synapses fluorine
advertisement

Coffee, Smoking and Female Gender; New insights
in protection against Parkinson’s disease?
A closer look at Parkinson and neuroprotective
factors
A literature-based study by:
K. Fornasari, 0473022
Supervisor:
H. Heusinkveld & R. Westerink
Department:
Neurotoxicology Research Group, Institute for Risk Assessment Sciences
(IRAS)
Abstract
Parkinson’s disease (PD) is an age-related progressive disease with symptoms like tremor
and bradykinesia. The major pathological hallmark of PD is degradation of dopaminergic
(DA) neurons but the mechanism is still not clear. It is believed that inter-related processes
like oxidative stress, excitotoxicity, depletion of endogenous antioxidants, reduced
expression of trophic factors and dysfunction of protein degradation are involved in the
cascade of events that will lead to DA neuron death. Age-standardized incidence rates of PD
in population-based studies in European countries and the USA range from 8.6 to 19.0 per
100,000 inhabitants when strict diagnostic criteria of PD are applied. When looking at PD
incidence rates in different gender, men are more susceptible for PD than women. It is
thought that in developing countries PD is less common than in developed countries because
of medical care, and shorter average lifespan. But because there are no good records of PD
patients in e.g., the African continent, it is difficult to estimate incidence rates of PD and to
compare these with incidence rates in developed countries. Until now there is still no cure for
PD, the available medication and surgery can only provide relief from symptoms. Although
there is no cure for PD, scientists found some striking evidence that nicotine, caffeine and
estrogens have neuroprotective effects on PD. This thesis went deeper into the subject of
neuroprotective factors in PD, how and why these protective factors work (what are their
mechanisms) what is already known and how these factors can (possibly) contribute to
therapies and the protection against PD. The neuroprotective factors are discussed in
particular, are nicotine, caffeine and estrogens and their restriction to gender. From this
literature based study it can be concluded that the specific neuroprotective factors are
gender related and that they can provide new potential strategies for the protection against
PD. The mechanisms, targets and genetic influences of these neuroprotective agents
deserve further investigation.
2
Preface
With this thesis I hope to broaden my knowledge about the scientific field of
neurotoxicology and to learn more about the scientific progresses within this field.
The general subject of this thesis is Parkinson's disease. The reason why I am
interested in this disease is that I came in touch with this disease at a very young
age. My best friends’ mother was diagnosed with PD when I was just about eight
years old and heard that there was/is nothing medical science could do about the
disease. My friends’ mother would not live very long. I thought it was not fair to just
wait until her symptoms went so bad that she eventually could not move anymore or
even die at a very young age. Now I'm almost 25 years old and I'm still seeing my
friends’ mothers once in a while because she's living about two blocks away from me.
I admire her because she is still pretty mobile and even passing me by on her
bicycle. Because of her strength and will to live I want to dedicate this thesis to her
and all PD patients. I hope that this thesis will give people an insight in the
possibilities of research on PD and maybe even a way of fighting this disease.
I would like to thank Mrs. Verduin to give me the inspiration to write this thesis and of
course my supervisors.
I hope you to get more interested in PD after reading this thesis,
Kim Fornasari, January 2010.
3
Outline
Introduction: Parkinsonism and Parkinson Disease pp. 5/7
Physical and Physiological Symptoms of PD
DA Neuron Degeneration
Treatment
Chapter I: Prevalence and Incidence of PD pp. 8/11
I.I General Prevalence and Incidence
I.II Incidence/ Prevalence in Developed Countries (Europe)
o
I.II.I Incidence in the Netherlands & U.S.A.
I.IV Incidence/ Prevalence in Developing Countries
o
I.IV.I A Door-to-Door Study
o
I.IV.II PD Management in Africa
I.V Conclusion
Chapter II: Risk factors in PD pp. 12/15
II.I The Inheritance of PD
II.II Environmental Risk Factors
II.III Environmental Risk Factors During Early Life
o
II.III.I Infections in Early Life
o
II.III.II Place of Birth
o
II.III.III Toxic Exposure Early in Life
II.IV Conclusion
Chapter III: Neuronal cell death pp. 16/22
III.I Mechanisms of cell death in the SN
III.II Mechanisms involved in neuronal cell death
o
III.II.I Oxidative stress and mitochondrial dysfunction
o
III.II.II Protein aggregation and misfolding
o
III.II.III Neuroinflammation
o
III.II.IV Excitotoxicity
o
III.II.V Apoptosis
o
III.II.VI Loss of neurotrophic factors
Chapter IV: Neuroprotective factors pp. 22/24
IV.I Adenosine receptor antagonists
IV.II Anti-inflammatory agents
IV.III Alpha-synuclein-directed therapies
IV.IV Kinase inhibitors
IV.V Trophic factors
IV.VI Antioxidants
Chapter V: Three important neuroprotective factors pp. 25/32
V.I Nicotine
o
V.I.I Nicotine neuroprotective but not neurorestorative
o
V.I.II The Mechanism
o
V.I.III Nicotine as antioxidant
o
V.I.IV The influence of nicotine on the gene expression in PD
V.II Caffeine
o
V.II.I Caffeine reduced PD and the role of estrogen
o
V.I.II The Mechanism
V.III Estrogen and PD
o
V.III.I Estrogens and the Nigrostriatal System
o
V.III.II Neuroprotective Effects of Estrogen in PD Animal Models
Chapter VI: Discussion and Future Research Leads pp. 33/37
VI.I Conclusion/Discussion
VI.II Future Leads
VI.III New Research Plan (??)
References pp. 38/15
Appendix pp. 2/4
4
Introduction: Parkinsonism and Parkinson’s disease
Parkinsonism is a term that refers to a clinical syndrome that includes many
combinations of motor problems, ebradykinesia (slowness and decreased amplitude
of movement), tremor-at-rest, muscle rigidity, loss of postural reflexes, flexed
posture, and the freezing phenomenon). For the diagnosis of Parkinsonism not all
the six features have to be present. At least two of the features need to be present,
with at least one of them being tremor-at-rest or bradykinesia.
The major cause of parkinsonism is Parkinson’s disease (PD) and can be referred to
as the primary parkinsonism. There are also three other types of parkinsonism [1]
namely; 1) secondary parkinsonism, such as drug-induced parkinsonism and postencephalitic Parkinsonism, 2) Parkinson-plus syndromes (presence of parkinsonism
plus other neurological features), such as the diseases known as progressive
supranuclear palsy and multiple system atrophy, and 3) heterodegenerative disorders
in which parkinsonism is only one feature of a hereditary degenerative disorder, such
as juvenile Huntington disease and Wilson disease.
To make a good diagnosis of PD there are three helpful clues that could indicate that
patients are dealing with PD rather than another category of parkinsonism[[2]; 1) an
asymmetrical onset of symptoms (PD often begins on one side of the body), 2) the
presence of rest tremor (rest tremor may be absent in patients with PD, it is almost
always absent in Parkinson-plus syndromes), and 3) substantial clinical response to
adequate levodopa therapy (usually, Parkinson-plus syndromes do not respond to
levodopa therapy). In this thesis I will focus specifically on the classical PD.
Physical and Physiological symptoms of PD
PD is a slowly progressive parkinsonian syndrome that gradually worsens in severity,
and, as described above, usually affects one side of the body before spreading to
involve the other side. Although the illness sometimes begins with bradykinesia, and
in some patients, tremor may never develop, tremor-at-rest is often the first symptom
recognized by the patient. Over time there is a steady worsening of the symptoms. If
these symptoms are left untreated, this will lead to disability with severe immobility
and falling. The early symptoms and signs of PD — rest tremor, bradykinesia, and
rigidity — can be corrected by treatment with levodopa and dopamine (DA) agonists.
When PD progresses over time, symptoms that not respond to levodopa will develop
steadily, such as flexed posture, the freezing phenomenon, and loss of postural
reflexes; these are often referred to as non-DA-related features of PD.
Moreover, bradykinesia that responded to levodopa in the early stage of PD
aggravates as the disease worsens and becomes no longer fully responsive to the
levodopa treatment. These intractable motoric symptoms lead specific to disability
with increasing immobility and balance difficulties. Although the motor symptoms of
PD dominate the clinical picture, and even define the parkinsonian syndrome, many
patients with PD have other complaints that have been classified as non-motor.
These include fatigue, depression, anxiety, sleeping disturbance, constipation,
bladder and other autonomic disturbances (sexual, gastrointestinal), sensory
complaints, decreased motivation and apathy, slowness in thinking (bradyphrenia),
and a declining cognition that eventually can progress to dementia. PD and the
Parkinson-plus syndromes have a degeneration of substantia nigra (SN) pars
compacta dopaminergic neurons in common, with a resulting deficiency of striatal DA
concentration due to loss of the nigrostriatal neurons. This neuronal loss comes
accompanied by an increase in glial cells in the SN and a loss of neuromelanin (NM),
5
the pigment that is normally contained in SN dopaminergic neurons. In the surviving
neurons, Lewy bodies are usually present. These bodies are intracytoplasmic,
eosinophylic, inclusions. The progressive loss of the nigrostriatal dopaminergic
neurons corresponds to a decrease of DA content in both the SN and the striatum.
Progressive loss of the dopaminergic nigrostriatal pathway can be detected during
life using PET and SPECT scans. These scans show a continuing reduction of floroDOPA (FDOPA) and DA transporter ligand binding in the striatum and an altered
secondary effect on cortical metabolism. [3-7]
DA neuron degeneration
The exact mechanism that is responsible for DA neuron degeneration in PD is still
not known. Oxidative stress, excitotoxicity, depletion of endogenous antioxidants,
reduced expression of trophic factors and dysfunction of protein degradation are
believed to be involved in the cascade of events that will lead to DA neuron death [810]. Looking at several studies, there is a clear indication that neuro-inflammatory
mechanisms possibly play an important role in the pathogenesis of PD, therefore,
inhibition of inflammation is proposed here as a very promising therapeutic
intervention [11-15]. Most cases of PD appear to be sporadic and represent interplay
between both genetic and environmental influences [16]. Genetic factors may interact
with early life events such as the exposure to hormones, endotoxins and neurotoxins
and thereby influencing the severity and predisposition of the disease.
Developmental exposure to environmental toxins (such as pesticides/herbicides),
either alone and/or in co-operation with other environmental (i.e. endotoxins;
hormonal dysfunctions) and/or genetic “predisposing” factors, may synergistically
increase DA neuron vulnerability [16-17], these environmental factors will be
discussed further in Chapter II
Treatment
Until now, there is no cure for PD but medication or surgery can provide a relief from
the symptoms. The most widely used form of treatment is L-dopa in various forms. Ldopa is transformed into dopamine in the dopaminergic neurons by L-aromatic amino
acid decarboxylase. However, only 1-5% of L-DOPA enters the dopaminergic
neurons and the remaining L-DOPA is often metabolized to dopamine elsewhere,
causing a variety of side effects. Due to the feedback inhibition L-dopa results in a
reduction in the endogenous formation of L-dopa, and eventually become
counterproductive. Carbidopa and benserazide are dopa decarboxylase inhibitors.
They help to prevent the metabolism of L-dopa before it reaches the dopaminergic
neurons and are generally given as a combination of carbidopa and levodopa, called
co-careldopa, and benserazide and levodopa, called co-beneldopa [18-20]. Duodopa
is an example combination of levodopa and carbidopa, dispersed as a viscous gel.
Using a patient-operated portable pump, the drug is continuously delivered via a tube
directly into the upper small intestine, there it is rapidly absorbed. Another drug,
Stalevo (a mix of carbidopa, levodopa and entacapone) is also available for
treatment. Tolcapone is a drug that inhibits the Catechol O-methyl transferase
(COMT) enzyme, thereby prolonging the effects of L-dopa, and so has been used to
complement L-dopa. Due to its possible side effects such as liver failure, it is limited
in its availability. A similar drug, entacapone has not been shown to cause significant
alterations of liver function and maintains adequate inhibition of COMT over time. [18,
34].
6
Another treatment is based on dopamine agonists; the dopamine agonists
bromocriptine, pergolide, pramipexole, ropinirole, piribedil, cabergoline, apomorphine,
and lisuride are moderately effective. Each of these antagonists has its own side
effects like somnolence, hallucinations and/or insomnia [19-20]. Dopamine agonists
initially act by stimulating some of the dopamine receptors [21]. However, they cause
the dopamine receptors to become progressively less sensitive and will eventually
increase the symptoms [19-20]. Dopamine agonists can be useful for patients
experiencing on-off fluctuations and dyskinesias as a result of high doses of L-dopa.
Apomorphine can be administered via subcutaneous injection using a small pump
which is carried by the patient. A low dose is automatically administered throughout
the day and reducing the fluctuations of motor symptoms by providing a steady dose
of dopaminergic stimulation [22-25]. Other drugs like selegiline and rasagiline inhibit
monoamine oxidase-B (MAO-B) and reduce the symptoms. MAO-B breaks down
dopamine secreted by the dopaminergic neurons will result in inhibition of the
breakdown of dopamine. Metabolites of selegiline include L-amphetamine and Lmethamphetamine [26]. The use of this drug might result in side effects such as
insomnia. Use of L-dopa in conjunction with selegiline has increased mortality rates
that have not been effectively explained [27]. Treating Parkinson's disease with
surgery was once a common practice, but after the discovery of levodopa, surgery
was restricted to only a few cases. Studies in the past few decades have led to great
improvements in surgical techniques and surgery is currently being used in people
with advanced PD for whom drug therapy is no longer sufficient [28]. Deep brain
stimulation is presently the most used surgical way of treatment, but other surgical
therapies that have shown promising results include surgical lesion of the
subthalamic nucleus and the internal segment of the globus pallidus, a procedure
known as pallidotomy [29]. Regular physical exercise and/or therapy can be
beneficial to the patient for maintaining and improving mobility, flexibility, strength,
gait speed, and quality of life; and speech therapy may improve voice and speech
function [30-32]. One of the most widely practiced treatments for the speech
disorders associated with Parkinson's disease is the Lee Silverman Voice Treatment
(LSVT). LSVT focuses on increasing vocal loudness [33].
The most striking finding in PD studies however, is the possible neuroprotective role
of nicotine, caffeine and estrogens as possible neuroprotective agents against PD.
There is not much known yet about the mechanism of these possible neuroprotective
agents. Nevertheless, these neuroprotective agents can lead to a new generation of
therapies against PD. This thesis will dig deeper into the subject of neuroprotective
factors in PD, how and why these protective factors work (what are their
mechanisms) what is already known and how these factors (possibly) can contribute
to therapies and the protection against PD. The neuroprotective factors that will be
discussed in particular are nicotine, caffeine and estrogens and their restriction to
gender. This thesis will deliver a contribution to a possible follow-up research on
Parkinson’s disease and its neuroprotective factors.
7
Chapter I: Prevalence and incidence of PD
Parkinson’s disease (PD) is a neurodegenerative disease with a prevalence of 100–
200 cases per 100,000 persons in the general population [35]. The prevalence
increases sharply with age, and most surveys show a slight male preponderance.
