory birds, pigs, and some domestic bird specimens.
3. The UON-FVM laboratory will handle the rest of domestic poultry specimens.
4. CDC/IEIP laboratory will perform RT-PCR testing for all human and animal specimens
in the interim.
5. ILRI laboratory will later (by June 2006) handle RT-PCR testing for avian samples in
order to keep human and animal tissues separate.
31
COLLECTION, HANDLING, AND TRANSPORTATION OF AI SUSPECT
SPECIMENS
Materials destined for the laboratories will be treated as follows:
Dead domestic and wild birds will be picked with hands surrounded by plastic paper and
enclosed in the plastic. If possible, a second layer of plastic paper will be used. The birds will
then be sent to local VIL or VO. Farmers around Nairobi can also send samples to UONFVM as they have done in the past.
The first responders (VIL/VO) will perform the post-mortem on dead birds as usual using
standard PPE. Collect spleen, trachea, intestines, and long bone and send these to Central
Veterinary Laboratory (CVL) in transport media.
Any persons coming into contact with sick wild or domestic birds should call the veterinary
officer immediately
In respect of HPAI suspect patients at a local clinic or hospital, clinician/nurses will collect
throat or nasopharyngeal swabs (under routine PPE) and send them to the KEMRI Influenza
Laboratory through the normal transportation channels.
TRAINING NEEDS
In each provincial and district hospital, laboratory and clinic staff will be trained on
collection, packaging, and transportation of suspect influenza virus specimens.
The DVS laboratory and field staff will be trained on safe handling of suspect AI specimens.
BIO-SAFETY ISSUES
All laboratory personnel shall be vaccinated against seasonal influenza (this is not HPAI) in
order to protect them against existing influenza subtypes and to raise the alarm in case they
show avian influenza-like symptoms.
All laboratories shall endeavour to stock reasonable amounts of TamifluR stock to be able to
treat laboratory personnel (TamifluR for approx 500 lab/hospital personnel is required).
Each provincial hospital will have PPE for approx 20 people, and each district hospital a PPE
for 10 people
Each district veterinary office shall have at least 5 sets of PPE.
IMMEDIATE RESEARCH OBJECTIVES
The KEMRI laboratory will be funded to expand it’s surveillance activity to Nyanza, Rift
Valley, Coast, and Western provinces. Currently, the laboratory carries out surveillance in the
Nairobi area only. This would include doubling the personnel in the laboratory, and
upgrading the laboratory to BL-3.
Established routine AI surveillance programs at UON, DVS, and ILRI will be carried out to
cover both wild and domestic birds. This surveillance will particularly focus on the areas with
high density of ducks.
All HPAI surveillance and monitoring in the country will be coordinated through the
National Task Force (via the Laboratory and Research Ccommittee). No materials will be
exported without permission of the National Task Force to ensure proper documentation of
AI prevalence in the country.
LABORATORY UPGRADE
1. The KEMRI Human Influenza Laboratory will be upgraded to BL-3 immediately
2. Two Avian Influenza laboratories will be upgraded to BL-3, in the listed order of priority
32
(i) CVL - Kabete
(ii) UON-FVM - Kabete
BUDGET
The expected work load from which budgetary estimates are derived are as follows
A. Specimens from routine outbreak public health response
Wild and domestic birds specimens – Immediate 10,000, thereafter 20,000 per year
Human -Immediate 5000, and an equal number per year
B. Specimens from targeted HPAI surveillance (Surveillance subcommittee)
Migratory birds – Immediate 7,000, Medium 30,000 (total), Long-term 45,000 (total)
Domestic poultry – Immediate 11,000, Medium 20,000/yr, Long-term 20,000/yr
Pigs - Immediate 3600, Medium 5,000/yr, Long-term 5000/yr
Definition: Immediate = 0-6 months, Medium = 7 month – 2 yrs (1.5 yrs), Long-term 3-5 yrs
(3 yrs)
The samples to be processed sum up to 36,600 in the immediate period; 80,000 in the medium
period, and 195,000 in the long-term period; for a grand total of 301,600 specimens over the
next 5 years.
33
BUDGET SUMMARY FOR THE LABORATORY PROGRAMME
Item
(KShs for 1.5yrs)
50,000,000
50,000,000
50,000,000
150000000
12018000
3833775
6000000
Long-term
(KSh/yr)
10000000
10000000
10000000
30000000
2,003,000
2,555,850
4,000,000
(KSh for 3 yrs)
30,000,000
30,000,000
30,000,000
90000000
6,009,000
7,667,550
12,000,000
Total
(KSh for 5 yrs)
90,000,000
90,000,000
90,000,000
270,000,000
36,054,000.00
14,057,175
25,925,575
2,000,000
16,567,850
500,000
3000000
24,851,775.00
750000
2,000,000
10,558,850
500,000
6,000,000
44,576,211
1,500,000
13,875,000
102,811,411
2,750,000
3,000,000
3,500,000
2,710,455
1,313,984
1,313,984
5,338,423
4,000,000
500,000
1,000,000
1,224,029
1,313,984
1,313,984
3,851,997
2,000,000
750000
1,500,000
1836043.5
1970976
1970976
5,777,995.50
3000000
500,000
1,000,000
1,224,029
1,313,984
1,313,984
3,851,997
2,000,000
1,500,000
3,000,000
3,672,087
3,941,952
3,941,952
11,555,991
6,000,000
5,250,000
8,000,000
8,218,585.50
7,226,912
7,226,912
22,672,410
13,000,000
Sub total
9,000,000
13,000,000
2,000,000
4,000,000
3000000
6,000,000
2,000,000
4,000,000
6,000,000
12,000,000
18,000,000
31,000,000
TOTAL
85,221,848
125,419,847
188,129,771
49,410,847
161,132,202
434,483,821
Laboratory upgrade
Sub total
Procurement
(Laboratory reagents
and consumables)
Sub total
Capacity
(Training
safety)
building
on bio-
Lab.
Action by
Immediate ksh
CVL
KEMRI
UON
DVS
DMS
Dean-FVM
CVL
KEMRI
ILRI
DVS
DMS
DVS
UON
Dean-FVM
CVL
DVS
KEMRI
DMS
CVL
KEMRI
UON
DVS
DMS
Dean-FVM
CVL
DVS
KEMRI
DMS
Sub total
Laboratory safety
Sub total
Logistical
(transport)
support
10,000,000
10,000,000
10,000,000
30,000,000
18,027,000
2,555,850
7,925,575
Medium
(KSh/yr)
33333333.33
33333333.33
33333333.33
100000000
8,012,000
2,555,850
4,000,000
4,875,000
33,383,425
500,000
*Itemized budgets from each laboratory are provided as Appendix 1, 2, 3, 4 and 5
34
BUDGET JUSTIFICATION
Upgrading the CVL, KEMRI, and UON-FVM laboratories to BL-3 with capability to handle
HPAI is a critical and immediate need.
