Introduction - Computer-Aided Engineering
advertisement

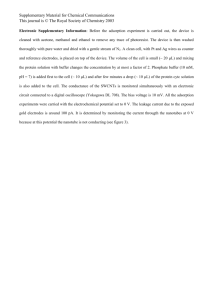
Bladder Contraction Device University of Wisconsin – Madison College of Engineering – Department of Biomedical Engineering Group Members Jeff Delorme Joe Zechlinski Client Wade Bushman, M.D., Ph. D. Urology Advisor John Webster, Ph. D. Biomedical Engineering Table of Contents Page Abstract 3 Introduction 3 Background 4 Client Requirements 5 Problem Statement 6 Proposed Design Solutions 6 Final Design 12 Conclusion 13 References 14 Appendix 15 2 Abstract This report describes a device that will detect the contraction of the bladder during voiding. The proposed design incorporates Ag-AgCl surface electrodes, a differential amplifier circuit, and a data recorder. Current methods/devices of detecting the electrical activity of the bladder are insufficient and no general consensus exists on the effectiveness of measurement technique. We anticipate that our design will succeed in producing a bladder electromyograph since a similar attempt have been successful to some extent. The proposed design has the potential to be a useful tool for our client in his laboratory research. Introduction One of the most common bladder disorders is overactive bladder, or OAB. It is characterized by involuntary contractions of the detrusor, the muscle that surrounds the bladder wall. These contractions cause uncontrollable release of urine. This has a tremendous impact on one’s life. Sufferers are often restricted to areas where bathrooms are close by. Going out in public, whether it is at the gym, at work, or for entertainment can be a worrisome prospect. Frequent bathroom visits also can affect sleep patterns. Those with OAB may reduce their fluid intake in an attempt to curb these problems. OAB has a much more extensive effect on one’s quality of life than many realize. Bladder stones and trauma due to surgery in the pelvic region can contribute to OAB. Generally speaking, however, the fundamental underlying cause is not well understood. miscommunication between the brain and the bladder is blamed for the disorder. 3 Often, a In the United States, OAB affects more than 17 million people. In most cases it can be easily treated. However, many people fail to consult their doctor for help. People who suffer from OAB are often too embarrassed to seek help, or do not know that treatments exist. Background To diagnose OAB, a patient undergoes testing in a urodynamics laboratory. Catheters are inserted to measure pressure in the bladder throughout the voiding process. The electromyography of the bladder is not observed during the testing procedure. This electromyography refers to the electrical signals produced by smooth muscle contractions of the detrusor muscle. A convenient method of obtaining this information is not readily available. Currently, invasive procedures involve attaching electrodes directly to the bladder, or inserting them within the bladder. Inconsistencies arise during measurement as the electrodes move in relation to one another as the tissue contracts. Furthermore, this method is not suitable for use in a urodynamics laboratory. One study was done in the Netherlands in which a non-invasive technique was used (Doorn et al.). Six surface electrodes were placed above the pubic bone to record electrical activity. They believed they were successful in distinguishing signals arising from detrusor contraction to those signals created by abdominal movements. Figure 1, shown below, shows some of their results. 4 Figure 1: Bipolar electrical signals of male during voiding (Doorn et al.). Permission to void occurs at mark A. Client Requirements The client has few, yet specific requirements for this device. Originally, his understanding was that no one had yet to attempt an EMG of the bladder during it’s contraction from a surface electrode. After a simple search for journal articles on the subject, it was clear that this field of study had been explored by numerous other professional level scientist and engineers. The client still wants us to attempt to construct a device that he will be able to use in his lab to obtain EMG data of the bladder throughout the voiding process. Ideally, the device should obtain the signal through surface electrodes. If this is not possible, he would accept more invasive means. He also wants the device to be used two to three times a day, and on various patients. He would like 5 to have the data our device obtains be digitalized and input into a computer software program where he could analyze it and make time comparisons to other data, such as internal bladder pressure and voiding flow rate. Problem Statement Our client seeks a noninvasive technique for the electromyography of the bladder. The device will be used in an urodynamics laboratory in conjunction with many other urinary diagnostic tools. Proposed Design Solutions I. Electrodes The bladder is located just beneath the pubic bone and rests against the pelvic floor and vagina in females. Several options are available for electrode placement, each presenting significant advantages and disadvantages. These locations are a) upon the skin above the pubic bone, b) within the vagina, or c) inside the bladder. Figure 2: Anatomy of Bladder. a) Two or more surface electrodes are taped directly above the pubic bone. This is the quickest and most convenient option available. It allows a fixed location for the 6 electrodes and can be placed with nominal accuracy. Little to no pain is discomfort is put upon the patient with this procedure. Because the skin barrier is not breached, there is minimal risk of infection if the electrodes are not properly sterilized. This technique will work well in the urodynamics laboratory as it will not interfere with catheters placed in the bladder via the urethra. Prior to the Netherlands study, it was unknown how viable this option would be due to signal strength concerns. Figure 3: Medtronic surfaces electrodes. Figure 4: Noraxon Ag-AgCl surface electrodes. b) A device to be inserted into the vagina would contain two electrodes separated by a fixed distance. This allows