Moreover, prevalence rates may vary depending on the geographical location and
seem to be especially low in developing countries. Although there are many studies
assessing prevalence, incidence studies are scarce especially in developing
countries where PD patients are not recorded well and knowledge is scarce. If
incidence rates are known it is maybe possible to make a connection with the place
people live, the place of birth, exposure to risk factors and the enlarged risk of PD.
Based on several prevalence and incidence studies Alves and co-workers [36] made
a general estimation of the incidence and prevalence rates within different age
groups and different parts of the world.
I.I General Prevalence & Incidence
Parkinsonian characteristics may be subtle at the onset of the disease, misdiagnosis
is therefore not uncommon. In a community-based study, only 53 % of patients on
anti-Parkinson medication, initiated by general practitioners due to suspected PD,
fulfilled criteria of probable PD when investigated by neurologists [37]. Besides
Parkinsonian features also often occur in
Table I: Incidence of PD in Dutch men
patients with Alzheimer’s disease (AD) and
and women based on data from RNH
other dementia disorders. Methodological
[41-43].
differences between studies make direct
comparison of prevalence and incidence
estimates difficult. The disease is found in
all ethnic groups, but with geographical
differences in prevalence. Early onset of
sporadic PD is rare, with about 4 % of
patients developing clinical signs of the
disease before an age of 50 [38] and
approximately 1–2 % of the population over
65 suffering from PD. This figure increases
to 3 to 5 % in people of 85 year and older
[39]. As PD is mainly an illness of the
elderly, it is expected to be more common
in developed countries where people live
longer. Most community-based prevalence
studies across Europe found crude
prevalence rates between 100 and 200 per
100,000 inhabitants [35]. Incidence calculations are thought to be a more precise
estimate of the frequency of the disease because they are not influenced by
mortality. However, there are substantial variations in reported incidence rates, most
likely due to methodological differences between studies, in particular differences in
case ascertainment and use of diagnostic criteria. Age-standardized incidence rates
of PD in population-based studies in European countries and the USA range from 8.6
to 19.0 cases per 100,000 inhabitants per year when strict diagnostic criteria of PD
are applied. As may be anticipated, door-to-door surveys and studies using broader
inclusion criteria have yielded higher prevalence and incidence rate figures [40].
8
I.II Incidence/Prevalence in Developed Countries
In an incidence study of Leentjens and co-workers [41], the authors reported on the
incidence rates of PD in The Netherlands, based on the analysis of data from an
ongoing longitudinal general practice-based registration network. Their analysis was
performed with data from the Registration Network Family Practices (Registratie Net
Huisartspraktijken; RNH). Data was collected on all relevant current and past health
problems. Before the authors could analyse the data, ‘health problems’ must be
defined as ‘anything that has required, does, or may require health care management
and has affected or could significantly affect a person’s physical or emotional wellbeing’. These problems are coded according to the International Classification of
Primary Care (ICPC), using the criteria of the International Classification of Health
Problems in Primary Care (ICHPPC-2) [42-43]. The register was continuously
updated with information from all possible sources, including correspondence, reports
and investigations from hospital-based specialists. After defining data, the age- and
sex- specific incidences were calculated by using incident PD cases as the
numerator and the total number of RNH participants as denominator. From 1990 to
2000 (inclusive), 139 new PD cases were identified and the overall crude incidence
for the population was 22.4 per 100,000 inhabitants per year [95% confidence
interval (CI): 13.1–31.7]. Analysis of the results showed an exponential increase of
PD incidence with age which kept increasing on to the highest age groups. The
incidence in men in this study was higher than that in women in all age groups,
except in the 60- to 69-year- old. The results are shown in Table I. The authors
concluded that the annual incidence of 22.4 per 100,000 per year in our population is
comparable with that of two other recent European community studies, but higher
than reported in most studies. The questions you can ask yourself after seeing these
results are whether this incidence rate is a good reflection of the incidence of PD in
the Netherlands and other developed countries, and whether the study population is
representative. Another question could be whether the men and women gender really
differ that much in PD incidence and whether this is the same for other countries
or/and different ethnicities. According to the authors their study was accurate enough,
but in an incidence study a lot of things can go wrong like incompleteness and non
reliability of the registrations, differences in detection strategies etc.
In an USA study of Eeden and co-workers [44], another PD epidemiological study
amongst different ethnicity groups was performed. In this study there were some
differences in PD incidence amongst difference races/ethnicity, but it is not justifiable
to take the conclusion that one race is more susceptible for PD than other races or to
take any other conclusions about these results. This is due to the relatively low
number of cases amongst the non-white study population (see appendix 1).
Surprisingly, unlike the study of Leentjens and co-workers, the overall incidence of
PD amongst men was higher than in women (see appendix 1). The differences in
the overall incidence between these two studies can be explained by differences in
strategy, registration and accuracy. Besides, the comparisons of age- and genderadjusted incidence rates between individual groups were none of all statistically
significant. Before one could say something about differences in PD incidence rates
in different ethnicity/ race groups, more studies need to be done on this topic.
9
I.IV Incidence/prevalence PD Developing countries
It is suggested that less people suffer from PD in African populations [45]. In Africa,
crude prevalence rates range from 7 to 43 per 100,000 [46-47] while in developed
countries like the Netherlands the crude prevalence rate is about 200 per 100,000.
Whether there is a true difference in susceptibility of the African population would be
of great epidemiological importance, in terms of investigating the cause(s) of PD.
However, these differences in prevalence rates could be due to several factors:
under-diagnosis of PD in these communities, differences in case finding methods,
differences in diagnostic criteria used and early mortality owing to other causes in
these populations. Previous studies in sub-Saharan Africa (SSA) have been
performed using different methods, making them difficult to compare with each other
and other studies elsewhere in the world: door-to-door studies carried out by
Osuntokun et al. [48] (Nigeria); case finding from neurological clinics and neurological
admissions by Harries et al. [49] (Kenya) and Bower et al. [50] (Ethiopia);
retrospective review of hospital admissions by Lombard and Gelfand [45]
(Zimbabwe); and data on the use of levodopa (L-dopa) usage by Cosnett et al. [51]
(South Africa). As there are few studies, papers describing both idiopathic PD and
Parkinsonism are included.
I.IV.I Door- to- Door Study
In 1986 a door-to-door study was performed by Osuntokun et al. [48] in a
Nigerian town. The authors looked at all neurological disorders, not specifically PD.
They used a two-step procedure, with a screening questionnaire that was carried out
by non-medically trained administrators, followed by an expert history and
examination if they answered positively to the questionnaire. Nearly 95% of the
population took part in the study. Only 11% of the population were over 50 years
(compared with over 33% in the United Kingdom). No diagnostic criteria for PD are
described. Their results showed a point prevalence rate for PD of 10 per 100,000,
only two cases were identified. The sex and gender of the cases were unknown. A
second door-to-door survey was carried out by Tekle- Haimanot in rural Ethiopia
between 1986 and 1988. Again, this study, which included a population of 60,820,
looked at all neurological disorders, and not just PD. Participation rates were
between 95 and 100%. The median age of this population was 14.5 years with 59%
of the population being <20 years old. They found four cases of PD (all male), giving
a crude prevalence rate of 7 per 100,000. No diagnostic criteria for PD were
documented. The authors state that the reason for the difference in the prevalence of
PD among white populations is due to the difference in population age structure.
However the data was not standardised for age. [48] This study makes it clear that
accuracy is required to perform a reliable epidemiological study.
I.IV.II PD management in Africa
Until now there are probably many people in SSA with undiagnosed or untreated PD.
Even if the patient is diagnosed, treatment is too expensive and to scarce. Besides,
most staff in African medical departments will have little, if any, prior knowledge of
PD. The perception of the disease within the population is very different from that
seen in developed countries. The symptoms are not recognisable to the general
population as being a particular illness; often, people think it is part of the inevitable
consequences of ageing, or in some areas local beliefs lead people to believe that
they have been ‘bewitched’. As a result, seeking the help of the local traditional
healer is most likely to be the first port of call, and not western medical treatment. It
10
also leads to stigma for those affected, and can have a devastating social impact.
[52]
Conclusion
As PD is mainly an illness of the elderly, it is expected to be more common in
developed countries where people live longer.
Most community-based prevalence studies across Europe found crude
prevalence rates between 100 and 200 per 100,000 inhabitants.
Age-standardized incidence rates of PD in population-based studies in
European countries and the USA range from 8.6 to 19.0 per 100,000
inhabitants when strict diagnostic criteria of PD are applied.
In the study of Leentjens et al. [41] The overall crude incidence for the
population was 22.4 per 100,000 per year
In the study of Leentjens et al. [41] as well as in the study of van den Eeden et
al. [44] the incidence rate of PD for man was higher as in women.
On the African continent it is still unclear how many people suffer from PD so there is
still no clear incidence or prevalence rate reported. Parkinson’s disease is present in
SSA and even those who are diagnosed and can afford treatment still have a difficult
clinical course:
Medical treatment is difficult to find, rarely available or affordable.
No major improvements have been made in the past 20 years.
Most people with PD remain undiagnosed and untreated in the community.
Patient education and information are severely lacking
Generally, no written information or long-term follow-up is available.
Only flying services are available for patients with PD in the developing world
in comparison with those available and taken for granted in the developed
world [52].
This will probably be the same for other developing countries/continents. Therefore
the incidence rates between developed countries and developing countries cannot be
compared. Due to the use of different case finding and analytical methods incidence
rates within certain continents or countries cannot be compared either. Therefore,
more and reliable clinical databases are needed. If there is enough information about
incidence rates of PD amongst different continents and races/ethnicity, then there will
be more to say about the relationship between the different environmental factors like
place of birth, environmental exposures etc. In the next chapter possible risk factors
for PD will be presented, not only the environmental but also the genetic risk factors
will be discussed.
11
Chapter II: Risk factors in PD
II.I The inheritance of PD
The most cases of primary Parkinsonism are sporadic, but in 10% of cases a positive
family history is seen. A genetic base for PD had long been controversial. Twin
studies have indicated a greater role of genetic factors in younger onset patients than
in patients with onset over the age of 50s [53].
In the last few years several gene mutations have been discovered, by painstaking
linkage and genome analysis, to cause PD in a small number of families. Ten
monogenic forms of PD, labelled PARK 1-10, have been identified with genes
identified in five. They are present either as autosomal dominants or autosomal
recessive mutations. Identification of these mutations has led to the recognition that
the ubiquitin–proteasome system is an important pathway that may be disrupted in
PD [54-55]. Studies are ongoing to identify additional genes that may contribute to
PD susceptibility, particularly in late-onset families without a clear pattern of disease
inheritance. More investigation about the inheritance of PD is required. Other genes
that probably are candidates in PD are genes that are involved in determining
dopamine signalling and disposition. Polymorphisms in the genes encoding
monoamine oxidase-B (MAO-B) and monoamine oxidase A (MAO-A) have been
explored as potential risk factors for PD (see Chapter IV).
II.II Environmental Factors
The event that suggested that environmental factors might contribute to the etiology
of PD was the recognition of a clearly induced state of acute parkinsonism by
accidental poisoning from MPTP (1- methyl-4-phenyl-1, 2,5,6-tetrahydropyridine), an
impurity that was a by-product in batches of illicitly produced “synthetic heroin” MPPP
(1-methyl-4-phenyl-4-propionoxypiperidine; also known as PPMP in Davis et al. [56]).
Although the absence of an additional methyl group on the 4-phenyl-piperidine ring,
MPPP is identical to the narcotic alphaprodine (1,3-dimethyl-4-phenyl-4propionoxypiperidine; also known as Nisentil), which is 26-fold more potent in rats
than its better-known isomer, Demerol (meperidine; pethidine; 1-methyl-4-phenyl-4piperidinecarboxylic acid ethyl ester). In addition to MPTP toxicity, there are also
several reports suggesting roles of other compounds in the induction of
parkinsonism; the best documented is manganese [57-59]. Manganese toxicity also
produces dystonia and was observed in manganese miners and ore-crushing
workers. But the toxicity from MPTP is much more specific than that from manganese
by affecting selectively the DA neurons. Namely, manganese affects other basal
ganglia neurons as well. Although these and other chemical poisons, like carbon
monoxide, can induce parkinsonism, this is classified as secondary- and not primaryparkinsonism or PD. In addition, rural living and pesticide and herbicide exposure at
early life have also been suggested from epidemiological studies to play a major role
in inducing PD [60]. A good example of a prospective study on the risk of pesticides
is the cohort study of Japanese men in Hawaii, originally established for the
investigation of risk factors: 7,986 Japanese–American men born between 1900 and
1919 were enrolled in the longitudinal Honolulu Heart Program, with a median length
of follow-up of 27 years. The relative risk of PD was 1.9 (95% CI, 1.0–3.5) for men
who had worked more than 20 years on a plantation compared with men who never
worked in a plantation (sugarcane and/or pineapple). The age-adjusted incidence of
12
PD was higher in men exposed to pesticides than in men who never did plantation
work [80].
II.III Environmental Risk Factors During Early Life
Neuropathological studies and animal models show that exposure to environmental
neurotoxicants can determine progressive damage in the substantia nigra many
years before the onset of clinical parkinsonism. Therefore, PD, like other neurologic
diseases related to aging, may be determined by exposures from the environment
early in life or even during pregnancy.
II.III.I Infections in Early Life
Inflammation has been proposed as one of the possible pathogenic mechanisms for
PD [61]. The pro- inflammatory cytokine tumour necrosis factor α (TNF- α) kills DA
neurons in vitro and is elevated in the brains of patients with PD [62]. Intrauterine
infection might lead to nigral cell loss in the fetal brain and a subsequent decrease in
DA neurons in the substantia nigra secondary to inflammation. Bacterial vaginosis
during pregnancy is characterized by the presence of lipopolysaccharide (LPS), a
bacteriotoxin that is an inducer of TNF-α [63]. These compounds are increased in the
chorioamniotic environment of infected women and could interfere with the normal
development of DA neurons in the fetus.
The results of Ling et al. [64] showed the possibility that, after intrauterine infection,
some newborn children had limited striatal neurochemical reserves and a reduced
DA cell count. This reduced reserve might enlarge the risk of developing PD in
adults. Most epidemiologic studies on infection during early life and risk for PD were
conducted in England. A population-based study was conducted in 42 general
practices in eastern Hertfordshire [65]. PD cases were subjects born after 1910 and
diagnosed by a neurologist or a geriatrician, and controls were subjects in the same
general practices matched by age and sex (172 cases, 343 controls). Records in the
first part of the 20th century were used to obtain information about birth weight and
growth during the first year of life. The subjects answered a questionnaire about
sibling ship, position in the birth order, type of housing, other features of the
environment in early life, and experience of the common infections of childhood.
Subjects were more likely to have suffered croup (odds ratio (OR) = 4.1; 95%
confidence interval (CI), 1.1–16.1) or diphtheria (OR = 2.3; 95% CI, 1.1–3.6) these
infection probably enlarged their risk of developing PD. The results of this study do
not suggest that poor growth in fetal life or infancy is important in the etiology of PD
but do suggest that early infection might have a role in susceptibility to PD. Some
investigators have examined the relationship between influenza pandemics and PD,
testing the hypothesis that PD could follow intrauterine influenza [66]. Three groups
of PD patients were identified through specialty clinics or general practitioners.