The CVL laboratory has facilities for HI and IFA and virus culture for avian diseases, but
currenly operates at BL-2 level. There are therefore, major bio-safety issues relating tothe
handling of HPAI strains (H5N1). As a first line of defense the National Taskforce requires this
facility be upgraded to a BL-3. There is also a need for diagnostic reagents for H5N1 and
training for the staff.
The KEMRI laboratory is a BL-2 facility but performs cell culture, HI, and IFA for human
influenza viruses. Presently, the laboratory can routinely detect A and B subtypes, and H1N1 and
H3N1. Like CVL, KEMRI has no HI or IFA reagents for detecting H5N1.
The requested 20 million shillings for upgrading the two laboratories is based on the cost of
upgrading the CDC/IEIP laboratory. This includes installation of class II biosafety cabinet,
vented outside with Hepafilter system, non-slippery floors, hand-free sinks, double doors and
shower-in shower-out systems. In addition, the laboratories would be installed with negative
airflow in the isolation laboratory with Hepafilter system and decontamination units for annual
cleaning and re-certifications.
Upgrading the UON-FVM laboratory (Kshs 10 million), which handles a significant number of
domestic poultry, would be advantageous for two reasons. First, being a University laboratory,
the UON-FVM laboratory is likely to attract private funding to sustain itself longer. Second, the
anticipated number of animal specimens (migratory birds, domestic birds, and pig) is large and it
makes sense to have two laboratories commissioned to undertake primary diagnosis for animal
influenza, with ILRI laboratory providing molecular diagnosis back up.
Reagents and consumables for the 4 laboratories (Kshs 103 million over 5 years) are requested to
ensure sustained AI detection system for the next 5 years. The CDC/IEIP laboratory will work
with the CVL laboratory to improve the sensitivity of their egg inoculation and HI detection
system by providing additional PCR screening for all their samples for the next 6 months. In
addition, CDC/IEIP laboratory will transfer PCR (conventional and real-time) activities for
animal specimens to ILRI laboratory. This activity transfer will ensure sustained diagnostic
capacity for a long time to come. Similar assistance will be provided to UON-FVM laboratory.
The biosafety requirements (Kshs 22.6 million over 5 yrs) and training requirements (Kshs 8
million over 5 yrs) are essential for protecting the first responders in rural areas of Kenya
(veterinarians, clinicians, nurses). Logistical support (Kshs 31 mill over 5 years) involves
purchasing two vehicles, one for DVS and another for DMS dedicated to AI in order to ensure
fast and timely response to die-off collections and collection of specimens (human, animal) from
hard-to reach areas of the country.
35
LABORATORY PROGRAMME WORK PLAN
ACTIVITY
SUB-ACTIVITY
BY WHOM?
BY WHEN
EXPECTED OUTPUT
PERFORMANCE
MOV
ASSUMPTIONS
Expertise exist in each
lab
Timely procurement
INDICATORS
Capacity building
Personnel safety
Harmonize SOPs
between labs
Acquire
reagents
and consumables
Training
on
biosafety
Laboratory
directors
DVS
and
DMS
Laboratory
directors
Jan 30 ‘06
Vaccination
Provision of PPE
Laboratory
and
environmental safety
Laboratory upgrade to
BL-3 (CVL,KEMRI,
UON)
Advanced
GLP
training
Improved
waste
management
Expert consultation
Drawing of plans
Pre-construction
preparations
Laboratory-based
HPAI
prevalence
determination
Data analysis
IQA and EQA
New
questions
Laboratory upgrade to
BL-3 (CVL,KEMRI,
UON)
research
Constructions
SOPs available with
laboratory directors
Materials in place
SOPs
Jan 30 ‘06
Laboratory
SOPs
harmonized
Required
material
acquired
Staff trained in
Observance of safety
procedures
Trainers are available
DVS
and
DMS
DVS
and
DMS
Laboratory
directors
DVS
and
DMS
DVS
and
DMS
Experts and
MOW
Experts, DVS,
DMS
Immediate
Staff immunized
Immediate
Staff protected
Personnel don’t come
down with disease
PPE in use
Training
progress
report
Safety
procedure
Manuals
Immunisation records
PPE records
Timely procurement
Jan 30 ‘06
Staff trained on GLPs
Jan 30th ‘06
Waste
management
system in place
Experts consulted
Training
progress
report
Inventory reports
Trainers are available
Immediate
Good safety procedures
in place
Incinerators and biopits functional
Experts report
Experts report
Expertise available
April 30th ‘06
Blueprints
Blueprints in place
Blueprints
Expertise available
April 30th ‘06
Timely
process
Continuous
- Tender report
Construction
materials in place
Laboratory
reports/manuscript
Laboratory
reports/manuscripts
Inventory reports
Laboratory
directors
Laboratory
directors and
collaborators
Laboratory
directors/epid
emiologist
Experts, DVS,
DMS
- Tendering done
Construction
materials in place
Data analyzed
Laboratory reports and
records
Laboratory reports and
records
Expertise available
New proposals
funding
Challenges
requiring
research will emerge
Feb 28th ‘06
IQA-continuous
EQA-annually
Reproducible results
Continuous
New research areas
Proposals in place
Dec 31st ‘07
BL-3 laboratories at
KEMRI, CVL, UON
BL-3 laboratories at
KEMRI, CVL, UON
Inventory reports
for
Actual Structures
Construction
reports
Vaccine available
Timely installation
tendering
Expertise available
Expertise & materials
available
36
INFECTION PREVENTION AND CONTROL
INTRODUCTION
Infection prevention and control (IPC) services provide the means to break the chain of infection
and limit spread of an infectious disease. This is a key strategy in control of communicable
diseases. IPC involves the observance of standard transmission precautions in addition to efforts
to eliminate infective agents.
Avian Influenza is a viral infectious disease. As a viral disease, there is no effective anti-viral drug
so far developed. Currently a vaccine against the culprit Highly Pathogenic Avian Influenza
(HPAI) virus responsible for the new epidemic has not been developed. Therefore, IPC remain a
central strategy to the control efforts of the epidemic.
VISION
To ensure that Kenya remains HPAI free
MISSION
To put in place mechanisms to prevent introduction of HPAI and in case of occurrence; control
transmission at source including stamping out
GOALS
1. To prevent introduction of HPAI into the country, that would affect wild and domestic
birds and human beings.