measurements to be recorded very close to the bladder wall, in the range of less than four millimeters. It is believed that the most accurate, isolated signal could be obtained in this fashion, though limited to use only in females. During contractions of the detrusor the electrode locations would remain constant, at least in respect to one another. While still relatively easy to insert and remove the device, this method may be uncomfortable or painful for some patients. It crosses a certain line of privacy, especially when other possibilities exist for electrode placement. Sterility of the device between uses is imperative. Because of the environment, electrode type may be limited as well. 7 Figure 4: Diagram of electrode inserted into vagina. c) Two thin electrodes are fed via a catheter through the urethra and into the bladder. A spring device might be used to create a fixed distance between the electrodes while inside the bladder. Another option is the use of a linear array of electrode sensors along a wire to be inserted in a similar fashion. This method allows very isolated signals to be recorded, as only the thin tissue of the bladder wall separates the electrodes from the detrusor muscle. Electrical “noise” from abdominal muscles and other tissues would be minimal. However, this method is invasive and the use of catheters can be painful for some patients. Infection is again a concern if the electrodes are not properly sterilized between uses. The spring-loaded device must be designed to be failsafe, so that it collapses properly for electrode removal. Figure 5: Electrode inserted through urethra. Electrodes will be purchased from a medical supplier. For surface electrodes, standard AgAgCl disk electrodes will be used. These can be purchased from a variety of suppliers. 8 Noraxon USA, Inc. has disposable, self adhesive Ag-AgCl single electrodes with a diameter of 10 mm. Linton Instrumentation offers reusable and disposable Ag-AgCl electrodes with 4mm, 8mm, or 12mm diameters. Medtronic, Inc. has a variety of electrodes for use in the vagina and urethra. Pricing has not yet been done on any of the electrodes. Figure 6: Variety of Medtronic electromyography electrodes. II. Circuitry One of the more crucial aspects of this device is the EMG circuit. The purpose of the circuit is to take the electrical signal that the electrodes have detected and modify it in such a way as to make it more meaningful to our client. Numerous things need to be taken into account such as degree of amplification, proper high pass and low pass corner frequencies, and potential sources of noise. Careful research was carried out to try and determine the magnitude of signal we can expect to be initially detecting using surface electrodes. However, the vast majority of experiments on bladder electrical activity were carried out using electrodes that were sewn directly onto the bladder surface. These studies reveal amplitudes in the range of 0.1 to 2 mV (Doorn et al.).The 9 one study known to date that has tried to measure bladder EMG from surface electrodes detected signals on the order of .5mV. The reliability of this study is questionable in general because it is the first study to seriously attempt the surface electrode method. However, we believe that the best assumption that can be made is that we can expect a .5mV signal. To amplify this signal to the point where it can be clearly seen on an oscilloscope would require an amplification of 2000. Again, this is only an early estimate and we believe that only through testing will we be able to better extrapolate a better idea of the correct amplification. Also of paramount importance to the EMG circuit is its high and low pass characteristics. As with the single amplitude, the frequency of the signal is not precisely known. The bladder is composed entirely of smooth muscle, which is known for having a very slow frequency. To accurately detect signals of the proper frequency, filters need to be applied to the circuit. The main purpose of the high pass filter is to remove any dc current in the system. The high pass corner frequency should be set low enough so that the slow frequency of the bladder contraction is not filtered out, but high enough to remove dc current. Ideally, applying a digital filter to the signal would have a perfectly sharp cut off frequency, but this may not be possible with the equipment we have available. We recommend a high pass cut off frequency of 0.01 Hz. The cut off frequency of the low pass filter is even more questionable. Once again, Doone’s study offers some direction. He was able to obtain a signal using a low pass digital filter with a cut off frequency of 66Hz. We would recommend 66Hz as a good starting place for our circuit. 10 There are a few possible sources of noise that should be anticipated. First of all, signals common to two different electrode leads should not be amplified. Sources of this include mainly the inductance between the leads and surrounding power sources. An EMG circuit with a good common mode rejection ratio is desired. A ratio on the order of 90 dB should prove sufficient, as it worked well in Doone’s study. Other sources of noise, such as small voltages produced at the skin/electrode junction will have to be taken into account. Through the use of proper cut off frequencies and amplification, most of which can only be determined through extensive testing, will we hope to obtain an EMG signal solely from the contraction of the bladder. III. Data Storage Many of the possibilities for data conversion and storage still need further research and consideration. In general, converting the analog data to a digital format has numerous benefits. First of all, digital filtering is “highly immune to interference because of the way it is implemented.”