Matched controls were selected which were born in the same 5-year period as the
index patient. For each group and each calendar year, the parkinsonian ratio to
control births was calculated. This risk ratio was used to estimate the relative risk of
each cohort developing PD in later life. Subjects born in 1892, 1904, 1909, 1918,
1919, and 1929 (years encompassing the influenza pandemics of 1890–1930)
appeared to have an increased risk of developing idiopathic PD compared with
subjects born in other periods, and four of these years coincide with years of
influenza pandemic. The PD vs. control birth ratio showed a significant correlation
with the crude influenza mortality for the year of birth during the period from 1900 to
1930 [66]. People born around 1900 had a risk of PD 5 times that of people born
13
around 1930 [67]. The strong variation of PD risk from year to year of birth shown in
some of the previous studies would be consistent with the action during development
of an infectious agent, more likely a virus that typically occurs in epidemics. These
studies were all based on the hypothesis that intrauterine influenza infection or other
viral insults may be cytotoxic to the developing fetal substantia nigra and could
enhance the risk of PD after a latent period [68-69]. Data on the season of birth are
not very good arguments for a relationship between influenza and PD because there
are other potential factors that are characterized by a seasonal variation that could
be responsible for the observed association. Epidemiologic studies on the
relationship between infections early in life and PD are inconclusive and again more
research is required.
II.III.II Place of Birth
The place of birth can be used as a surrogate for early- life exposure. And so the
state of birth in the United States was studied as an exposure of interest for PD [70].
The outcome was measured by death, using the death certificates from U.S. death
information in 1981. The measure of effect was the proportionate mortality ratio
(PMR), using all the other deaths in the United States as the comparison group.
Potential confounders such as age, gender, and whether the state of birth was the
same as the state of death were included in a logistic model. Cerebrovascular
disease deaths were used as a negative control group because there is no
association with childhood exposure; multiple sclerosis was used as a positive control
because it has been found related to geography in childhood. The results showed a
very high PMR for Utah (45/10,000), Idaho (37/10,000), Colorado (31/10,000), New
Mexico (32/10,000), Kansas (32/10,000), and Nebraska (33/10,000), with a west to
east gradient. The lowest PMR was registered in Delaware (7/10,0000). However, it
is important to mention that PMR can be affected by the distribution of other causes
of death. The PMR rates from west to east can possibly be explained by the fact that
many pesticide (especially Dieldrin and Lindane) and herbicide manufacturing
facilities were settled in these area’s until 1999. Like mentioned earlier, pesticide and
herbicide exposure can have a PD inducing effect. In contrast, an study conducted
by Kurtzke and Goldberg (1988) [71] using death certificates showed that ageadjusted death rates of PD presented a north–south gradient, similar to that found for
multiple sclerosis. Only the state where the PD subject was resident at the time of
death was considered in the analysis. Geographic studies based on death certificates
may be affected by the underestimation of PD cases that can be inhomogeneous
across different geographic areas. Studies of geographic variation need to be
interpreted with caution because many factors beyond environmental exposure could
determine the geographic patter n of a disease. Chance, migration, differences in
procedures used to diagnose/classify cases, and access to medical care are other
possible alternative explanations [72].
II.III.III Toxic Exposure Early in Life
Clinical parkinsonism can be caused by a series of previous mentioned exogenous
factors such as viruses, poisoning with toxic substances such as MPTP and
manganese, and trauma. These clinical observations suggest that environmental risk
factors are important for the etiology of PD. Several environmental toxicants related
to the occupation in agriculture have been implicated as risk factors in PD.
14
The chemical structure of 1-methyl-4-phenylpyridinium (MPP+), the toxic metabolite
of MPTP, is very similar to the herbicide paraquat (PQ) [73]. Animal experiments
have clearly shown the selective action of PQ on the DA system. Systemic PQ given
to mice through repeated intraperitoneal injections induces selective damage of DA
neurons in the pars compacta of the substantia nigra [74]. The cell loss in this model
was dependent on dose and age. The presence of a different effect of the exposure
at different ages in this model showed a possible interaction of toxic environmental
exposures with normal aging [74]. Chronic, continuous, and systemic exposure to
rotenone, commonly used as an insecticide in gardening, selectively inhibits
mitochondrial complex I, causing selective degeneration of the nigrostriatal system
with accumulation of cytoplasmic inclusions containing ubiquitin and α-synuclein [75].
In mice, PQ exposure determines an up-regulation of α synuclein, accelerating the
formation of aggregates in the substantia nigra [76]. This confirms previous
observations in vitro that postulated a selective binding of PQ with partially folded αsynuclein [77]. Toxic exposures that occur early in the development could determine
long-term pathology in the central nervous system. A model exploring this hypothesis
should explore the possibility that early damage to the DA system could result in cell
loss or high vulnerability to a second environmental risk factor associated with PD
(two-hit model). A similar kind of model was hypothesized for combined exposure to
PQ and the fungicide maneb (MB) during development. The combined action could
permanently change the nigrostriatal DA system and enhance its vulnerability to
subsequent neurotoxicant challenges. Mice exposed to two neurotoxicants, PQ and
MB, and subsequently exposed again as adults presented with the most severe
damage. They showed a 70% reduction in motor activity, 2 weeks after the last toxic
dose [78]. Developmental exposure to PQ or MB alone produced minimal changes,
whereas a significant decrease in nigral cell counts was observed after adult
exposure. Striatal DA levels were reduced with 37% after only the developmental
exposure to PQ plus MB, but after a second exposure during adulthood, striatal DA
levels were reduced with 62%. This experiment suggests that the exposure during
development to the two toxicants produced a state of masked toxicity that was
revealed after adult re-exposure. So exposure to specific pesticides during the
prenatal period can produce a limited but selective amount of lesions in the
nigrostriatal system. These developmental lesions might determine an enhanced
susceptibility that, in combination with later exposure to other toxicants (e.g., PQ),
may be involved in the induction of PD during aging.
Several epidemiologic studies have showed the importance of pesticides, in
particular insecticides and fungicides. The problem with these studies is that they
were mainly case–control, with a limited number of cases and without biological
measurement of the exposure. Most of the studies were based on retrospective
collection of data with questionnaires [79].
II.V Conclusion
As a conclusion, several research data suggest that the use of pesticides or
surrogates of pesticide exposure increase the risk of PD. However, there are still too
few epidemiologic studies specifically addressing the issue of toxic exposure early in
life. While the search continues for environmental factors that can be associated with
PD, several studies have shown that cigarette smoking, coffee drinking and estrogen
levels are inversely associated with PD.
15
Chapter III: Neuronal cell death
As described in the introduction, the currently available therapies like levopoda
therapy for PD are symptomatic and become less effective over time due to
progression of the underlying disease process. Due to this progressive nature of PD
and the fact that neuronal degeneration in the SN is slow, therapeutic intervention of
PD is especially aimed at blocking or slowing down the degenerative process.
Neuroimaging and autopsy data indicate that there is a preclinical period of 4-5 years
before the PD symptoms appear. The rate of cell loss and dopaminergic function in
the striatum is most likely to be in the order of 10% per year in PD patients. Both PET
and SPECT imaging are able to detect a decline in striatal dopamine function before
clinical symptoms appear which may make it possible to begin neuroprotective
intervention during the preclinical phase [3-7]. The neurodegenerative process in PD
is likely to involve a cascade of inter-related events; oxidative stress, mitochondrial
dysfunction, excitotoxicity with excess formation of NO and O2 radicals, and
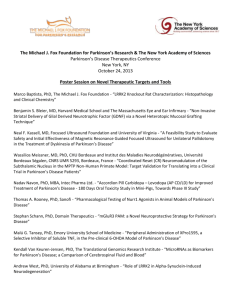
inflammatory changes, leading to both apoptotic and necrotic cell death (Figure 1) [810]. These events offer potential targets for neuroprotective therapeutic strategies
[11-15]. Because the dopaminergic neurons are dysfunctional for some time before
they are irreversibly damaged, both neurotrophic and anti-apoptotic agents may be
used to prevent delayed cell death and/or restore function [34].
Chapter IV will be dedicated to neuroprotective factors in PD, their mechanism, their
target(s), their restriction to gender and their possible contribution to new therapies.
In order to understand these factors, more knowledge about the mechanism of cell
death of DA neurons in the SN is required. In this chapter the normal mechanisms of
neuronal cell death will be discussed, followed by the events that are involved in the
progressive degeneration of these cells.
Figure 1: Oxidative stress, excitotoxicity, mitochondrial damage and altered calcium influx
each contribute to cell death and enhance each other. [34]
III.I Mechanisms of cell death in the SN
Even in the general population there is a gradual decline in neurons of the SN pars
compacta and dopamine content of the basal ganglia with age. In idiopathic PD the
symptoms appear when about 70 to 80% of the striatal dopamine [81] and about
50% of the nigral dopamine neurons are lost [82-83]. PD might progress in two ways.
There might be an accelerated rate of cell death so the critical level of dopamine loss
is reached during the normal life-span. Alternatively an acute insult or stress may
16
cause rapid but partial loss of substantia nigra neurons. This acute insult is inspired
by the earlier mentioned MPTP toxicity and the environmental toxin theory [84].
Post-mortem analyses have estimated the rate of cell loss in the substantia nigra
during normal ageing. This cell loss is about 5% per decade [82-83]. Nigral cell count
in PD is reduced by about 50% at the onset of the symptoms in comparison with agematched controls. As the disease progresses there is also a rapid progression of cell
death at a tenfold higher rate (45% per decade) [82-83]. Working backwards at the
same rate of cell loss, it has been estimated that PD patients would diverge from
control baseline about 5 years before the onset of symptoms. The rate of decline of
striatal dopamine function, as showed by serial PET or single-photon emission
computed homography (SPECT) scans is even higher (up to 12% per year), but
these studies have yielded similar estimates of approximately 4–5 years of disease
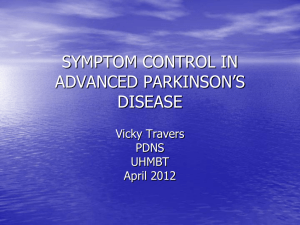
duration before the onset of the symptoms [3-7;85]. Looking at these data and figure
2, one could indicate that idiopathic PD may involve not a ‘double hit’ comprising an
acute toxic assault in combination with natural age-related cell loss, but that a more
active disease process in which nigral cell death is accelerated. In addition, the
disease is not a slow underlying decline that may have been going on for decades
before symptom appearance but rather begins in middle age, considerably later than
previously suspected, and becomes apparent relatively rapidly. The mechanisms
involved in the progressive degeneration of nigral dopamine neurons in PD are
studied intensively [86]. In recent years particular attention has focused on several
distinct mechanisms—oxidative stress, mitochondrial dysfunction, excitotoxicity,
calcium imbalance, inflammatory changes and apoptosis— which may all interact
and amplify each other in a vicious cycle of toxicity leading to neuronal dysfunction,
atrophy and finally cell death.
17
Figure 2: Rate of progression in Parkinson’s disease. Model of disease progression. Normal agedependent cell loss in the substantia nigra is shown in blue. PD symptoms become apparent after a
critical level of cell loss, the ‘symptom threshold’. In the ‘accelerated ageing’ model of PD (red), cell
loss starts early and progresses more rapidly, whereas in the ‘double hit’ or ‘assault’ model (brown)
there is subthreshold cell loss resulting from acute toxic insult, followed by a normal rate of agedependent cell loss until the critical threshold is reached. Recent evidence favours an even more rapid
exponential cell loss, departing from normal numbers only a few years before symptom onset (green)
[34].
III.II Mechanisms involved in neuronal cell death
III.II.I Oxidative stress and mitochondrial dysfunction
Oxidative stress is a result of overabundance of reactive free radicals secondary to
either an overproduction or a failure of cell buffering mechanisms that normally limit
their accumulation. Excess reactive species can react with cellular macromolecules
and thereby disrupt their normal functions. Oxidative damage to proteins, lipids, and
nucleic acids has been found in the SN of patients with PD [87-89]. Both
overproduction of reactive oxygen species (ROS) and failure of cellular protective
mechanisms appear to be operative in PD. Dopamine metabolism promotes oxidative
stress through the production of quinones, peroxides, and other ROS [90-91].
Mitochondrial dysfunction is another source for the production of ROS, which can
then further damage mitochondria. Complex I activity is diminished in the SN of PD
patients [92], while inhibitors of complex I, such as MPP+ and pesticides like
rotenone, can cause a Parkinsonian syndrome in animal models [93-95]. The
mechanisms responsible for mitochondrial dysfunction in PD are not well understood,
but inherited or acquired mutations in mitochondrial DNA may be one of the causes
[89-98]. Increased iron levels seen in the SN of PD patients also promote free radical
damage, particularly in the presence of neuromelanin. Other evidence is the
impairment of endogenous protective mechanisms in PD. The antioxidant protein
glutathione is reduced in post-mortem PD nigra [99-101]. Several of the genes linked
18
to familial forms of PD appear to be involved in the failure of protection against
oxidative stress, including PTEN-induced putative kinase (PINK1) and DJ-1 [102105]. There are different strategies that have been proposed to limit oxidative stress
in PD. These strategies include inhibitors of monoamine oxidase, a key enzyme
involved in dopamine catabolism; enhancers of mitochondrial electron transport, such
as Coenzyme Q10; compounds that can directly extinguish free radicals, such as
vitamin E; and molecules that can promote endogenous mechanisms to buffer free
radicals, such as selenium. The many kinds of agents have the advantage of being
tolerated with only a few adverse effects, but there is still no clinical proof of
effectiveness [106].
III.II.II Protein aggregation and misfolding
Protein aggregation and misfolding are important mechanisms in many
neurodegenerative disorders, including PD, Alzheimer's disease, and Huntington's
disease. While the proteins involved in these disorders are different, each is
associated with characteristic aggregates of misfolded protein, and these abnormal
aggregates appear to have some toxic properties. In PD, the primary aggregating
protein is alpha-synuclein (α-syn), whose link to PD was first identified through rare
families with autosomal dominant PD caused by mutations in this protein [107-110].
Although mutations in α-syn are found in a very small number of inherited PD cases,
α-syn is the major component of Lewy bodies and Lewy neurites found in sporadic
PD [111]. Gene duplication of the α- syn locus also causes PD, further supporting the
central role of this protein in PD pathogenesis [112]. Point mutations [113], over
expression [114], and oxidative damage of α-syn [115] all promote self-aggregation.
While some studies link α-syn to PD, the mechanism by which overabundance or
aggregation of α-syn cause neuronal injury is not understood yet. It is still unclear
which molecular form of α-syn is toxic. Hypotheses include toxic effects of oligomers
on cell membranes or proteosomal function, effects of α-syn on gene transcription or
regulation, interactions of α-syn with cell signalling and cell death cascades,
alterations in dopamine storage and release, and α-syn-mediated activation of
inflammatory mechanisms [116-119].