2. To develop strategies for control of HPAI in the event of an outbreak
OBJECTIVES
To put in place quarantine and isolation facilities
To establish a vaccination programme for both birds and humans
To provide sanitary regulations and guidelines to all farmers
To establish an effective culling and compensation system
To train technical (animal and human health) workers on IPC
To put in place strategic stocks of protective gear & disinfectants
SWOT ANALYSIS
Strengths
A National Avian Influenza Task force in place
Qualified technical man power in place
A clear quarantine policy for sick animals
Epidemio-surveillance system in place both with the DVS and IDSR
WHO has issued guidelines on EPP for HPAI
OIE has issued guidelines on regulation of trade in Livestock and their products
Training mechanisms are in place
Weakness
Insufficient technical staff in some areas
Weak quarantine policy for humans
Infection Prevention and Control committees in most hospitals not activated
37
Lack of isolation units in hospitals
Lack of quarantine facilities in some ports of entry
Inadequate financial allocation
Inadequate legal provisions in the current laws
Opportunities
High level of awareness in the community
Experiences with preparedness in the face of previous global threats e.g. Ebola and SARS
Interest from the international community
Threat
Migratory birds whose movement cannot be controlled
Lack of sustainability of preparedness and response programme
Assumptions
Continued goodwill from the government
Continued goodwill from development partners
That neighbouring countries will equally apply preparedness and response measures That
neighbouring countries cooperate share experiences
An effective vaccine against H5N1 will be available soon
Adequate stock of Tamiflu anti-viral drug will available
Constraint
Protective material and gear are very expensive
38
INFECTION PREVENTION AND CONTROL WORK PLAN
1.
Activity
Sub activity
Item
Prevent
introduction of
HPAI virus into
the country
Ban imports
from infected
country
Demand risks
assessment from
exporting country
Establish
quarantine
stations at ports
of entry
Domestic & wild
birds & their
products
Risk assessment
report
Strengthen the
inspection of
imports at ports
of entry
Protect personnel
investigating
HPAI
Prevent
transmission of
HPAI from
contaminated
surfaaes and
materials
Ensure no HPAI
introduced
through Swill
Ensure no HPAI
introduced
through Fomites
Ensure no HPAI
introduced
through animal
By
Who
DVS
By When
Expected Output
Indicators
immediate
No imports from
infected countries
,,
immediate
immediate
Imported Avian
products
KAA,
KPA &
DVS
KAA,K
PA &
,DMS
KRA &
DVS
Issue protective
gear
DVS /
DMS
Decontaminate
areas suspected of
contamination
DVS
Decontaminte swill
from aircrfts and
ships
Animal quarantine
Human quarantine
Safely dispose off
swill
Public education
on fomites that
may carry HPAI
Demand sanitary
certificate from
exporting countries
Assumptions
No. DVS import
licences
Means of
Verification
Inspection records at
ports of entry
Awareness on risk
status of exporting
countries
Quarantine facilities
in place
No of reports
received
Physical inspection of
reports at DVS
No of facilities put in
place
Establishment reports
Exporting will
cooperate and be
transparent
Funds will be
available
immediate
Inspections
strengthened
No. of inspection
reports
Physical inspection of
reports
No illegal imports
into the country
immediate
Personnel are
protected
No of gear issued
Stores records
Gear available
DMS
DVS,
KAA,
KPA
DMS
immediate
Aircrafts and ships
are not HPAI
contaminated
Disinfection
schedules
Disinfection
certification reports
Appropriate
authorities in place to
certify disinfection
immediate
All swill safely
disposed off
Quantities disposed
Disposal schedules
All swill is declared
DMS &
DVS
immediate
DVS
immediate
only safe animal feeds
premixes imported
No of sanitary
certificates presented
KRA & DVS records
No illegal imports
into the country
No illegal imports
into the country
immediate
39
Activity
Sub activity
Item
By
Who
By When
Expected Output
Indicators
Means of
Verification
Assumptions
Feed premixes
International
travel
2
3
4
Prevent infection
of domestic birds
and other
susceptible
animals
Prevent HPAI to
humans
HPAI outbreak
response
DMS,
DVS,
KAA,
KPA
DVS
Create awareness
and encourage
confinement of
domestic bird
Procure doses of
seasonal vaccine
to vaccinate
people at risk
Stop inerraction
between HPAI
infected and the
non-infected
Provide for
compensation of
culled birds
during outbreak
response
Disposal of
culled/dead birds
Engage extra
staff to cope with
increased
workload
Limit
transmission of
disease through
poultry
movement
Stop
consumption of
Order human
influenza vaccine
DMS
immediate
People at risk
vaccinated
No of people
vaccinated
DMS reports
Vaccine supplies and
funds available
Issue quarantine
advisories
DMS
when
necessary
Infected individuals
observing travel
restrictions
No of people on
travel restrictions
DMS reports
Field staff to
supervise quarantine
Review animal
diseases act cap
364
DVS
immediate
Compensation
catered for in cap 364
Legal ammendment
available
Gazette Notice
Political support
available
Inceneration or
burial &
decontamination of
the area
Hire extra Vet&
Health Personnel
DVS
when
necessary
No nuisance of
carcasses of birds
No of disposed birds
Disposal reports
Wild scavengers will
not eat the dead birds
DVS &
DMS
when
necessary
Extra staff hired
No hired
Employment records
Resources available
and staff will agree to
set terms
Enforce poultry
movement control
DVS
when
necessary
Poultry movement
controlled
No of movement
permits issued
DVS Reports
Compliance from the
general public
Enforce poultry
inspection
DVS
when
necessary
Safe poultry
consumed in the
No of poultry
inspections
DVS Reports
Compliance from the
general public
40
Activity
5
6
7
8
Sub activity
HPAI infected
poultry
Protect birds
from HPAI
Limit
transmission of
disease to
humans
Protect personnel
in contact with
HPAI from
infection
Prevent hospital
acquired
infection with
HPAI
Item
By
Who
By When
Expected Output
Indicators
Means of
Verification
Assumptions
No of birds
vaccinated
No of people
vaccinated
DVS Reports
Compliance from the
general public
Epidemic vaccine
avalaible
country
when
necessary
when
necessary
Vaccinated birds
DMS/
DVS
when
necessary
Personnel are
protected
No of gear issued
Stores records
Issued to the right
personnel
2 national referred
hospital
8 provincial
hospital
6 district hospitals
DMS
immediatel
y
Medium
term
Long term
Isolation units
established
No of units