(Cao). This means that digital signals are much less likely to contain noise if the digital filter is accurately applied to the data from the signal. Another reason is that the degree of accuracy of the digital signal as a representative of the analog signal can be adjusted by varying the sampling rate and bit number. Perhaps the biggest reason to convert to a digital signal is that a digital signal can be processed, stored, and displayed in a variety of different ways after the analogue signal has been obtained. All of this is done through the use of computers. Additional research needs to be done to determine in what format the client would like to display his data, and what data processing devices he currently has in his lab. 11 For at least the initial stages of the testing of our prototype, we believe an oscilloscope could function as a method of viewing the results from the EMG circuit. Although there is no method of long term data storage available by using an oscilloscope, it should provide us a chance to see the signal in real time, as the bladder contracts. Final Design Adhering to the desired design concept, surface electrodes were chosen to measure electrical activity of the bladder. Initially, concerns were raised as to whether a viable signal could be obtained from this location, a distance away from the detrusor muscle. Namely, the pubic bone might block the weak electrical signals from being recorded. However, as shown by the team in the Netherlands, signals could be recorded through the tissue. Thus, worries about accuracy and signal strength with this method were negated. Regarding these facts, the use of surface electrodes is by all means the best option available. Standard Ag-AgCl disk electrodes will be used. To summarize the final circuitry design, an EMG circuit complete with buffers, a differential amplifier, and both a high and low pass filter should be built. Ideally, an amplification of 2000 should be obtained. The band pass of the filters should cover the range from 0.01 to 66Hz. Initially, testing could begin with the use of two electrodes hooked up to one EMG amplifying circuit. Possibilities exist for further development of using more electrodes. The figure below shows the basic design of our device. Figure 7: Final Design 12 Data collection methods and storage options still need further examination. Until we gain more information from the client and learn what kind of equipment he has available, we will simply use an oscilloscope to plot the change in voltage across the electrodes throughout the time it takes to void the subject’s bladder. Conclusion Following our design solution and circuitry outline, a prototype EMG circuit will be built. After completion, extensive testing will be done to evaluate its performance. This will occur in Dr. Bushman’s urodynamics laboratory. Specifically, research must be done to determine the optimal orientation and number of electrodes that yield the strongest, most isolated electromyography of the bladder. The exact frequency and amplitude of the electrical signals from the detrusor muscle will be determined throughout this process. This will involve analyzing other electrical activity present during voiding, including effects of such actions as coughing, sneezing, and use of the abdominal muscles. After reviewing data from this research, a redesign of the circuit component may be necessary. The final circuit design will undergo further testing to examine its usefulness in the laboratory. 13 References Doorn, E.S.C. van Waalwijk van, Gommer, E.D., Janknegt, R.A., and Kinder, M.V. “A NonInvasive Method for Bladder Electromyography in Humans.” Archives of Physiology and Biochemistry. Vol. 106, No. 1, pp. 2-11, 1998. “Electrodes.” Linton Instrumentation. http://www.lintoninst.co.uk/electrodesinvivo.htm (28 September 2003). “Overactive Bladder.” American Foundation for Urologic Disease. http://www.afud.org/oab/media/presskit/back3.html (26 September 2003). “Overactive Bladder: Symptoms, Causes and Treatments.” NCERx. http://www.bladderdisorders.com/html/overactive-bladder.php3 (26 September 2003). “Surface EMG Electrodes.” Noraxon USA, Inc. http://www.noraxon.com/Products/electrodes.htm (28 September 2003). Urodynamics Accessories Catalog. Medtronic, Inc. http://www.medtronic.com/neuro/mfd/urology/URO_acc_2001.pdf (27 September 2003). 14 Appendix Product Design Specifications Function: The Bladder Contraction Detector (BCD) would provide a means of sensing the contraction of the bladder in a non-invasive manner. Ideally, the BCD detects and records the electrical activity of the bladder detrusor muscle throughout the voiding process. Client Requirements: Data collected is saved to a computer or available as a printout Data collection is performed by electrodes External electrode placement is preferred Device applicable to both sexes preferred Design Requirements: 1. Physical and Operational Characteristics a. Performance requirements: The device is to be used two to three times a day in a laboratory setting. b. Safety: The device should meet the highest standards of safety. Before human testing, a protocol concerning its use and safety would have to be approved. c. Accuracy and Reliability: A high degree of precision would be ideal. Measurability is not a concerning factor. d. Life in Service: The device should be reliable as it will be used 2-3 times a day over the course of 2 years. e. Operating Environment: Surface electrodes – 20-25°C Electrodes within bladder – pH 5-8, 37°C, high concentration of salts and ammonia, maximum pressure 150cm water Electrodes within vagina – pH 4-5, 30-37°C, moist h. Size: The device will be used in a confined laboratory setting, so its size must be reasonable. i. Weight: There are no weight limitations as the device will be used in a laboratory setting. Ideally, it will be less than 20 lbs. j. Materials: No material restrictions exist for the main circuit component. If internal electrodes are used, they must be biologically inert. Materials toxic to the human body cannot be used. 15 2. Production Characteristics a. Quantity: One b. Target Product Cost: $200 or less 3. Miscellaneous a. Standards and Specifications: FDA approval may be required for clinical use. c. Patient-related concerns: The device will need to be sterilized for each subject. Patient data from the device must be kept confidential as according to hospital standards. d. Competition: Similar devices have been constructed for research purposes. 16