Recent studies implicating parkin and ubiquitin carboxyl-terminal hydrolase L1 (UCHL1) in genetic forms of PD reinforce the connection between protein aggregation and
PD pathogenesis [120-121]. Parkin is an E3 ubiquitin ligase involved in targeting
misfolded proteins for degradation, mutations of this gene found in genetic forms of
PD disrupt its E3 ubiquitin ligase activity. Surprisingly native α-syn does not appear to
be a substrate for parkin [122], and brains from patients with parkin-associated PD do
not usually contain Lewy bodies [123]. Parkin does appear to have a variety of other
substrates that may play a role in protein turnover and degradation, including HSP70,
which is known to modulate α-syn toxicity [124]. UCH-L1 serves as an ubiquitin
recycling enzyme in neurons, and its dysfunction promotes aggregation of damaged
proteins, including α-syn [125]. So overproduction or impaired clearance of α-syn,
resulting in aggregation, may be an important mechanism for PD. With this
information new potential neuroprotective therapies could be developed like inhibitors
of α-syn aggregation. Molecules that promote protein clearance could also have
therapeutic potential in genetic PD patients. Promoters of protein clearance could
include enhancers of parkin or UCH-L1 function, or molecules that promote
proteosomal or lysosomal degradation pathways [126]. So still, more research is
required.
19
III.II.III. Neuroinflammation
In PD pathogenesis, neuroinflammation has been recognized as an important
mechanism of the disease [127-128]. Activation of microglia has been demonstrated
in SN and striatum from post-mortem PD brains and in PD animal models [129-131].
Pro-inflammatory cytokines, such as IL-1β, IL-6, and TNF-α, are elevated in the CSF
and basal ganglia in PD patients [132]. The SNpc of PD patients shows large
numbers of activated microglia and reactive astrocytes. These two cell types are
presumably responsible for the increase of these cytokines in the nigro-striatal
pathway since they are able to produce and release cytokines. In turn, these
cytokines may also activate the surrounding microglia and astrocytes but may also
act on neurons [61, 129]. In vitro, both aggregated and nitrated forms of α-syn can
directly trigger a microglial response and release of cytotoxic factors [133-135]. In
mouse models, α- syn or modified forms of the protein can trigger both microglial and
humeral responses [136-137] and inhibition of NF-KB signalling seems to be
neuroprotective [138]. Given the evidence for neuroinflammation in PD, agents with
anti-inflammatory effects have been investigated for their neuroprotective potential.
Many of these anti-inflammatory drugs are already in common use for other purposes
of neuroprotection. Non-steroidal anti-inflammatory agents (NSAIDs) for example,
reduce dopaminergic cell death in animal and culture PD models [139-141], and
minocycline, another agent with anti-inflammatory capabilities, is currently being
investigated in human trials [142]. More investigation about this topic is needed also
because it is still not clear whether the inflammatory response is a cause or a
consequence of dopaminergic cell loss, and it is not known the release of
inflammatory factors is a part of a harmful or protective mechanism toward the
dopaminergic neurons.
III.II.IV Excitotoxicity
Excitotoxicity has been implicated as a pathogenic mechanism in several
neurodegenerative disorders including PD. IN the mammalian central nervous
system glutamate is the primary excitatory transmitter and primary driver of the
excitotoxic process. Dopaminergic neurons in the SN have high levels of glutamate
receptors and receive glutaminergic innervation from the subthalamic nucleus and
cortex. Excessive NMDA receptor activation by glutamate increases intracellular
calcium levels that activate cell death pathways [143]. Calcium influx produced by
excessive glutamate receptor activation can also promote peroxynitrite production
through the activation of nitric oxide synthase [144]. Levels of 3-nitrotyrosine, a
marker of peroxynitrite formation, are increased in post-mortem SN from PD patients.
NMDA receptor antagonists protect against dopaminergic cell loss in MPTP models
[145-146], but there is a major limitation to clinical application because of the low
potency and poor tolerability of the currently available agents. For example, riluzole
has glutamate antagonist properties, but failed to show any neuroprotective effect in
a small clinical trial [147]. Neuroprotective effects have also been attributed to
amantadine, which has modest NMDA antagonist properties as well as other actions
[148]. Human dopaminergic neurons have NMDA receptors with an unusual subunit
composition characterized by abundant expression of the NR2D subunits, which
have physiological and pharmacological properties distinct from the receptor types
found in many other regions of the brain [149]. The development of NMDA
antagonists with selectivity of specific channel subunits can be a potential
neuroprotective strategy
20
III.II.V Apoptosis
Apoptosis (programmed cell death) is a mechanism that has been demonstrated to
participate in neural development and play an important role in some forms of neural
injury. There are still some questions about whether apoptosis is directly involved in
PD. Several pathological studies have revealed signs of both apoptotic and
autophagic cell death in the SN of PD brains [150-152], although the extent is limited.
This is perhaps because of the slow process of cell death in PD. A Recent in vitro
study of Sun et al. (2010) [153] indicate that Insulin like growth factor-1 (IGF-1), a
neurotrophic factor, protects PC12 cells exposed to MPP + from apoptosis via the
GSK-3beta signalling pathway, this neurotrophic factor is absent in PD. Alterations in
cell death pathways are unlikely to be the primary cause for PD, but both apoptotic
and autophagic cell death pathways are possibly linked to oxidative stress, protein
aggregation, excitotoxicity, or inflammatory processes [154]. It is possible that
alterations in cell death pathways might trigger some of these pathological
processes. The activation of the cell death pathways most likely represents endstage processes in PD neurodegeneration. Therefore, inhibitors of these cell death
pathways have been proposed as potential neuroprotective agents regardless of the
initial cause for neurodegeneration in PD (see also Chapter IV).
III.II.VI Loss of neurotrophic factors
The loss of neurotrophic factors has been implicated as a contributor to cell death
observed in PD. The neurotrophic factors brain-derived neurotrophic factor (BDNF),
glial-derived neurotrophic factor (GDNF), and nerve growth factor (NGF) have all
been demonstrated to be reduced in the nigra in PD [155-157]. Treatment with
growth factors has therefore been proposed as a potential neuroprotective therapy in
PD. Indeed, the potent ability of these agents to stimulate growth and branching of
dopaminergic neurons suggests that they may be useful neuroprotective treatments,
even if deficiency of the factors is not the primary cause of the disease process.
However, issues relating to compound delivery and potential side effects have limited
the clinical application of this treatment strategy. The recent identification of
conserved dopamine neurotrophic factor (CDNF) and mesencephalic-astrocyte–
derived neurotrophic factor (MANF), which constitute a new class of neurotrophic
factors active against dopaminergic neurons, may provide new hope for therapeutic
approaches to neurodegenerative disorders based on neurotrophic factors or
downstream components of their signalling pathways [158-159]. Glial cell-line derived
neurotrophic factors (GDNF) and CDNF can protect and repair the nigrostriatal
dopaminergic system in animal models of PD in vivo. Despite promising clinical data,
intracerebroventricular infusion of GDNF in PD patients resulted in no therapeutic
benefit and produced serious side effects [160]. The poor outcome in the clinical trials
with GDNF may result from the insufficient concentration at the site of
neurodegeneration. GDNF binds with high affinity to heparin sulphates in the
extracellular matrix (ECM) that limits the volume of its distribution. It is therefore
important to find another or other neurotrophic factor(s) with a low affinity to ECM
[161-162]. CDNF and MANF are secreted proteins with eight cysteine residues.
MANF showed protection of embryonic nigral dopaminergic neurons in vitro
[159,163]. MANF protein is up regulated in cerebral ischemia in rats and is
cytoprotective against endoplasmatic reticulum (ER) stress in various cell lines
[159,164]. CDNF and MANF are both expressed in the striatum. MANF and CDNF
provide better protection against DA degeneration than GDNF because their local
diffusion and transport profiles are more efficient. Protection of striatal dopaminergic
21
cells may be achieved with various neurotrophic factors acting on different neuronal
circuits [165]. Although in vitro studies on CDNF and MANF look promising for the
protection against PD; it’s still not clear what the effects of these compounds are in
vivo. This extrapolation requires more caution.
Chapter: V Neuroprotective factors
In 2003, the Committee to Identify Neuroprotective Agents in Parkinson’s (CINAPS)
published an assessment of potential neuroprotective compounds. Twelve of these
compounds where prioritized to be further investigated in clinical trials [166]. Since
then, the list of potential therapies grew longer, but still there are no convincing
outcomes of clinical trials. Some of those listed strategies are still under intense
study; only the most promising are listed below and presented in table II [106].
V.I Adenosine receptor antagonists
Several epidemiological studies have indicated that caffeine may have some
influence on the incidence of PD, at least in men [167-168]. The finding that caffeine
mediates its action by antagonizing adenosine receptors led to the evaluation of
adenosine receptor antagonists as potential neuroprotective factors. In the striatum,
the A2a receptor can heterodimerize with the D2 receptor to inhibit dopamine
signalling [169-170], while inhibition of the A2a receptor can promote dopamine
function. Two small clinical trials of the A2a antagonist istradefylline has
demonstrated potential symptomatic effects in advanced PD [171-172]. Recent
research has even suggested that A2a antagonist also be neuroprotective. Both
caffeine and istradefylline are neuroprotective in the MPTP model [173-174]. A
potential advantage of these antagonists is that they have also been shown to be
neuroprotective in non-dopaminergic brain areas in animal models so that they also
22
protect against PD neurodegeneration found in regions besides the SN. In Chapter
IV the neuroprotective role of caffeine will be discussed more specifically.
VI.II Anti-inflammatory agents
As mentioned in Chapter III, inflammation has been recognised as one of the
possible pathological mechanisms for PD [67]. Anti-inflammatory agents, like
Nonsteroidal anti-inflammatory drugs (NSAIDs) and minocycline have been pursued
to be potential disease-modifying treatments against PD [175-176]. In vivo and In
vitro studies both have shown that certain NSAIDs, like aspirin, have neuroprotective
qualities. The only problem is that it is not yet known at what dose or exposure time
these agents will provide neuroprotection [177]. Different epidemiological studies
have shown different and conflicting results. In a study of Chen et al. the results
showed that NSAID use can lower the risk of PD by 45% while a follow-up study of
the same group of researchers have shown that only ibuprofen has this effect [178].
Also other studies did not show any significant neuroprotective effect of NSAIDs
[179-181]. So it is still unclear that any of the currently available NSAIDS have
neuroprotective properties in PD. Still, targeting of neuroinflammation mechanisms
can be a solution to prevent, cure or even slow the disease process of PD. An
alternative approach of targeting neuroinflammation may be the use of statins (3hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors) These statins are a class
of drug used to lower cholesterol levels. These drugs have also anti-inflammatory
effects, including reduction of nitric oxide and superoxide production by microglia
[182]. They also may play a role in scavenging free radicals [183]. The use of statins,
especially simvastatin, has been shown to reduce dopamine loss in acute MPTP
animal models and is associated with reduced PD incidence [182]. Minocycline is a
second generation tetracycline that has been used as antimicrobial agent. This agent
showed anti-inflammatory effects that were independent of its microbial activity.
Minocycline can block microglial activation and therefore may also have antiapoptotic activity. In both MPTP and 6-OHDA animal models the agent protects
against dopaminergic cell loss [184-186].
IV. III Alpha-synuclein-directed therapies
Alpha-synuclein appears to be an important mediator of toxicity in PD. Disruption of
α-syn aggregation has been the focus of research to develop new therapies against
PD. This aggregation can be reduced by several ways: 1) by reducing the α-syn
protein; 2) by increasing the clearance of α-syn; 3) by preventing and reducing
chemical modifications that can promote aggregated species; and 4) by the direct
interference with aggregation. Methods to reduce α-syn protein production include
small-molecule modifiers of transcription and RNAi-based methods, knocking down
translation.[187] Increasing the α-syn clearance can be done by activating
proteosomal or lysosomal pathways. Another option is to promote chaperon function
or activation of lysosomal degradation.[188-189] As oxidative modification and
phosphorylation of α- syn both promote aggregation of α- syn, antioxidant therapies
and kinase inhibitors could also help reduce α- syn aggregation and toxicity [190191]. The direct blockage of α- syn could be developed into therapeutic strategies for
PD. Peptide- based inhibitors have been developed that can block α-syn self
association and aggregation [192-193]. Although promising, these therapies are still
in an early stage and need more research.
23
IV. IV Kinase inhibitors
Mutation in the Leucine-rich repeat kinase 2 (LRRK2) gene is the most abundant
genetic cause of PD [194-195]. The gene itself codes for a large protein called
dardarin. This protein contains a serine/threonine kinase domain and a GTPase
domain. The exact function of this protein is not known jet, but an increase in kinase
activity is associated with the most common pathogenic mutation of the gene [196].
The evidence that pathogenic mutations increase this activity makes it an important
target for neuroprotection therapy. Kinases are good targets for small molecule
therapies and certain therapies for other disease are often based on inhibition of
kinase activity. Still, the development of LRRK2 kinase inhibitors is very difficult
because the endogenous substrates for LRRK2 are unknown. The function of the
gene and its protein needs to be further characterised before the kinase inhibitor can
be used in neuroprotective therapy.
IV. V Trophic factors
These factors are being used in neuroprotective therapies against PD for a long time
and still have a promising potential for future research. The factors themselves are
very well known, no further detail about the cell death mechanism in PD is needed for
a trophic factor approach. Trophic factors enhance dopaminergic survival,
independent from the mechanism of cell death. But on the other hand, they directly
target the dopaminergic deficit and not the non-dopaminergic aspects of the disease.
A good example of a well known neurotrophic factor is Insulin-like growth factor 1
(IGF-1), which has been shown to prevent neurodegeneration and promote
regeneration in many animal models of PD. For example, administration of IGF-1 or
the N-terminal fragment of IGF-1 given shortly after a 6-OHDA lesion prevented the
loss of dopamine neurons in the SN and reversed behavioural abnormalities [197].
The earlier mentioned growth factor GDNF was first shown to promote dopaminergic
neuronal survival and neurite outgrowth in cell culture [198], and since then
numerous reports have shown its powerful neurotrophic effects in both rodent and
primate models of PD. It might be very interesting to explore these growth factors
further in models of PD both in vivo and in vitro, and might have some clinical
relevance for the future treatment of the human disease.
IV. VI Antioxidants
Epidemiological studies have shown that uric acid might be a potential
neuroprotective agent in PD. Uric acid is an antioxidant that acts by scavenging
reactive oxygen and nitrogen species [199]. Several studies have shown that
subjects with high serum urate levels have a decreased incidence of PD [200-201]. In
the early stage of PD the higher plasma urate levels correlates with slower disease
progression [202]. In culture (in vitro), uric acid can reduce the dopaminergic cell
death in response to rotenone (insecticide) and homocysteine [203]. Recent studies
have shown that a urate-rich diet could help to reducing the risk of developing PD
and even could serve as a neuroprotective therapy in PD [204]. The problem with
urate-rich diets is that it causes a higher risk of developing gout and cardiovascular
diseases. Another surprising and promising neuroprotective compound, which also
can act as antioxidant, is nicotine, and will be discussed in the next chapter.