established
DMS Reports
Funds are available
Equip and
furnish the
isolation units
See list of items
DMS
when
necessary
Isolational units
operational
No of isolation units
DMS Reports
Funds available
Provide logistical
support to IPC
sub committee
Provide transport
facilitation
immediatel
y
Medium
term
immediatel
y
Amount allocated
Financial records
Funds available
Additional vehicles
purchased
Awareness amongst
stakeholders created
No procured
DMS & DVS Reports
Funds available
Create general
awareness among
stakeholders
Train the
technical
personnel
DVS &
DMS
DVS &
DMS
DVS &
DMS
Transport available
Build human
capacityto cope
with HPAI
Cater for transport
costs
Proccure additional
vehicles
Hold sensitisation
forums
No sensitised
DMS & DVS Reports
Cooperation by
stakeholders
Hold staff update
& consultative
meetings
DVS &
DMS
immediatel
y
Technical staff
competent to deal
with HPAI
No updated
Training reports
Funds available
Put up isolation
units for Avian
Influenza
Operationalise
the isolation units
Vaccinate birds at
risks
Vaccinate 10% of
human population
at risk
DVS
Provide protective
gear
DMS
DMS
DMS
People at risk
vaccinated
DMS reports
DMS
41
INFECTION PREVENTION AND CONTROL BUDGET SUMMARY
Activity
Immediate Budget
(Kshs)
Medium Term
Budget (Kshs)
Long Term Budget
(Kshs)
7,600,000
19,200,000
9,100,000
0
0
0
6,200,000
11,600,000
8,800,000
1
Prevent introduction of HPAI into the country
2
Prevent infection of domestic birds and other susceptible animals (*)
3
Prevent HPAI to humans
4
Respond to an HPAI outbreak
15,000,000
1,072,400,000
725,110,000
5
Put up isolation units for Avian Influenza
13,500,000
36,000,000
12,500,000
6
Strengthen National IPC secretariat
0
11,470,000
0
7
Operationalise the isolation units
0
0
0
8
Provide logistical support to IPC sub committee (*)
0
0
0
9
Build human capacityto cope with HPAI (*)
0
0
0
42,300,000
1,150,670,000
755,510,000
TOTAL
42
CASE MANAGEMENT
INTRODUCTION
Case management is care and treatment of a patient admitted with HPA1 virus infection.
It includes:
Clinical diagnosis
Specimen collection for laboratory confirmation of the clinical diagnosis
Admission procedures and referral where necessary
Drug treatment whether in-patient or out patient
Care while in hospital that includes preventive precautions to prevent spread of infection
Referrals and transfers where necessary
Discharge protocols and procedures
VISION
All or almost all people who contract the HPA1 virus infection survive through intensive case
management in selected health facilities
MISSION
Establish and sustain capacity for effective case management of HPA1 virus infection in health
facilities in Kenya
PROBLEM STATEMENT
1. There is an impending threat of HPAI virus infection in Kenya, which is likely to turn
into an epidemic or a pandemic.
2. There is inadequate capacity to handle such a situation
GOAL
To achieve a (hundred percent) 100% survival rate
OBJECTIVES
1. Develop case management guidelines
2. Improve infection prevention and control standards in health facilities
3. Well equipped isolation wards established
4. Develop referral standards and guidelines
SITUATION ANALYSIS
The country is divided into seven HPA1 virus high risk zones based on migratory patterns of
birds form Europe and Asia
These are:
1. North Western migratory route covering Turkana and Marsabit districts
2. Nyanza and western migratory routes around L. Victoria and Ahero
3. Central Rift Valley covering lakes Baringo, Bogoria, Elementaita, Nakuru, Naivasha and
Magadi
4. Amboseli region covering the national park and its surrounding area.
5. Nairobi and central highlands covering south Kinangop and surrounding wet lands
6. Tsavo covering lakes Jipe, Ngulia, other pools and wet lands
7. Coast region covering Watamu. Mombasa, Malindi and Kilifi
43
Health facilities in these seven zones lack adequate isolation facilities to facilitate ideal case
management of HPA1 virus infection. In these seven areas, the following eight (8) hospitals have
been identified.
North Western Zone – 2 hospitals have been identified due to large geographical bio diversity.
They are:
1. Lokichoggio ICRC hospital
2. Marsabit District hospital
3. New Nyanza General Hospital
4. Nakuru Provincial General Hospital
5. Narok District Hospital
6. Kenyatta National Hospital
7. Voi District Hospital
8. Port Reitz District hospital
HPA1 virus is highly contagious and the eight identified hospitals in the seven zones will be used
to provide care and treatment for these patients. This is necessary because such patients require
isolation from the rest of the public until they recover fully to prevent spread of the infection.
These hospitals therefore require well equipped isolation wards and currently only KNH has one
which is ill equipped.
These hospitals have all cadres of health personnel but they have not been trained on
identification and management of HPA1 virus infection which is a new disease in Kenya.
There is need to develop guidelines on case management, referral and drug management.
Each of the high risk regions covers large geographical areas with high population and several
health facilities which could diagnose a suspected case. This therefore calls for a stand by
ambulance within the zonal hospital specifically meant for quick transfer of such patients.
The same facilities identified also need to be provided with full communication equipment to link
them with the rest of the facilities in their zones.
44
CASE MANAGEMENT WORK PLAN
Objectives
Activities
Develop case
management
guidelines
Set up a task force
to develop the
guideline
Improve infection
Prevention in the
health facilities
Develop training
curriculum
Provide update
trainings for
healthcare
providers
Purchase specially
designed
ambulances
Well
equipped
isolation
wards
established
Set up isolation
wards
Sub-objectives
By who
By When
Output
Hold 8 meetings
DMS
Task force in place
Three Workshop
DMS
Last week of
October
2005
Nov 2005 to
Feb 2006
Printing and
publishing of
guidelines
Set up task force to
develop the
curriculum
DMS
April 2006
Guidelines published
DMS/CNO
February
2006 to
March 2006
Task force in place
Workshops
conducted
Number of meetings
held
Print and publish
curriculum
DMS/CNO
April 2006
Curriculum available
Conduct Training
of Trainers (ToT)
Conduct training
for healthcare
providers
Develop ambulance
design/specificatio
n
Procure and supply
specially designed
ambulances
Develop design of
the isolation wards
DMS/CNO
March 2006
ToTs trained
DMS/CNO
Healthcare providers
trained
DMS
From April
2006 to Dec.
2006
January 2006
DMS
August 2006
DMS/MoP
W
February
2006
Number of
ambulances
purchased
Design developed
Put up the
buildings
Purchase and
supply equipment
Purchase and
supply infection
DMS/MoP
W
DMS
August 2006
Wards completed
September
2006
Wards equipped
Design developed
Performance
Indicators
Number of meetings
held
MoV
Assumptions
Minutes of meetings
Funds will be
available in time
Number of
workshops
conducted
Guidelines available
in clinical areas
Draft guidelines
developed
“
Observable
“
Number of meetings
held
Minutes of meetings
held
“
Curriculum
developed
Number of copies of
curriculum
distributed
Number of ToTs
trained
Number of
healthcare providers
trained
Copy of design
available
Curriculum in place
Copy of design of
ambulance
The design will be
available
Specially designed
ambulances
purchased
Design of the
isolation ward,
developed
Wards incomplete
Log books of
purchased
ambulances
Copies of the
designs
Funds will be availed
Number of wards
put up
List of equipments
purchased
Wards will be put
up as per design
Funds will be
available
Equipment
purchased
Register of number
of curriculum copies
distributed
Training reports
Training reports
Training curriculum
developed in time
-
Designs will be made
Ass planned in the
Infection prevention
45
Objectives
Activities
Sub-objectives
prevention
requirements
Purchase and
supply nopharmaceuticals
items
Purchase and
supply drugs
Develop
referral
standards and g
uidelines
Set up a technical
task force for
patients referral
guidelines
Hold 8 meetings
Printing and
publishing of the
referral manual
By who
By When
Output
Performance
Indicators
MoV
Assumptions
Items available
Items purchased
List of items
purchased
Funds will be
available
Items available
Drugs are bought
Lists of drugs
bought
- Drugs will be
available
and control plan
DMS
DMS
DMS
DMS
Emergency
con. Jan
2006.
The rest –
August 2006
Emergency
con. Jan
2006.
The rest –
August 2006
End of
December
2005 to end
of February
2005
April 2006
- Funds will be
available
Task force in place
Guidelines
developed
Guidelines published
Number of meetings
held
Guidelines
developed
Minutes of meetings
held
Copies of guidelines
developed
Referral manual
published
Number of copies of
referral
Funds will be
available
46
CASE MANAGEMENT BUDGET SUMMARY
Immediate Budget
(KShs)
24,000
Medium Term Budget
(KShs)
0
Long Term Budget
(KShs)
0
159,000
3,000,000
0
1,800
0
0
0
3,840,000
0
0
8,000,000
8,000,000
2.1 Buying drugs
37,500,000
592,500,000
592,500,000
2.2 Supportive drugs
44,368,740
0
0
0
1,404,230,000
2,808,460,000
2.3 Buy non-pharmaceuticals
7,500,000
0
0
3.1 Setting up isolation wards
75,000
26,000,000
54,000,000
0
0
48,000,000
3.2 Buy Equipments for the isolation wards
4.1 Setting up Technical Task force on
Referral guidelines
4.2 Purchase of 8 Special Ambulances
0
20,708,680
0
24,000
3,000,000
0
40,000
12,000,000
12,000,000
GRAND TOTAL
89,712,540
2,073,278,680
3,522,960,000
Activity
Setting up a technical taskforce
1.2 Developing Curriculum
20,000
1.3 Training of Health Workers
47
INFORMATION, EDUCATION AND COMMUNICATION
SITUATION ANALYSIS
There have been outbreaks of Avian Flu in several countries, especially in Asia, where some of
the cases resulted in fatalities. In view of this, governments worldwide have been putting systems
and controls in place in order to mitigate its expected effects.
STATEMENT OF FUNCTION
The Information, Education and Communication (IEC) Sub Committee was constituted
alongside five other sub committees of the National Preparedness Task Force to create
awareness, sensitisation and education to the Kenyan public on the Highly Pathogenic Avian
Influenza (HPAI). These awareness functions are to be executed in close coordination with other
sub committees.
STATEMENT OF PURPOSE AND MANDATE
On 26th October 2005, the Government of Kenya established a National Preparedness Task
Force co-chaired by the Ministries of Livestock and Fisheries Development and Health. This
National Task Force was mandated to carry out activities such as surveillance and epidemiology
(Avian and human), prevention and control, case management, laboratory, research, IEC and
Resource Mobilisation functions.
The IEC Sub Committee is mandated;
1.
2.
3.
4.
To develop a risk communication strategy that addressed different target groups.
To establish and manage an official HPAI Website.
To undertake media monitoring and develop appropriate media briefings.
To establish a partnership with both local and international media houses to disseminate
information on HPAI.
5. To coordinate the development of appropriate IEC materials.
6. To facilitate preparation of media briefs and press statements by the official
spokespersons.
7. To facilitate media coverage of activities being undertaken by the various subcommittees.
STATEMENT OF STRATEGY
The statement of strategy involves the following action points:
a. Establishment and manning of a Media Centre
b. Conducting Research Analysis and Media Monitoring
c. Carrying out Social Mobilisation
d. Mass Media campaigns
e. Production and distribution of IEC materials
f. Establishment and maintenance of an HPAI Website
VISION
Proper management of information on HPAI so that Kenya’s economy is not affected in any way
by panic arising from false information or rumours and that all Kenyans become active
participants in the country’s rapid response plan to tackle the HPAI threat
MISSION
To respond countrywide through effective, efficient and appropriate public sensitisation and
awareness tools.
48
GOAL
Kenyans are adequately and correctly sensitized and informed about Highly Pathogenic Avian
Influenza (HPAI).
OBJECTIVES
1. To develop the Media Centre
2. To educate and disseminate accurate information timely to the general public and other
stakeholders about HPAI
3. To prepare education materials for the public
4. To build capacity of all persons who will be involved in the Information dissemination
and social mobilization programs
5. To collect and collate information on HPAI
6. To maintain a data bank of HPAI related issues
7. To ensure stakeholders are interlinked for information exchange
8. To communicate to the public through any appropriate languages
9. To communicate to the public simplified messages
10. To correct any misconceptions on bird flu
11. To use all available media
SWOT ANALYSIS
Strengths
a. Availability of highly trained personnel to man the Media Centre
b. Availability of materials on HPAI
c. Kenya is covered by vast mass media,
d. Already existing IT structures
Weaknesses
a.
b.
c.
d.
e.
Lack of resources
Untimely release of funding
Illiteracy of the populace
Media politics and priorities
No media center
Opportunities
a. Willingness of media houses to disseminate information to the general populace
b. Partners willing to support the HPAI budget
c. Widespread civil society network in Kenya
d. Donor funding
e. Government goodwill
f. Public expectant of information
g. Immense global information on HPAI
Threats
a. Incorrect HPAI messages in media and within the population
b. Minimal awareness of bird species both local and migratory
c. Lack of funds
BUDGET JUSTIFICATION
Media Centre
49
The Media Centre shall be developed and maintained by the members of the IEC sub committee
in collaboration with relevant members of the National Task Force. It will serve as a nerve centre
from which information will be managed and flow systematically to the general public. This
information flow will include press statements and interviews, production of IEC materials and
any other media related issues. This will ensure that information is properly managed. The centre
shall ensure that the Website is updated with the latest information, which shall be accessed by
both local and international media, as well as the general public.