24
Chapter: V Three important neuroprotective factors
The most striking finding in PD studies is the possible neuroprotective role of
nicotine, caffeine and estrogens as possible neuroprotective agents against PD.
There is not much known yet about the mechanism of these possible neuroprotective
agents nevertheless these neuroprotective agents can lead to a new generation of
therapies against PD. This chapter will be dedicated to these three promising
neuroprotective factors. Figure 3 shows a schematic overview of this chapter.
V.I Nicotine
Smoking cigarettes is a known health hazard and number one cause of mortality and
morbidity. It is associated with a risk of serious chronic disorders, including
cardiovascular disorders, lung disease, and cancers. Surprisingly smoking cigarettes
appear to have beneficial effects against PD. Since initial epidemiological findings in
the early 1960s, numerous case- and cohort studies report a reduced incidence of
PD in smokers [205-214]. The neuroprotective effect of smoking in PD is correlated
with increased intensity and duration of smoking, is reduced with smoking cessation,
and occurs with different types of tobacco products [205-214]. Importantly, it does not
appear to be due to selective survival of PD cases or reporting bias [205-214]. These
findings implied that the decline in PD with smoking is a true biological effect.
Table II: Nicotine pre-treatment protects against nigrostriatal damage
in different parkinsonian animal models.
Animal
model
Nigrostriatal Nigrostriatal
insult
treatment
regimen
Protection
References
Rats
6-OHDA
Injection,
drinking water
Improvement
in
behavioural
deficits
and molecular/
functional measures
in striatum
[114,115,
120, 121]
Monkeys
MPTP
Drinking water
Improvement
in
molecular
and
functional measures
in striatum
[101,
125]
Mice
MPTP
Injection drinking Variable effects —
water
protection in some
studies but not in
others
124,
[126, 127]
Although smoking is not rational and hazardous, these data are useful and may
provide insight about mechanisms to reduce the occurrence of PD. Besides, it can
provide a new treatment strategy to manage PD.
Many studies on the influence of smoking on the protection against nigrostriatal
damage have been performed. Experiments with different parkinsonian animal
models have provided the evidence that nicotine exposure improves dopaminergic
markers and function in the lesioned striatum, the brain region that is predominantly
25
affected in PD [215-218] (Also see Table IV). These data will provide a base for the
suggestion that nicotine in smoke may contribute to the neuroprotective effect of
tobacco use in PD.
V.I.II Nicotine neuroprotective but not neurorestorative
Although experiments in animal models have proven that nicotine may have
neuroprotective effects on nigrostriatal damage and probably on the protection for
PD, the question is raised whether nicotine only protects against developing damage
and/or whether it can also restore integrity of damaged dopaminergic neurons. In a
very recent study of Quik et al. [219] the authors tested whether nicotine given before
and/or after nigrostriatal damage improved striatal dopaminergic function in two wellestablished parkinsonian animal models, unilateral-lesioned 6-hydroxydopamine (6OHDA) rats and MPTP-treated monkeys. This test was done to distinguish the two
alternatives; neuroprotective and neurorestorative. In the rat study, animals were
given nicotine both before and after an unilateral 6-OHDA-induced lesion of the
medial forebrain bundle and the data were compared to data on rats exposed to
nicotine given two weeks after lesioning only. The results showed that combined
nicotine pre- and post-treatment reduced behavioural deficits and ameliorated lesioninduced losses of striatal dopaminergic markers. But nicotine administered two
weeks after lesioning did not have these same effects. In a monkey study, there was
a similar effect; here the result was improvement in striatal dopaminergic markers
when nicotine was given before and during the development of nigrostriatal damage.
However, nicotine treatment did not improve dopaminergic integrity in the striatum of
monkeys with pre-existing nigrostriatal damage. These data showed that nicotine
does not restore the function once dopaminergic neurons have been damaged, but
that it attenuates ongoing neurodegenerative processes. Since PD is a progressive
neurodegenerative disorder, the results from experimental animal models would
suggest that nicotine might reduce PD progression [219].
V.I.III The Mechanism
Now that it is revealed that there is indeed an inverse relationship between the use of
tobacco and PD incidence it is important to know how nicotine is neuroprotective in
PD, and what its target(s) are. This knowledge can be used to develop a new therapy
with minimum or adverse side effects.
In general, nicotine exerts its effects in the peripheral and central nervous system by
stimulating nicotinic Acetylcholine receptors (nAChr). These are pentameric ligandgated ion channels composed of α and β subunits or only α subunits [220-225]. The
nAChrs in the peripheral nervous system and the brain are distinct from each other,
providing an opportunity of selective targeting of the desired receptors. The most
relevant nAChrs in the pathophysiology of PD are most likely the ones in the
nigrostriatal tract. It has proved quite challenging to identify these nAChrs because
multiple subtypes are expressed with six different α- (α2, α3, α4, α5, α6, and α7) and
three different β- (β2, β3, β4) subunits in the nigrostriatal pathway. But only selective
nAChr subtypes are present in the striatum including the α4β2*, α6β2* and α7 nAChr
populations [220-222, 225-226] (the asterisk indicates the possible presence of other
subunits in the receptor complex). Evidence for their presence is based on a wide
variety of approaches, including work with nAChr-null mutant mice as well as nAChr
subtype selective antibodies and lesion studies [220-222, 227]. Recent work has
indicated that the α6b2* nAChrs are composed of several subtypes, including the
α6α4β2* and α6(non α4)β2* populations [228-229]. Interestingly, these two α6β2*
26
subtypes appear to be differentially regulated with chronic nicotine dosing [230]. A
study with nAChr null mutant mice indicated that the α6α4β2* nAChr population may
be important for this effect of higher frequency stimulation on dopamine release
[230]. The α6α4β2* and α6(non-α4)β2* nAChrs subtypes are not only variably
affected by nicotine exposure, but they also appear to be differentially affected by
nigrostriatal damage. For instance, the α6α4β2* nAChr subtype is more susceptible
to lesions than the α6(non α4)β2* or α4β2* nAChr populations in parkinsonian
rodents and monkeys [230]. The data may indicate that the α6α4β2* nAChr subtype
is expressed on dopaminergic terminals that are more susceptible to nigrostriatal
degeneration. Nicotine-mediated neuroprotection against nigrostriatal damage also
appears to involve various nAChr subtypes [231]. The involvement of the α4β2*
nAChr subtype is indicated in studies showing a loss of nicotine-mediated protection
in α4β2* nAChr knockout mice with nigrostriatal damage [232]. The role of α6β2*
nAChr subtypes in neuroprotection is indicated in a study with lesioned rats using the
neurotoxin α-conotoxin MII (a-CtxMII) E11A to differentiate between α6α4β2* and
α6(non α4)β2* subtypes [231,233]. Receptor competition studies in control and
lesioned rats treated with and without nicotine showed that the α6α4β2* subtype is
only present when nicotine- mediated protection is observed. This latter subtype may
be necessary for neuroprotection and a target for the development of protective
strategies against Parkinson’s disease. The mechanisms whereby interaction at
α6α4β2* nAChr results in the protection against nigrostriatal damage are not yet
known, as the intracellular signalling pathways linked to this specific nAChr subtype
are not identified yet. However, based on knowledge of other nAChr subtypes, one
might anticipate that changes in multiple downstream pathways are involved, such as
alterations in various kinases, including phosphatidylinositol 3-kinase (PI3K), protein
kinase B (PKB), mitogen-activated protein kinase (MAPK) and jnk kinase, caspases
3, 8 and 9, nitric oxide synthase, the cell survival protein Bcl-2, and other intracellular
events [221, 234-235]. Activation of these intracellular messengers may modulate
immune responsiveness to enhance neuronal function [236-237]. They may also
activate different trophic factors, such as brain-derived neurotrophic factor (BDNF)
and/or basic fibroblast growth factor-2 (FGF-2) levels, which are implicated in
neuroprotection for nigrostriatal damage [238-240]. Treatment with nAChr ligands
directed to these subtypes may thus yield optimal therapeutic benefit for Parkinson’s
disease, with a minimum of adverse side effects.
V.I.IV The influence of nicotine on the gene expression in PD
Genes involved in determining dopamine signalling and disposition have been the
focus of many recent epidemiologic studies of Parkinson’s disease (PD). More
specifically, polymorphisms in the genes encoding monoamine oxidase B (MAO-B)
and monoamine oxidase A (MAO-A) have been explored as potential risk factors for
PD. Both MAO-A and MAO-B are located on the X chromosome; their protein
products are mitochondrial enzymes that catabolise dopamine, although their sites of
expression differ by cell type [241]. The dopamine D2 receptor, an auto-receptor, is
encoded by DRD2 (chromosome 11q23), a gene that is also polymorphic and is
considered to be a candidate gene in PD as well. Several case-control studies have
shown that a single nucleotide polymorphism (SNP) in intron 13 of the MAO-B gene
(A→G) substitution 36 bases upstream of exon 14 boundary) is related to PD risk
[242]. In a previous study the researchers reported that individuals with the G allele
had approximately two times increased risk of PD (OR) =2.09; 95% CI: 1.18–3.69)
[243]. Moreover, the inverse relation between smoking and PD was modified by the
27
intron 13 SNP. The protective effect of smoking was limited to subjects with the G
allele (OR=0.24 (95% CI: 0.10–0.55)) [244]. These findings have been replicated in
an Australian population [245], whereas no interactions were observed in a study of
PD in US health professionals [246]. Population-based surveys have indicated that
the incidence of PD is considerable higher in men than in women [247]. Kelada et al.
(2002) [248] therefore hypothesized that gender might modify the associations
among smoking, MAO-B intron 13 genotype, and PD. They tested for gender-specific
interactions between smoking and genetic polymorphisms of monoamine oxidase B
(MAO-B) intron 13 (G or A allele), monoamine oxidase A (MAO-A) EcoRV (Y or N
allele), and dopamine D2 receptor (DRD2) Taq1B (B1 or B2 allele) in a case-control
study of 186 incident idiopathic Parkinson’s disease (PD) cases and 296 age- and
gender-matched controls. The odds ratios (ORs) for PD risk for ever smokers versus
never smokers were 0.27 (95% CI: 0.13–0.58) for men of genotype G, and 1.26
(0.60–2.63) for men of genotype A (interaction w2 = 8.14, P = 0.004). In contrast, for
women, the OR for ever smokers versus never smokers were 0.62 (95% CI: 0.25–
1.34) and 0.64 (95% CI: 0.18–2.21) for women of genotype GG/GA and AA,
respectively (interaction w2 = 0.001, P=0.975). No interactions were detected
between smoking and either MAO-A EcoRV or DRD2 Taq1B genotypes. These
results suggest that a strong gender difference exists with respect to the modifying
effect of MAO-B genotype on the smoking association with PD. Estrogen and nicotine
both have an inhibiting effect on MAO-B, it is possible that estrogen and tobacco
smoke constituents interact with MAO-B in different ways to modify PD risk in
women. For men, neuroprotection by tobacco smoke constituents varies by MAO-B
intron 13 genotype. The overall conclusion is that smoking inhibits MAO-B and
therefore act as a neuroprotective factor against PD.
V.I.V Nicotine as antioxidant
Yet another hypothesis is that nicotine might provide some of its therapeutic actions
in PD and AD through antioxidant mechanisms [249].
Initial chromatographic studies suggest that nicotine can affect the formation of the
neurotoxin 6-hydroxydopamine resulting from the addition of dopamine to Fenton's
reagent (i.e., Fe2+. and H2O2). Thus, under certain circumstances, nicotine can
strongly affect the course of the Fenton reaction. In in vivo studies, adult male rats
being treated with nicotine showed greater memory retention than controls in a water
maze task. However, neurochemical analysis of neocortex, hippocampus, and
neostriatum from these same animals revealed that nicotine treatment had no effect
on the formation of reactive oxygen species or on lipid peroxidation for any brain
region studied. In an in vitro study, addition of various concentrations of nicotine to rat
neocortical homogenates had no effect on lipid peroxidation compared to saline
controls. The results of these studies suggest that the beneficial/protective effects of
nicotine in both Parkinson's disease and Alzheimer's disease may be, at least partly,
due to antioxidant mechanisms [249].
V.II Caffeine
Because cigarette smoking has adverse effects on human health and because it is
difficult to determine whether nicotine or other tobacco chemicals may be potentially
beneficial in the prevention against Parkinson disease, alternatives are extensively
investigated. In contrast, the identification of caffeine as the explanatory molecule for
28
a reduction in the risk of PD among coffee drinkers and the discovery that caffeine
reduces the dopaminergic neurotoxicity in PD animal models are promising.
V.II.I Caffeine Reduced PD and the Role of Estrogen
As mentioned earlier the effects of caffeine on the central nervous system are
mediated primarily by its antagonistic actions at the A1 and A2A subtypes of
adenosine receptors [250]. The action of caffeine on A2A receptors is most likely
relevant to PD because the expression of these receptors are only observed in the
striatum, and because genetic inactivation of the A2A receptors or selective A2A
antagonist , like caffeine , remove the dopaminergic neurotoxicity in animal models of
PD [251]. In prospective studies, it is shown that the risk of PD is reduced among
men who regularly drank coffee [252-253], whereas in on women such association
has not been found yet [252-254]. The gender difference could be explained if the
effect of caffeine on risk of PD depends on the levels of estrogen. In a large
prospective study on post menopausal women who did not take estrogen
replacement therapy there is found a reduced risk of PD [255].
In a large cohort study of Ascherio et al. [256] the investigators found that
consumption of coffee was associated with a reduced PD mortality among men and
among women who never used post menopausal estrogens. On the contrary, PD
mortality among women who used estrogen was independent of the consumption of
coffee. These results suggest that post menopausal estrogens modify the effects of
caffeine on risk of PD. In both men and women a significant reduction in PD risk was
present at low levels of caffeine (3-6 cups of coffee a week), and a little further
reduction of higher amounts of caffeine intake [256]. The results of this study thus
suggest that caffeine reduces the risk of PD but that this may be prevented by the
use of estrogen replacement therapy. The results of a MPTP mouse study of Chen
et. al. [173] showed that these two agents may work through a common mechanism
to prevent MPTP toxicity. Estrogen may compete with caffeine for its activation of a
protective pathway. Besides, estrogen and caffeine as well as MPTP share a
cytochrome P450, CYP1A2, for their metabolism or detoxification. Therefore,
metabolism of caffeine and/or estrogen could alter MPTP metabolism. The effects of
estrogen on the risk of PD will be further discussed in the next chapter (III.III).