It is expected that the Media Centre will be fully equipped to ensure that the work is
implemented effectively and efficiently.
Research
The Media Centre shall collect, collate and utilise information for the purposes of designing a risk
communication strategy. This initial material will also be used to develop useful tools for
dissemination activities. This research stage will include media monitoring and analysis on the
ongoing HPAI interest issues, which would be essential for gauging the information disseminated
to the Kenyan public.
Social Mobilisation
Noting that social mobilisation is a necessary tool in such a campaign, therefore stakeholders,
partners, policy makers and all other relevant groups will be actively involved. Communities
living along the migratory route of the birds will be targeted as a priority. The committee will also
be targeting communities, in both rural and urban areas, where there is close interaction between
humans and poultry. 20 districts have been identified and will be targeted for initial awareness
campaigns. These numbers of districts can either increase or decrease depending on the HPAI
situation in the country.
Other players in the NGO sector shall also be actively involved in the implementation on the
ground of the social mobilisation activities.
Mass Media
The mass media is a vehicle for sensitising small and large numbers of people spread across the
country. These media include; Radios, TVs and Newspapers. Noting that language is of critical
importance in this campaign, these media shall be used to reach the rural communities with
structured messages in the local dialects. Newspaper supplements and advertisements are crucial
to maintaining a concerted approach to enlightening the public. It is important that these
campaign tools are done in the initial stages of the campaign. Free interviews are expected to be
conducted through the goodwill of the mass media, including radio, television and newspapers.
At the same, the Media Centre, through the National Task Force, shall seek and gain mutual
support from other government institutions, the corporate sector and the media to ensure
success of the activities.
50
IEC COMMITTEE WORK PLAN
1
Activity
Sub-activity
Detail
Research
(a) Formative
1. Focussed Group
Discussion (FGD)
Action by Time
frame
Media
Dec 05Centre
Jan 06
2. Questionnaires
(b) Media monitoring
2
Mass media (Radio) (a) Radio interviews
Mass media (TV)
Interviews in radio
shows
Media
Centre
(b) Radio programmes Radio presentations by
experts
(c) Radio spots
Short, 1-minute
adverts
(d) Production
Independent
Production of radio
programmes
(a) TV Spots
Short, 1-minute
Media
adverts
Centre
(b) TV Documentary
(c) TV interviews
Print media
Content analysis in all
mass media
(a) Supplements
Indicators (targets) Means of
verification
Research carried out to
10 FGDs conducted 10 FGDs reports
help design risk strategy, as
prepared
well as assess the situation
obtaining regarding HPAI.
Questionnaires
Reports on
prepared and distri
administration of
buted
Questionnaires
received
Short,
Clips assist in analysing
Clips from all media Clips collected and
Medium, information flow, and
houses collected and archived
Long term desiging of risk
collated.
communication strategy
Dec 05To sensitise and inform the Approx. 10 radio
Radio shows and
May 06
public on HPAI. The
shows
spots are Aired,
(Through public is also sensitised in
recorded and
out the
English, Kiswahili and any
archived
campaign) other relevant language.
Approx. 15 radio
programmes
100 spots gone on
air
100 productions
Radio shows and
conducted
spots produced
Assumptions
(risks)
Funds
Dec 05May 06
(Through
out the
campaign)
TV shows,
documentaries and
spots are produced,
aired, recorded and
archived
Media goodwill
Supplements
published and
archived
Media goodwill
Independent
Production of radio
programmes
Interviews on TV with
experts
Supplement in all the
daily newspapers
Media
Centre
Dec 05May 06
(Through
out the
Expected output
To sensitise and inform the 12 spots aired in 4
public on HPAI. The
TV stations
public is also sensitised in
English and Kiswahili
languages.
3 TV productions
done
3 interviews held in
4 stations, and aired
in English and
Kiswahili
To sensitise and inform the Supplements in 4
public on HPAI. The
dailies and one
public is also sensitised in Kiswahili
English and Kiswahili
Media goodwill
51
campaign) languages.
(b) Advertisement
3
IEC materials
4
Media Centre
5
Social Mobilisation
(a) Developing of
IECs
(b) Printing and
distribution of IEC
materials
Establishing and
Equipping Media
Centre
Website
Media
Centre and
members
of other
subcommittee
s
Dec 05May 06
(Through
out the
campaign)
To facilitate the effective
and efficient execution of
media and awareness
campaigns.
printed IEC
materials
One million IEC
materials printed and
distributed
Media Centre
Media Centre
established and
established,
equipped
equipped and
functional
Media
Centre
Community
mobilisation in 20
districts
Conduct public
Barazas, meetings and
FGD, in churches,
institutions, organised
groups
MoH,
MoLFD,
CBOs,
NGOs,
Advocacy meetings
Conduct advocacy
among media,
partners, policymakers, poultry
industry stakeholders,
and other key groups
Conduct meetings for
experts in the poultry
industry and medical
fields, both animal and
human.
Developing, Software
and Hardware,
maintaining
Media
Centre
Dec 05May 06
(Through
out the
campaign)
Media
Centre
Medium
term
To keep abreast with the
10 meetings held
developments in the HPAI
threat.
Meetings held and
cooperation of
information updated partners
successfully.
Media
Centre
Medium
term
To facilitate the effective
and efficient publicity
campaigns, as well as used
as an educational tool for
the Kenyan public.
Website established, Setting up of the
updated and
media centre and
maintaned.
coordination with
other committees
Establishing and
Maintenances
Dec 05May 06
(Through
out the
campaign)
Dec 05May 06
(Through
out the
campaign)
To sensitise and inform the IEC materials
public on HPAI. The
developed
public is also sensitised in
English and Kiswahili
languages and any other
relevant language.
Computers,
communication and
stationery.
Experts meetings
6
Adverts in all the daily
newspapers
Posters, fliers,
brochures, fact sheets,
pamphlets, banners, Tshirts, caps, label
stickers, quarantine
stickers, quarantine
ribbons, guideline
manuals,
To mobilise and sensitise
the public on HPAI. The
public is also sensitised in
English and Kiswahili
languages.
20 districts mobilised Mobilisation
for activities
successful, people
participate actively
and information
about HPAI adopted
in the communities.