V.II.II The Mechanism
The detailed mechanisms how caffeine suppresses neuronal death have not been
fully understood yet. Nevertheless, in a study of Nakaso et al. [257] Researchers
investigated the cytoprotective mechanisms of caffeine using human dopaminergic
neuroblastoma SH-SY5Y cells as a PD model. Caffeine prevented the apoptotic cell
death that was induced by serum/retinoic acid (RA) deprivation, MPP+, rotenone,
and 6-OHDA in SH-SY5Y cells in a dose dependent manner. Caffeine lowered
caspase-3 activity induced by serum/RA deprivation and 6-OHDA administration, and
also decreased the number of apoptotic condensed and/or fragmented nuclei. Akt
(also known as protein kinase B (PKB) was phosphorylated 60 min after caffeine
administration in a dose dependent manner; PI3K inhibitors, wortmannin and
LY294002 cancelled this cytoprotective effect of caffeine. MAP kinases such as
Erk1/2, p38, or JNK on the other hand, were not activated by caffeine. These results
suggest that caffeine has a cytoprotective effect due to the suppression of apoptotic
signals or the up-regulation of cytoprotective signals. Therefore, the authors
investigated the signal transduction pathways in SH-SY5Y cells following caffeine
administration and came to the conclusion that caffeine had a cytoprotective effect by
29
the activation of the PI3K/Akt pathways in SH-SY5Y cells. To fully understand the
mechanism in which caffeine can help to prevent progression of PD further
investigation on this topic is needed.
V.III Estrogen and PD
Experimental, epidemiological, and clinical evidence suggest that female sex
hormones may influence the onset and severity of PD symptoms. For instance, PD is
more common in men than in women (male to female ratio 3:2) [258]. This ratio
suggests that estrogen has a possible protective influence in predisposition of the
disease. Gender difference in estrogen levels may also explain why the dopaminergic
drugs that are used to treat PD affect men and women differently with regard to
therapeutic response, drug clearance, and blood pressure [259-260].
This is supported by several animal studies that have demonstrated estrogenic
modulation of pre- and postsynaptic indices of dopaminergic function within the SN
and the striatum, as well as estrogens’ ability to protect dopaminergic neurons from
MPTP and other toxins. Clinical reports suggest a very potent protective effect of
estrogen replacement therapy (ERT) on the onset and the progression of PD and
PD-related dementia [261-262].
V.III.I Estrogens and the Nigrostriatal Dopamine System
Estrogen binds to intracellular receptors that enter the nucleus and act as
transcription factors to regulate the gene expression [263]. These estrogen receptors
were thought not to be expressed in the striatum and SN [264], but recent studies,
using more sensitive techniques, report their expression in these regions [265-266].
Adding to the body of evidence is the observation that estrogens may act as well via
non-genomic mechanisms such as membrane receptors, and regulation of ion
channels [264, 267]. These effects can occur within seconds or minutes; this is too
rapid to be caused by the activation of ‘classical’ receptors like the intracellular
estrogen receptors [264, 268]. The exact mechanism by which estrogen exert its
effects is still not clear but it is evident that estrogen have some profound effects on
the functions of dopaminergic neurons in the striatum and SN, which are relevant for
the understanding of PD. However, several animal studies with ovariesectomized
(OVX) and gonadally intact rats suggest that estrogen alters the function of both
presynaptic SN neurons and their postsynaptic targets in the striatum and thereby
exerting a potent modulatory influence over dopaminergic transmission within the
basal ganglia [269]. However a clear picture of estrogens’ effects has not yet
emerged therefore further preclinical research is needed in order to shape the design
of future clinical studies of estrogen influences on PD.
V.III.II Neuroprotective Effects of Estrogen in PD Animal Models
A number of animal studies show that estrogens protect dopaminergic neurons from
injury. Cultured mesencephalic neurons incubated in medium containing estradiol
were resistant to bleomycin sulphate (BLM)-induced apoptosis [266]. BLM is an anticancer drug with two molecular domains: one binds to nuclear DNA and the other
acts as a radical generator. A specific estrogen receptor antagonist IC 182, 780 can
block this effect, suggesting that the neuroprotective effect is mediated by the nuclear
estrogen receptors [266]. In the presence of estrogen in animal models of PD using
MPTP and 6-hydroxydopamine (6-OHDA) neuronal survival was shown. The
estrogen may interfere with the uptake of MPTP and 6-OHDA into the nigral
dopaminergic neurons or alter DA release and reuptake in remaining cells [270]. This
30
is possibly due to an estrogen-related decrease in the binding affinity of DA at
presynaptic reuptake sites. The most common used neurotoxin in animal studies on
PD is MPTP; this is because the compound produces degeneration of the
nigrostriatal dopaminergic system thus inducing PD symptoms in animals (see
chapter II.II) [271-272]. The evidence that pre-treatment with estradiol protect
against the effects of MPTP is shown by an increase in DA concentration in mice. In
rats a similar effect is seen when MPP+ is directly infused. In rat experiments MPP+
is used instead of MPTP in mice because rats cannot metabolise MPTP as can mice.
Further findings in primate research implied that estrogens are critical in the
maintenance of a subpopulation of nigral dopaminergic neurons [160]. Leranth and
colleagues [273] found that more than 30% of the nigral dopaminergic neurons were
lost 30 days after ovarisectomy in monkeys. The results of this study suggest that
estrogen is possibly necessary in the maintenance and the survival of nigral
dopaminergic neurons. The way estrogen might protect neurons is via antioxidant
effects or neurotrophic effects [266]. In cultured rat ventral mesencephalic neurons,
estradiol attenuates the formation of toxic free radicals by glutamate [266] and in
other animal studies estrogen has been demonstrated to have an effect on the
regulation of GDNF,, a member of the transforming growth factor family [274-276].
The exact mechanism behind these possible forms of estrogen induced
neuroprotection has yet not been demonstrated.
31
Nicotine
Caffeine
Estrogen
nAChr
receptor
A2A
receptor
Estrogen
receptor
Pesticides
(Dieldrin)
GABAA
receptor
(intracellular)
Glutamate
Calcium
influx
Neuronal cell death:
- Oxidative stress
- Mitochondrial dysfyuntion
- Protein aggregation +
Misfolding
- Neuroinflammation
- Excititoxicity
- Apoptosis
- Loss of neurotrophic factors
Gene expression
(nucleus)
Figure 3: Overview of neuroprotective factors and their receptors. Estrogen normally binds to the
intracellular estrogen receptor and activates gene expression in the nucleus. Estrogen might also act
on the extracellular receptor A2A in a competitive manner together with caffeine and attenuates the
formation of toxic free radicals by glutamate. There is evidence that nicotine, caffeine and estrogen
have a reducing effect on processes that will lead to cell death. Many toxic compounds (Dieldrin used
as an example) have a inducing effect on neuronal cell death.
32
Chapter VI: Discussion and Future Research Leads
VI.I Conclusion/Discussion
It is still hard to diagnose PD although there are several helpful clues to indicate if
patients are dealing with PD or another form of parkinsonism [2]. Besides,
patients often not only have the dominating motoric symptoms but also complaints
of other non-motoric symptoms that eventually lead to dementia. This can be one
of the reasons for misdiagnosis of PD in patients. In PD and Parkinson- plus
syndromes the SN neurons will degenerate, and will result in a deficiency of
striatal DA concentration [3-7]. The cause of this DA neuron death is not totally
clear yet but there are good evidences in different studies that processes like
oxidative stress, excitotoxicity, inflammation and loss of neurotrophic factors may
have a large influence on this process [8-10]. The combination of
neuroinflammation [61-69], exposure to environmental influences (like pesticides)
and genetic influences (for example the polymorphisms in genes that function in
dopamine signalling pathways) [73-80] appear to be involved in most cases of PD
that are sporadic, as mentioned in Chapter II.
Although several epidemiology studies in developed countries, like the study of
Leentjens et al. [41] and van den Eeden and co-workers [44], show comparable
incidence rates, it is still a crude measurement because of the difference in study
methods and misdiagnosis of PD. The differences in the overall incidence
between these two studies can be explained by differences in strategy, patient
registration and accuracy. Although there are differences in incidence rates
between different studies, it is mainly observed that women are less susceptible
to PD than men as they show a lower incidence rate, and that this difference is
possibly due to the neuroprotective influence of estrogen in PD. This is confirmed
by studies with postmenopausal women [255].
The difference in PD incidence between different ethnic groups is not confirmed
yet [41, 44]. To measure incident rates in developing countries more accurate
there should be a better PD database. The prevalence of PD in these countries is
however most likely largely underestimated because of misdiagnosis and the lack
of competent medics. It is plausible that in developed countries PD is more
common than in developing countries as the people in developed countries have
a longer average lifespan and better medical care. Besides, in developed
countries neurotoxicants like pesticides and MPTP are more widely used and
spread because of the industrialisation. In contrast; in developed countries there
are more regulations by law on neurotoxicants, so maybe the people here are
less exposed. Therefore, studies with geographic variation need to be interpreted
with caution, as many factors beyond environmental exposure like migration,
chance etc. could determine the geographical pattern of the disease. [44, 52]
While research continues for environmental factors that can be associated with
PD, several studies have shown that there are several neuroprotective factors
that can be useful in the intervention of PD. These strategies might block or slow
degenerative processes of neurons in PD. Potential targets for these
neuroprotective factors are events like oxidative stress, mitochondrial dysfunction,
excitoxicity and inflammatory changes that lead to apoptotic and necrotic cell
death [8-10]. In 2003, the Committee to Identify Neuroprotective Agents in
Parkinson’s (CINAPS) published an assessment of potential neuroprotective
compounds. Twelve of these compounds where prioritized to be further
investigated in clinical trials. Compounds like adenosine receptor antagonists,
33
anti-inflammatory agents, antioxidants, alpha-synuclein blockers, kinase inhibitors
and trophic factors have all proven to have a protective effect against PD by
blocking or intervention of several degenerative processes and pathways in PD
models. However, lack of knowledge of the basics of PD and deficiencies in the
methodology used to study disease progression are current barriers. As a result,
there are still no convincing outcomes of clinical trials.
As research on PD continues, the list with potential neuroprotective therapies will
grow longer. The most striking is the possible role of nicotine, caffeine and
estrogen as neuroprotective agents in PD. Although smoking and the use of other
tobacco products is of great risk to human health, treatment with nAChr ligands,
other than nicotine, specifically directed to nAChr subtypes may yield optimal
therapeutic benefit [219- 240]. Another even more promising neuroprotective
agent is caffeine. Caffeine acts agonistically on the A2A receptors and has proven
to reduce dopaminergic neurotoxicity in PD animal studies [250-257]. The earlier
mentioned neuroprotective factor estrogen not only acts via an antioxidant effect
or neurotrophic effect to protect neurons, but has also a possible influence on the
neuroprotective characteristics of nicotine and caffeine [258- 276]. Several studies
have shown a positive influence of estrogen on the effect of nicotine and caffeine
in the neuroprotection against PD. As epidemiological studies already have
shown men indeed have a higher risk to develop PD because they lack a
physiologically efficient concentration of estrogen for neuroprotection. Based on
this knowledge one could conclude that neuroprotective factors act gender
specifically, and that each of the specific neuroprotective factors not only can
provide a potential new strategy for the protection against PD but also a potential
new strategy in combination with each other or with other therapies (like
Levopoda therapy).
As an overall conclusion, based on available literature, neuroprotection in PD
remains an important goal that can not be ignored. Successful neuroprotective
therapies could turn PD from a progressive and disabling disease to a problem
that can be managed. With the rising interest in the understanding and treatment
of PD, therapies might improve. In the next paragraph some possible
improvements are summarized.
VI.II Future Leads
Now that researchers still find new possible ways of neuroprotection against PD,
what can be done or improved with this knowledge in the future? Here are some
suggestions:
The research on neuroprotective factors must be extended to reveal the
exact mechanism and possible targets of any neuroprotective factor.
Better/strict diagnosis of PD patients and other parkinsonian syndromes
Improvement of education about PD in developing countries
Finding other possible neuroprotective factors that are less gender specific
Finding out the differences in mechanisms of PD in men and PD in women
Research on the effect of Neuroprotective factors on the genetic pathways
and expression of PD.
Research on the possible restoration effects of neuroprotective factors on
degenerated neurons.
34
Doing more research on the oxidative and antioxidant properties of
nicotine, caffeine and other possible neuroprotective agents.
Searching for (and maybe creating) other nAChr ligands than nicotine that
are of less hazardous to human health.
Searching for estrogen-like molecules that have the same neuroprotective
effect on PD, these molecules can replace estrogen supplements. These
new supplements can also provide men protection against PD without the
side effects of normal estrogens. This prevention can be useful when men
and women have a PD family background or are disposed to certain
environmental risk factors like pesticides.
Because pesticides are widely used in large amounts and because they
are possible risk factors on PD, it is of great importance to do more
research on the neurotoxicity of pesticides and other neurotoxicants and
especially their influence on DA degeneration and so the development of
PD. It is known that some pesticides can degenerate DA neurons, but it is
often not clear in what amount and at what exposure time. When this is
cleared up, maybe scientists can look if neuroprotective factors are a good
solution for protection against these neurotoxins;
And so more research on environmental risk factors for developing PD
These are only suggestions; maybe in the future scientists come up with better
suggestions and solutions for research on neuroprotective factors in PD (next
paragraph).
VI. III New research plan (??)
In the previous paragraph improvements on possible new research on
neuroprotective factors and PD are summarized. But what kind of experiment
would have the most achievable goal and will be relevant to the prevention and
understanding of PD? Looking at this thesis the most obvious choice of future
research would be research on the three most promising neuroprotective factors;
nicotine, caffeine and estrogen. These three compounds have shown to prevent
nigrostriatal damage. However, one has to take into account the financial and the
ethical aspects. Time and the risk for human health are important to be taken in
account as well as the question whether the new experiment will be in vitro or in
vivo. In this paragraph the advantages and the disadvantages of possible new
research on the three earlier mentioned neuroprotective factors will be discussed.
It is proven with several epidemiological studies that there is indeed an inverse
relationship between tobacco smoke and the incidence of PD [205-214].
Furthermore, several mutant mice experiments have shown that nicotine exerts its
neuroprotective effect on nigrostriatal damage via the nAChr receptor [220-225].
But it is also known that smoking cigarettes, or other types of tobacco, is a health
hazard and the number one cause of serious chronic disorders and many kinds of
cancer. Looking at this ethical issue, is it useful to do further research on the
effect of nicotine on PD?
The answer would still be yes, because besides smoking there is another way to
expose experimental subjects to nicotine, namely via nicotine tablets. It is not
known if these tablets have any health hazard or that they will have the same
35
effect on nigrostriatal damage as smoking, but it seems a more ethical way.
Because nicotine acts via the nAChr receptor it may be possible to do research
on other nAChr receptors and its subtypes [227, 231]. In this thesis primarily the
in vivo experiments are described. The disadvantage of these in vivo experiments
is that knock-out or lesioned animals not necessarily represent the human in vivo
PD situation [231-233]. So, it is not clear whether nicotine or other nAChr ligands
will have the same effect in humans as in (lesioned) animal models. Hence,
extrapolation of the outcome of these experiments to humans who have PD (or
have the possibility to develop PD in the future) is tough. Another disadvantage of
these in vivo studies is the amount of animals used and also the costs. In vitro
experiments would be cheaper but the results will be even harder to extrapolate to
humans. Based on the knowledge of other nAChr subtypes, one might anticipate
that changes in downstream pathways are involved, and activation of these
receptors will result in the activation of intracellular messengers which are
involved in neuroprotection for nigrostriatal damage [236-237]. This is however
still a speculation, the exact pathway in which nicotine will have any effect on the
protection against nigrostriatal damage is still poorly understood. A nice new
experiment would therefore be the mapping of these pathways to understand
more of the underlying mechanism and other possible advantages and
disadvantages of nicotine and/or other nAChr ligands
PD is more common in men than in women [44], this suggests that estrogen has a
possible protective effect against nigrostriatal damage. This could be an
explanation for the difference in effects of PD treatment in men and women [259260]. Clinical reports suggest that estrogen have a very potent effect of Estrogen
Replacement Therapy (ERT) on the onset and progression of PD [261-262]. As
ERT is not available for men, who have a higher risk of developing PD, this is a
disadvantage. Normally estrogen binds to intracellular receptor and exerts gene
expression in the nucleus. There is however evidence that estrogen can also act
via non-genomic mechanisms such as membrane receptors and regulation of ion
channels [264, 268]. The exact mechanism by which estrogen exerts its effect is
still not clear. Therefore preclinical research on the exact mechanism and
pathways of estrogen is needed in order to make a new study design.