To advocate on the
10 meetings held
Meetings held and
immediate concerns of the
advocacy
HPAI threat.
successfully
conducted.
Website set up and
utilised
Funds
Funds
Community
cooperation
cooperation of
partners
52
IEC MATERIALS
IEC materials shall be developed, printed and distributed through the Media Centre. These
materials include; Posters, fliers, brochures, fact sheets, pamphlets, banners, T-shirts, caps, label
stickers, quarantine stickers and ribbons. All IEC materials required by National Task Force will
be prepared with the consultation of the IEC Sub Committee. This will ensure accurate
information that is well edited and designed for the targeted audience.
BUDGET DEVELOPMENT
No
Activities
Short term
Medium term
Long term
1
Research
2,000,000
1,000,000
1000,000
2
a. Mass Media (Radio)
4,000,000
9,000,000
3,100,000
b. Mass Media (TV)
2,160,000
34,500,000
16,500,000
0
5,000,000
3,000,000
c. Mass Media (Print)
3
IEC Materials
1,020,000
22,000,000
1,000,000
4
Media Centre
580,000
350,000
200,000
5
Social Mobilisation
9,360,000
24,000,000
22,000,000
6
Website
680,000
1,000,000
200,000
20,000,000
96,850,000
47,750,000
TOTAL
Collaboration and Coordination
The Media Centre will not work in isolation, but rather in consultation with the National Task
Force and its sub committees.
Gaps and Constraints
The Media Centre is working with the assumption that funding will be made available to
effectively and efficiently execute the work plan.
Programme Implementation and Monitoring
It is envisaged that this programme will be implemented in the short term (0-6 months), medium
term (6 months-2 years) and long term (2-5 years). The members of the Media Centre shall be
mandated to conduct implementation and monitoring activities.
Way forward
The members of the Media Centre will be part of the concerted countrywide effort to tackle the
HPAI in the short, medium and long-term basis.
No
Approved Budgets for Sub Committees for the immediate term
Amount in Kshs
1
Infection Control
28,000,000
2
Epidemiology and Surveillance
61,120,000
3
Laboratory
43,240,000
4
IEC Materials
20,000,000
5
Case Management
92,500,000
6
Coordination
4,892,500
Total
249,752,500
53
SUMMARY AVIAN FLU GUIDELINE
What is Flu?
Influenza flu is a contagious respiratory illness caused by the influenza viruses. Some people,
such as older people, young children, and people with certain health conditions, are at high risk
for serious flu complications.
About the Influenza Flu Viruses
Influenza A and B are the two types of influenza viruses that cause epidemic human disease.
Influenza B viruses are not categorized into subtypes. Since 1977, influenza A (H1N1) viruses,
influenza A (H3N2) viruses, and influenza B viruses have been in global circulation. New
influenza virus variants result from frequent antigenic change (i.e., antigenic drift) resulting from
point mutations that occur during viral replication. Influenza B viruses undergo antigenic drift
less rapidly than influenza A viruses.
Antibody against one influenza virus type or subtype confers limited or no protection against
another type or subtype of influenza.
Symptoms of Flu
fever (usually high)
headache
dry cough
Case Definitions of Flu
Cough
Fever
Influenza in close contacts
World Health Organization Case Definitions for Influenza
Suspected:
a case that meets the clinical case definition
Flu Transmission
A combination of infection control strategies is recommended to decrease transmission of
influenza in health-care settings. These include placing influenza patients in private rooms when
possible and having health-care personnel wear masks for close patient contact (i.e., within 3 feet)
and gowns and gloves if contact with respiratory secretions is likely. The use of surgical or
procedure masks by infectious patients may help contain their respiratory secretions and limit
exposure to others. Likewise, when a patient is not wearing a mask, as when in an isolation room,
having health-care personnel mask for close contact with the patient may prevent nose and
mouth contact with respiratory droplets. However, no studies have definitively shown that mask
use by either infectious patients or health-care personnel prevents influenza transmission. Flu
viruses spread in respiratory droplets caused by coughing and sneezing. Flu in Kenya
Influenza Flu outbreaks recorded in Kenya
October 2003
Kijabe Hospital
March 2004
Kambaa Girl’s High School
Vaccination
54
Influenza “B” isolated
Influenza “B” isolated
The single best way to prevent the flu is to get a flu vaccination each fall. The "flu shot" -- an
inactivated vaccine (containing killed virus) that is given with a needle. The flu shot is approved
for use in people older than 6 months, including healthy people and people with chronic medical
conditions.
All health care workers
Clinical Management of Influenza
Clinical Presentation in Babies and children
Primary influenza pneumonitis can be a presenting diagnosis.
Complications of influenza
Respiratory: respiratory failure, bacterial superinfection, viral pneumonia
Differential diagnosis of influenza
Triaging at the influenza assessment/admission area
Designate a separate assessment/admission clinic for patients with suspected influenza. Patients
referred with “flu” should proceed directly to this area, and those with symptoms of influenza
should be rapidly diverted here to minimise transmission to others in the waiting room.
Divert patients requiring resuscitation to the usual emergency department area.
Admission pro-forma
A risk assessment classifying patients accordingly
Essential epidemiology (including vaccination history– pneumococcal, influenza)
Blood culture
Electrocardiograph in patients with ischaemic heart disease, or older, or sicker.
Fluid intake
Ensure increased fluid intake.
All confirmed and suspected cases of influenza or
All confirmed and suspected cases of influenza in the following groups:
All essential workers (including health care workers).
The symptoms of uncomplicated influenza – fever, mild dyspnoea, pleuritic pain, blood tinged
sputum, scattered lung crackles – all suggest possible bacterial lung involvement.
65
Available as 100mg capsules
Dosage:
Treatment 100mg 12hrly for 5-7 days
100mg 24hrly in renal impairment, 10-15 years or over 65 years 2-4mg/kg in children 1-9 years
(syrup), maximum 100mg daily
Prophylaxis 100mg 12hrly for period of time during which protection is required, or 10 days
after vaccination
Available as 100mg tablets and syrup 50mg/5mL
Dosage:
Treatment 100mg 12hrly for 5 days
Available as a metered dose diskhaler, 10mg per dose
Dosage:
Treatment 10mg bid by diskhaler 5 days
Antiviral Drugs - Dosage Regimens
Available as 100mg capsules
Dosage:
Treatment 100mg 12-hrly for 5-7 days
55
2-4mg/kg in children 1-9 years (syrup), maximum 100mg daily
Prophylaxis: 100mg 12-hrly for period of time during which protection is required, or 10 days
after vaccination
Available as 100mg tablets and a syrup 50mg/5mL
Prophylaxis: 100mg 12-hrly for period of time during which protection is required, or 10 days
after vaccination
Available as a metered dose diskhaler, 10mg per dose
Data for treatment in children, pregnancy, underlying diseases etc. not yet available.