In a MPTP-induced animal model of PD, results showed the interference of
estrogen in MPTP uptake and 6-ODHDA into the nigral dopaminergic neurons
and alter DA release and uptake [270]. MPTP is used in animal studies because it
produces nigrostriatal damage in animal models [271-272]. Although it is known
that MPTP might have an acute effect on human health and development of PD
[56], one should be careful by making certain statements. Experiments with MPTP
do not prove that estrogen is a cure on PD, but more a protection against acute
poisoning with MPTP and possible other neurotoxicants [173]. Besides, estrogen
has only proven to have an effect on DA damage in animal models and not
specifically on PD, therefore the results can not easily be extrapolated to humans.
Because cigarette smoking has serious adverse effects on human health and
because it is difficult to determine whether nicotine or other tobacco chemicals
may be potentially beneficial in the prevention against PD, less research on
nicotine is done. On the contrary, the identification of caffeine as the explanatory
molecule for a reduction in the risk of PD is promising.
36
Caffeine not only has minimal hazardous effects on human health but is also easy
and cheap for intake. In prospective studies it is shown that the risk of PD was
reduced in man who drank regularly coffee. On women such association has not
been found yet. Caffeine exerts its effects via the A2A receptor [250-251].
Estrogen might also bind to this receptor, or act by the same mechanism, to exert
its neuroprotective effect. Therefore estrogen might compete with caffeine for its
activation of protective pathway. This is, however, never been proved but only
assumed by the results of a MPTP mouse study [173]. Again, it is for this reason
hard to make the assumption that caffeine and estrogen will act the same in (all)
humans and that caffeine and estrogen are specifically protective against PD and
not to other neuronal illnesses. The detailed mechanism by which caffeine
suppresses neuronal death has not been fully understood yet. Although Nakaso
et al. [257] have done in vitro research on the cytoprotective mechanism of
caffeine and its signal transduction pathways; it is still not fully clear how caffeine
protects against PD progression.
To conclude, all three neuroprotective factors have advantages as well as
disadvantages. Further research is important, but it is clear that it is still a long
road to find a cure against PD. Maybe researchers will find a combined
therapeutic strategy where nicotine and caffeine (or nicotine and estrogen) can
act together against nigrostriatal damage. Or they might find some other
compound (maybe by accident) that has neuroprotective properties.
Untill now the best option to investigate in the future is caffeine; it is cheap, it is
not for harmful humans and easy to use in epidemiological studies. Although
every human being can act differently on caffeine, it’s is still worth finding out
more about the mechanism in which caffeine exerts its neuroprotective effect and
what it can mean for people with PD or who are susceptible for PD. There are not
much known hazards of drinking coffee; it must be certain that drinking a lot of
coffee not causing any harm to human health and that the benefits are bigger
than the disadvantages. Coffee is known to be neuroprotective in both in vitro and
in animal studies, and sometimes it is easier to prevent than to cure. But because
PD in humans is hard to detect in before the onset of the symptoms, prevention is
of no use. The most important question one should ask in future research is: can
caffeine also be neurorestorative. Maybe it is not restorative in vitro or in animal
models but maybe in humans it will have different effects.
Further research is necessary to have a better understanding of the disease and
its mechanism, each step in research might eventually provide some relief or
protection against PD.
37
References
1. Fahn S, Przedborski S. Parkinsonism.
In: Merritt’s neurology (Rowland LP, ed),
pp 679-693. Philadelphia: Lippincott
Williams & Wilkins, 2000.
2. Fahn S. Description of Parkinson’s
disease as a clinical syndrome. Ann NY
Acad Sci 991:1–14, 2003.
3. Seibyl JP, Marek KL, Quinlan D, Sheff
K, Zoghbi S, Zea-Ponce Y et al.
Decreased
single-photon
emission
computed tomographic [123I] beta-CIT
striatal uptake correlates with symptom
severity in Parkinson’s disease. Ann
Neurol 38:589–598, 1995.
4. Eidelberg D, Moeller JR, Ishikawa T,
Dhawan V, Spetsieris P, Chaly T et al.
Assessment of disease severity in
parkinsonism
with
fluorine-18fluorodeoxyglucose and PET. J Nucl Med
36: 378–383, 1995.
5. Snow BJ, Lee CS, Schulzer M, Mak E,
Calne
DB.
Longitudinal
fluorodopa
positron emission tomographic studies of
the evolution of idiopathic Parkinsonism.
Ann Neurol 36:759–764, 1994.
6. Morrish PK, Sawle GV, Brooks DJ. An
[F-18]dopa-PET and clinical study of the
rate of progression in Parkinson’s disease.
Brain 119:585–591, 1996.
7. Benamer HT, Patterson J, Wyper DJ,
Hadley DM, Macphee GJ, Grosset DG.
Correlation of Parkinson’s disease severity
and duration with 123I-FP-CIT SPECT
striatal uptake. Mov Disord 15:692–698,
2000.
8. Di Monte DA, Langston JW Idiopathic
and
1-methyl-4phenyl1,2,3,6tetrahydropyridine
(MPTP)-induced
Parkinsonism. In: Neuroglia (Kettenmann
H, Ransom BR, eds), pp 997–989, 1995.
9. Olanov CW, Schapira AH, Agid Y
Neuroprotection for Parkinson’s disease:
prospects and promises. Ann Neurol
53(Suppl3):S1–2, 2003.
10. Jenner P Oxidative stress in
Parkinson’s disease. Ann Neurol 53:S26–
S38, 2003.
11.
Hunot
SM,
Hirsch
EC
Neuroinflammatory
processes
in
Parkinson’s disease. Ann Neurol 53:S49–
S60, 2003.
12. Gao HM, Liu B, Zhang W, Hong JS
Novel anti-inflammatory therapy for
Parkinson’s disease. Trends Pharmacol
Sci 24:395–401, 2003.
13. Schiess M Nonsteroidal antiinflammatory drugs protect
against
Parkinson neurodegeneration: can an
NSAID a day keep Parkinson disease
away? Arch Neurol 60:1043–1044, 2003
14. Chen H, Zhang SM, Herman MA,
Schwarzschild MA, Willett WC, Colditz GA,
Speizer FE, Acherio A Nonsteroidal antiinflammatorydrugs and the risk of
Parkinson’s
disease.
Arch
Neurol
60:1059–1064, 2003.
15. McGeer PL, McGeer EG Inflammation
and neurodegeneration in Parkinson’s
disease. Parkinsonism Relat Disord 10
(Suppl 1):S3–S7, 2004.
16. Warner TT, Schapira AHV Genetic and
environmental factors in the cause of
Parkinson’s disease. Ann Neurol 53:S16–
S25, 2003.
17. Marchetti B, Serra P-A, Tirolo C,
L’Episcopo F, Caniglia S, Gennuso F,
Testa N, Miele E, Desole MS, Barden N,
Morale MC Glucocorticoid receptor-nitric
oxide crosstalk and vulnerability to
experimental Parkinsonism: pivotal role for
38
glia-neuron interactions. Brain Res Rev
48:302–321, 2005.
18. Antonini A, Pezzoli G, Isaias IU,
Canesi M, Cilia R Long-term Efficacy of
Entacapone in Patients with Parkinson's
Disease and Motor Fluctuations - A SixYear Clinical Follow-Up Study. US
Neurological Disease, 2006.
19. Hagan, J. J., Middlemiss, D. N.,
Sharpe, P. C., and Poste, G. H.
Parkinson’s
disease:
prospects
for
improved
drug
therapy.
Trends
Pharmacol. Sci. 18:156–163,1997.
20. Tolosa, E., Mari, M. J., Vallldeoriola,
F., and Molinuevo, J. L. History of
levodopa and dopamine agonists in
Parkinson’s disease treatment. Neurology
50 (Suppl. 6):S2–S10, 1998
21. Olanow CW. The scientific basis for
the current treatment of Parkinson’s
disease. Ann Rev Med 2004; 55: 41–60.
22. Frankel JP, Lees AJ, Kempster PA,
Stern GM Subcutaneous apomorphine in
the treatment of Parkinson’s disease. J
Neurol Neurosurg Psychiatry 53:96-101,
1990.
23. Stocchi F et al. Apomorphine and
lisuride infusion: a comparative chronic
study. Adv Neurol 60:653-655, 1993.
24. Gancher ST, Nutt JC, Woodward WR
Apomorphine
infusional
therapy
in
Parkinson’s disease: clinical utility and
lack of tolerance. Mov Disord 10:37-43,
1995.
25. Pietz K et al. Subcutaneous
apomorphine in late stage Parkinson’s
disease: a long-term follow up. J Neurol
Neurosurg Psychiatry 65:709-716, 1998.
26. Reynolds GP, Elsworth JD, Blau K,
Sandier M, Lees A J, Stern GM Deprenyl
is metabolized to methamphetamine and
amphetamine in man. Br J Clin Pharmacol
12: 542- 544, 1978.
27. Lees A, on behalf of the Parkinson’s
Disease Research Group of the United
Kingdom. Comparison of therapeutic
effects and mortality data of levodopa and
levodopa combined with selegiline in
patients with early, mild Parkinson’s
disease. BMJ;311:1602-1607, 1995.
28. Benabid AL, Krack PP, Benazzouz A,
Limousin P, Koudsie A, Pollak P: Deep
brain stimulation of the subthalamic
nucleus
for
Parkinson’s
disease:
methodologic aspects and clinical criteria.
Neurology 2000; 55(suppl 6):S40–S44.
29. Laitinen LV, Bergenheim AT, Hariz MI:
Leksell’s posteroventral pallidotomy in the
treatment
ofParkinson’s
disease.
J
Neurosurg;76:53–61, 1992.
30. Hirsch, M. A., Toole, T., Maitland, C.
G., & Rider, R. A. The effects of balance
training and high-intensity resistance
training on persons with idiopathic
Parkinson’s disease. Archives of Physical
Medicine and Rehabilitation, 84, 1109–
1117,2003.
31. Miyai, I., Fujimoto, Y., Yamamoto, H.,
Ueda, Y., Saito, T., Nozaki, S., et al. Longterm effect of body weight-supported
treadmill training in Parkinson’s disease: A
randomized controlled trial. Archives of
Physical Medicine and Rehabilitation, 83,
1370–1373, 2002.
32. Crizzle, A. M., & Newhouse, I. J. Is
physical exercise beneficial for persons
with Parkinson’s disease. Clinical Journal
of Sport Medicine, 16, 422–425, 2006.
33. Ramig, L. O., Countryman, S.,
Thompson, L., & Horii, Y. A comparison of
two forms of intensive speech treatment
for Parkinson disease. Journal of Speech
and Hearing Research, 38, 1232–1251,
1995.
34. Dunnett S B & A Björklund Prospects
for new restorative and neuroprotective
treatments in Parkinson’s disease Nature
Vol 399, 1993.
35. von Campenhausen S, Bornschein B,
Wick R, Botzel K, Sampaio C, Poewe W,
Oertel W, Siebert U, Berger K,Dodel R
Prevalence and incidence of Parkinson’s
disease
in
Europe.
Eur
Neuropsychopharmacol
15:473–490,
2005.
36. Alves G, Forsaa EB, Pedersen KF,
Dreetz
Gjerstad
M,
Larsen
JP.
Epidemiology of Parkinson's disease. J
Neurol. Sep;255:18-32, 2008.
37. Meara J, Bhowmick BK, Hobson P
Accuracy of diagnosis in patients with
presumed Parkinson’s disease. Age
Ageing 28:99–102, 1999.
38. Van Den Eeden SK, Tanner
CM,Bernstein AL, Fross RD, Leimpeter A,
Bloch DA, Nelson LM Incidence of
Parkinson’s disease: variation by age,
gender, and race/ethnicity. Am J
Epidemiol 157:1015–1022, 2003.
2
39. Fahn S Description of Parkinson’s
disease as a clinical syndrome. Ann N Y
Acad Sci 991:1–14, 2003.
40. Twelves D, Perkins KS, Counsell C
Systematic review of incidence studies of
Parkinson’s disease. Mov Disord 18:19–
31, 2003.
41. Leentjens AFG, Van den Akker M,
Metsemakersc JFM, Troost J The
Incidence of Parkinson’s Disease in the
Netherlands: Results from a Longitudinal
General
Practice-Based
Registration
Neuroepidemiology; 22:311–312, 2003.
42. Lamberts H, Wood M: International
Classification of Primary Care. Oxford,
Oxford University Press, 1987.
43. Classification Committee of the
WONCA: ICHPPC-2-Defined International
Classification of Health Problems in
Primary Care. Oxford, Oxford University
Press, 1983.
44. Stephen K. Van Den Eeden1, Caroline
M. Tanner2, Allan L. Bernstein3, Robin D.
Fross4, Amethyst Leimpeter1, Daniel A.
Bloch5, and Lorene M. Nelson5Incidence
of Parkinson’s Disease: Variation by Age,
Gender,
and
Race/EthnicityAmerican
Journal of EpidemiologyVol. 157, No. 11,
2002.
45. N.U. Okubadejo, J.H. Bower, W.A.
Rocca and D.M. Maraganore, Parkinson's
disease in Africa: a systematic review of
epidemiologic
and
genetic
studies,
Movement Disord 21 , pp. 2150–2156,
2006.
46. P.P. Ashok, K. Radhakrishnan, R.
Sridharan and M.E. Mousa, Epidemiology
of Parkinson's disease in Benghazi, NorthEast Libya, Clin Neurol Neurosurg 88 , pp.
109–113, 1986.
47. Tekle-Haimanot R, Abebe M, GebreMariam A et al. Community-based study of
neurological disorders in rural central
Ethiopia. Neuroepidemiology; 9: 263–77,
1990.
48.
Osuntokun
BO,
Adeuja
AO,
Schoenberg
BS
et
al.Neurological
disorders in Nigerian Africans: a
community based study. Acta Neurol
Scand; 75: 13–21, 1987.
49. Harries J. L-dopa in the treatment of
Parkinsonismin Africans. East Afr Med J;
49: 112–5, 1972.
50. Bower JH, Teshome M, Melaku Z,
Zenebe G. Frequency of movement
disorders in an Ethiopian University
Practice. Mov Disord 2005; 20: 1209–13.