Infection Prevention and Control and Nursing Care for Flu Patients
Ministry of Health advises strict adherence to barrier nursing practice when handling patients
with Flu.
Suspect cases should wear surgical masks until Flu is excluded.
Wherever possible, patients under investigation for Flu should be separated from those
diagnosed with the syndrome.
Use disposable medical equipment wherever possible in care of patients with Flu. Surfaces soiled
with spills from Flu patients should be decontaminated with an effective disinfectant e.g. 2%
chlorine solution before cleaning.
Health workers must observe standard, respiratory and contact precautions.
Advice to Health care workers on protective apparel when handling flu patients
Wear gloves and mask at all times with a suspected or confirmed case of Flu.
Wear protective eye goggles, mask, gown, waterproof aprons, and head covers during procedures
and patient activities that are likely to generate splashes or sprays of respiratory secretions, blood
or other body secretions or fluids.
Advice to Health care workers on Hand washing
Wash hands before and after significant contact with any patient, after activities likely to cause
contamination and after removing gloves.
Hand Advice to Health care workers on protective apparel when handling wastes from patients
with Flu
Apply standard precautions when handling any clinical wastes.
Restrict visitors but where absolutely necessary the visitors should face masks, goggles, gown and
head covers when in close contact with Flu patients.
Handling a case of Flu
II. Infection Control
Where possible, place a surgical mask on the patient.
All health-care personnel should wear N-95 respirators while taking care of patients with
suspected Flu. If a suspect Flu patient is admitted to the hospital, infection control personnel
should be notified immediately. Infection control measures for inpatients should include:
Standard precautions (e.g., hand hygiene); in addition to routine standard precautions, health-care
personnel should wear eye protection for all patient contact.
Contact precautions (e.g., use of gown and gloves for contact with the patient or their
environment)
Droplet Precautions (e.g., used when a patient is known or suspected to be infected with
microorganisms transmitted by droplets (large-particle droplets {larger than 5 um in size},
generated by coughing, sneezing or talking).
If airborne precautions cannot be fully implemented, patients should be placed in a private room,
and all persons entering the room should wear N-95 respirators.
III. Standard Precautions
Use Standard Precautions for the care of all patients.
56
Handwashing
Wash hands after touching blood, body fluids, secretions, excretions, and contaminated items,
whether or not gloves are worn. Wash hands immediately after gloves are removed, between
patient contacts, and when otherwise indicated to avoid transfer of microorganisms to other
patients or environments.
Gloves
Wear gloves (clean, non-sterile gloves are adequate) when touching blood, body fluids, secretions,
excretions, and contaminated items. Remove gloves promptly after use, before touching noncontaminated items and environmental surfaces, and before going to another patient, and wash
hands immediately to avoid transfer of microorganisms to other patients or environments.
Gown
Wear a gown (a clean, nonsterile gown is adequate) to protect skin and to prevent soiling of
clothing during procedures and patient-care activities that are likely to generate splashes or sprays
of blood, body fluids, secretions, or excretions. Patient-Care Equipment
Handle used patient-care equipment soiled with blood, body fluids, secretions, and excretions in
a manner that prevents skin and mucous membrane exposures, contamination of clothing, and
transfer of microorganisms to other patients and environments. If a private room is not available,
consult with infection control professionals regarding patient placement or other alternatives.
IV. Droplet Precautions
Patient Placement
Place the patient in a private room. When a private room is not available, place the patient in a
room with a patient(s) who has active infection with the same microorganism but with no other
infection (cohorting).
Mask
In addition to standard precautions, wear a mask when working within 3 ft of the patient.
Patient Transport
Limit the movement and transport of the patient from the room to essential purposes only. If
transport or movement is necessary, minimize patient dispersal of droplets by masking the
patient, if possible.
V. Contact Precautions
In addition to Standard Precautions, use Contact Precautions, or the equivalent, for specified
patients known or suspected to be infected or colonized with epidemiologically important
microorganisms that can be transmitted by direct contact with the patient (hand or skin-to-skin
contact that occurs when performing patient-care activities that require touching the patient's dry
skin) or indirect contact (touching) with environmental surfaces or patient-care items in the
patient's environment.
Patient Placement
Place the patient in a private room. When a private room is not available, place the patient in a
room with a patient(s) who has active infection with the same microorganism but with no other
infection (cohorting). Consultation with infection control professionals is advised before patient
placement.
Gloves and Handwashing
In addition to wearing gloves as outlined under Standard Precautions, wear gloves (clean, nonsterile gloves are adequate) when entering the room. Remove gloves before leaving the patient's
environment and wash hands immediately with an antimicrobial agent or a waterless antiseptic
agent. After glove removal and handwashing, ensure that hands do not touch potentially
contaminated environmental surfaces or items in the patient's room to avoid transfer of
microorganisms to other patients or environments.
Remove the gown before leaving the patient's environment. After gown removal, ensure that
clothing does not contact potentially contaminated environmental surfaces to avoid transfer of
microorganisms to other patients or environments.
57
Patient Transport
Limit the movement and transport of the patient from the room to essential purposes only. If the
patient is transported out of the room, ensure that precautions are maintained to minimize the
risk of transmission of microorganisms to other patients and contamination of environmental
surfaces or equipment.
1. Patient-Care Equipment
When possible, dedicate the use of non-critical patient-care equipment to a single patient (or
cohort of patients infected or colonized with the pathogen requiring precautions) to avoid
sharing between patients.
Influenza Surveillance and Epidemiological Preparedness
Scale –up influenza surveillance. Widen the present coverage of the current Influenza Flu
Network covering only Nairobi.
Strengthen all Infectious diseases surveillance
Train surveillance staff on influenza
Surveillance
A timely, representative and efficient surveillance system is the cornerstone of influenza control.
International and regional surveillance
Kenya hosts one of the may WHO Collaborating National Influenza Centres for surveillance on
Influenza, and this laboratory participates in diagnosis and typing of influenza viruses.
has the expertise for rapid definitive identification of influenza viruses, including new pandemic
subtypes;
handles reagents for influenza diagnosis and identification,
maintains up-to-date national information on influenza epidemiology;
Requirements for a national surveillance system
detect increased influenza activity, either epidemic or pandemic. This includes detection of “flulike” illnesses in the community, and the use of laboratory confirmation of influenza infection to
estimate the proportion of these cases that are due to influenza.
rapidly disseminate surveillance results
58