51. Cosnett JE, Bill PL. Parkinson’s
disease
in
blacks.Observations
on
epidemiology in Natal. S Afr Med J; 73:
281–3, 1988.
52. Dotchin CL, Msuya O, Walker RWO.
The challenge of Parkinson’s disease
management in Africa Age and Ageing;
36: 122–127, 2007.
53. Tanner CM, Ottman R, Goldman SM,
Ellenberg J, Chan P, Mayeux R et al.
Parkinson disease in twins: an etiologic
study. JAMA 281:341–366, 1999.
54. Zhang Y, Gao J, Chung KK, Huang H,
Dawson VL, Dawson TM. Parkin functions
as an E2-dependent ubiquitin- protein
ligase and promotes the degradation of
the synaptic vesicle-associated protein,
CDCrel-1. Proc Natl Acad Sci USA
97:13354–13359, 2000.
55. Staropoli JF, McDermott C, Martinat C,
Schulman B, Demireva E, Abeliovich A.
Parkin is a component of an SCF-like
ubiquitin ligase complex and protects
postmitotic
neurons
from
kainate
excitotoxicity. Neuron 37:735–749, 2003.
56. Davis GC, Williams AC, Markey SP,
Ebert MH, Caine ED, Reichert CM et al.
Chronic Parkinsonism secondary to
intravenous injection of meperidine
analogues. Psychiatry Res 1:249– 254,
1979.
57. Mena I, Court J, Fuenzalida S,
Papavasiliou PS, Cotzias GC. Modification
of
chronic
manganese
poisoning.
Treatment
with
L-dopa
or
5-OH
tryptophane. N Engl J Med 282:5–10,
1970.
58. Cook DG, Fahn S, Brait KA. Chronic
manganese intoxication. Arch Neurol
30:59–64, 1974.
59. Huang CC, Chu NS, Lu CS, Wang JD,
Tsai JL, Tzeng JL et al. Chronic
manganese intoxication. Arch Neurol
46:1104–1106, 1989.
60. Tanner CM. Epidemiology of
Parkinson’s disease. Neurol Clin 10:317–
329, 1992.
61. McGeer PL, Yasojima K, McGeer EG.
Inflammation in Parkinson’s disease. Adv
Neurol 86:83–89, 2001.
62. Mogi M, Harada M, Riederer P,
Narabayashi H, Fujita K, Nagatsu T.
Tumor necrosis factor-alpha (TNF-alpha)
3
increases both in the brain and in the
cerebrospinal fluid from parkinsonian
patients. Neurosci Lett 165(1–2):208–210,
1994.
63 Thorsen P, Jensen I, Jeune B,
Ebbesen N, Arpi M, Bremmelgaard A, et
al. Few microorganisms associated with
bacterial vaginosis may constitute the
pathologic core: a populationbased
microbiologic study among 3596 pregnant
women. Am J Obstet Gynecol 178:580–
587, 1998.
64. Ling Z, Gayle DA, Ma SY, Lipton JW,
Tong CW, Hong JS, et al. In utero
bacterial endotoxin exposure causes loss
of tyrosine hydroxylase neurons in the
postnatal rat midbrain. Mov Disord
17(1):116–124, 2002.
65. Martyn CN, Osmond C. Parkinson’s
disease and the environment in early life. J
Neurol Sci 132:201–206, 1995.
66. Mattock C, Marmot M, Stern G. Could
Parkinson’s disease follow intra-uterine
influenza? A speculative hypothesis. J
Neurol Neurosurg Psychiatry 51(6):753–
756,1988.
67. Martyn CN. Infection in childhood and
neurological diseases in adult life. Br Med
Bull 53(1):24–39, 1997.
68. Poskanzer DC, Schwab RS. Cohort
analysis
of
Parkinson’s
syndrome:
evidence for a single etiology related to
subclinical infection about 1920. J Chronic
Dis 16:961–973,1963.
69. Takahashi M, Yamada T. A possible
role of influenza A virus infection for
Parkinson’s disease. Adv Neurol 86:91–
104, 2001.
70. Betemps EJ, Buncher CR. Birthplace
as a risk factor in motor neurone disease
and Parkinson’s disease. Int J Epidemiol
22(5):898–904, 1993.
71. Kurtzke JF, Goldberg ID. Parkinsonism
death rates by race, sex, and geography.
Neurology 38(10):1558–1561,1988.
72. Elliot P, Cuzick J, English D, Stern R.
Geographical
and
Environmental
Epidemiology: Methods for Small-Area
Studies. New York:Oxford University
Press, 1992.
73. Snyder SH, D’Amato RJ. 1985.
Predicting Parkinson’s disease. Nature
317(6034):198–199.
74. McCormack AL, Thiruchelvam M,
Manning-Bog AB, Thiffault C, Langston
JW, Cory-Slechta DA, et al. Environmental
risk factors and Parkinson’s disease:
selective
degeneration
of
nigral
dopaminergic neurons caused by the
herbicide
paraquat.
Neurobiol
Dis
10(2):119–127, 2002.
75. Betarbet R, Sherer TB, MacKenzie G,
Garcia-Osuna M, Panov AV, Greenamyre
JT.Chronic systemic pesticide exposure
reproduces features of Parkinson’s
disease. Nat Neurosci 3(12):1301–1306,
2000.
76. Manning-Bog AB, McCormack AL, Li
J, Uversky VN, Fink AL, Di Monte DA. The
herbicide paraquat causes up-regulation
and aggregation of alpha-synuclein in
mice: paraquat and alpha-synuclein. J Biol
Chem 277(3):1641–1644, 2002.
77. Uversky VN, Li J, Fink AL.
Trimethylamine-N-oxide-induced folding of
alpha-synuclein. FEBS Lett 509(1):31–35,
2000.
78. Thiruchelvam MJ, Richfield EK,
Goodman BM, Baggs RB, Cory- Slechta
DA. Developmental exposure to the
pesticides paraquat and maneb and the
Parkinson’s
disease
phenotype.
Neurotoxicology 23:621–633, 2002.
79.
Checkoway
H,
Nelson
LM.
Epidemiologic approaches to the study of
Parkinson’s
disease
etiology.
Epidemiology 10:327–336, 1999.
80. Petrovitch H, Ross GW, Abbott RD,
Sanderson WT, Sharp DS, Tanner CM, et
al. Plantation work and risk of Parkinson
disease in a population-based longitudinal
study. Arch Neurol 59(11):1787–1792,
2002.
81.
Bernheimer,
H.,
Birkmayer,W.,
Hornykiewicz, O., Jellinger, K. &
Seitelberger, F. Brain dopamine and the
syndromes of Parkinson and Huntington.
Clinical, morphological and neurochemical
correlations. J. Neurol. Sci. 20, 415–455
1973.
82. Fearnley, J. & Lees, A. J. Parkinson’s
disease: neuropathology. Brain 114,
2283–2301, 1991.
83. McGeer, P. L., Itagaki, S., Akiyama, H.
& McGeer, E. G. Rate of cell death in
parkinsonism
indicates
active
neuropathological process. Ann. Neurol.
24, 574–576, 1989.
4
84. Calne, D. B. & Langston, J. W.
Aetiology of Parkinson’s disease. Lancet
2, 1457–1459, 1983).
85. Brooks, D. J. The early diagnosis of
Parkinson’s disease. Ann. Neurol. (suppl.)
44, S10–S18,1998.
86. Olanow, C. W., Jenner, P. & Beal, M.
F. Cell death and neuroprotection in
Parkinson’s disease. Ann. Neurol. (suppl.)
44, S1–S196, 1998.
87. Z.I. Alam, A. Jenner, S.E. Daniel, A.J.
Lees, N. Cairns, C.D. Marsden, P. Jenner,
B. Halliwell, Oxidative DNA damage in the
parkinsonian brain: an apparent selective
increase in 8-hydroxyguanine levels in
substantia nigra, J. Neurochem. 69 1196–
1203, 1997.
88. D.T. Dexter, A.E. Holley, W.D. Flitter,
T.F. Slater, F.R. Wells, S.E. Daniel, A.J.
Lees, P. Jenner, C.D. Marsden, Increased
levels of lipid hydroperoxides in the
parkinsonian substantia nigra: an HPLC
and ESR study, Mov. Disord. 9 92–97,
1994.
89. D.T. Dexter, J. Sian, S. Rose, J.G.
Hindmarsh, V.M. Mann, J.M. Cooper,
F.R.Wells, S.E. Daniel, A.J. Lees, A.H.
Schapira, et al., Indices of oxidative stress
and mitochondrial function in individuals
with incidental Lewy body disease, Ann.
Neurol. 35 38–44, 1994.
90. T.G. Hastings, D.A. Lewis, M.J.
Zigmond, Reactive dopamine metabolites
and
neurotoxicity:
implications
for
Parkinson's disease, Adv. Exp. Med. Biol.
387 97–106, 1996.
91. D. Sulzer, L. Zecca, Intraneuronal
dopamine-quinone synthesis: a review,
Neurotox. Res. 1 181–195, 2000.
92. A.H. Schapira, J.M. Cooper, D. Dexter,
P. Jenner, J.B. Clark, C.D. Marsden,
Mitochondrial complex I deficiency in
Parkinson's disease, Lancet 1 1269. 1989.
93 R. Betarbet, T.B. Sherer, G.
MacKenzie, M. Garcia-Osuna, A.V. Panov,
J.T. Greenamyre, Chronic systemic
pesticide exposure reproduces features of
Parkinson's disease, Nat. Neurosci. 3
1301–1306. 2000.
94 J.W. Langston, P. Ballard, J.W. Tetrud,
I. Irwin, Chronic Parkinsonism in humans
due to a product of meperidine-analog
synthesis, Science 219 979–980. 1983.
95. J.W. Langston, L.S. Forno, C.S.
Rebert, I. Irwin, Selective nigral toxicity
after systemic administration of 1-methyl4-phenyl-1,2,5,6-tetrahydropyrine (MPTP)
in the squirrel monkey, Brain Res. 292
390–394. 1984.
96. G.F.Wooten, L.J. Currie, J.P. Bennett,
M.B. Harrison, J.M. Trugman, W.D. Parker
Jr., Maternal inheritance in Parkinson's
disease, Ann. Neurol. 41 265–268. 1997.
97 A.H. Schapira, Mitochondria in the
aetiology and pathogenesis of Parkinson's
disease, Lancet Neurol. 7 97–109. 2008.
98 I. Cantuti-Castelvetri, M.T. Lin, K.
Zheng, C.E. Keller-McGandy, R.A.
Betensky, D.R. Johns, M.F. Beal, D.G.
Standaert, D.K. Simon, Somatic
mitochondrial DNA mutations in single
neurons and glia, Neurobiol. Aging 26
1343–1355. 2005.
99. T.L. Perry, V.W. Yong, Idiopathic
Parkinson's disease, progressive
supranuclear palsy and glutathione
metabolism in the substantia nigra of
patients, Neurosci. Lett. 67 269–274,
1986..
100. J. Sian, D.T. Dexter, A.J. Lees, S.
Daniel, Y. Agid, F. Javoy-Agid, P. Jenner,
C.D. Marsden, Alterations in glutathione
levels in Parkinson's disease and other
neurodegenerative disorders affecting
basal ganglia, Ann. Neurol. 36 348–355,
1994.
101. E. Sofic, K.W. Lange, K. Jellinger, P.
Riederer,
Reduced
and
oxidized
glutathione in the substantia nigra of
patients
with
Parkinson's
disease,
Neurosci. Lett. 142 128–130, 1992
102. I.E. Clark, M.W. Dodson, C. Jiang,
J.H. Cao, J.R. Huh, J.H. Seol, S.J. Yoo,
B.A. Hay, M. Guo, Drosophila pink1 is
required for mitochondrial function and
interacts genetically with parkin, Nature
441 1162–1166. 2006.
103. R.H. Kim, P.D. Smith, H. Aleyasin, S.
Hayley, M.P. Mount, S. Pownall, A.
Wakeham, A.J. You-Ten, S.K. Kalia, P.
Horne, D. Westaway, A.M. Lozano, H.
Anisman,
D.S.
Park,
T.W.
Mak,
Hypersensitivity of DJ-1-deficient mice to
1-methyl-4-phenyl-1,2,3,6tetrahydropyrindine (MPTP) and oxidative
stress, Proc. Natl. Acad. Sci. U. S. A. 102
5215–5220. 2005.
104.J. Park, S.B. Lee, S. Lee, Y. Kim, S.
Song, S. Kim, E. Bae, J. Kim, M. Shong,
J.M. Kim, J. Chung, Mitochondrial
5
dysfunction in Drosophila PINK1 mutants
is complemented by parkin, Nature 441
1157–1161, 2006.
105. T. Yokota, K. Sugawara, K. Ito, R.
Takahashi, H. Ariga, H. Mizusawa, Down
regulation of DJ-1 enhances cell death by
oxidative
stress,
ER
stress,
and
proteasome inhibition, Biochem. Biophys.
Res. Commun. 312 1342–1348. 2003.
106. Yacoubian, T.A. and D.G. Standaert,
Targets for neuroprotection in Parkinson's
disease. Biochimica et Biophysica Acta
(BBA) - Molecular Basis of Disease,
1792(7): p. 676-687. 2009.
107. A. Athanassiadou, G. Voutsinas, L.
Psiouri, E. Leroy, M.H. Polymeropoulos, A.
Ilias, G.M. Maniatis, T. Papapetropoulos,
Genetic analysis of families with Parkinson
disease that carry the Ala53Thr mutation
in the gene encoding alpha-synuclein,
Am. J. Hum. Genet. 65 555–558. 1999.
108. R. Kruger, W. Kuhn, T. Muller, D.
Woitalla, M. Graeber, S. Kosel, H.
Przuntek, J.T. Epplen, L. Schols, O. Riess,
Ala30Pro mutation in the gene encoding
alphasynuclein in Parkinson's disease,
Nat. Genet. 18 106–108. 1998.
109. M.H. Polymeropoulos, C. Lavedan, E.
Leroy, S.E. Ide, A. Dehejia, A. Dutra, B.
Pike, H. Root, J. Rubenstein, R. Boyer,
E.S. Stenroos, S. Chandrasekharappa, A.
Athanassiadou, T. Papapetropoulos, W.G.
Johnson, A.M. Lazzarini, R.C. Duvoisin, G.
Di Iorio, L.I. Golbe, R.L. Nussbaum,
Mutation in the alpha-synuclein gene
identified in families with Parkinson's
disease, Science 276 (1997) 2045–2047.
110. J.J. Zarranz, J. Alegre, J.C. GomezEsteban, E. Lezcano, R. Ros, I. Ampuero,
L. Vidal, J. Hoenicka, O. Rodriguez, B.
Atares, V. Llorens, E. Gomez Tortosa, T.
del Ser, D.G. Munoz, J.G. de Yebenes,
The new mutation, E46K, of alphasynuclein causes Parkinson and Lewy
body dementia, Ann. Neurol. 55 (2004)
164–173.
111. M.C. Irizarry,W. Growdon, T. GomezIsla, K. Newell, J.M. George, D.F. Clayton,
B.T.. Hyman, Nigral and cortical Lewy
bodies and dystrophic nigral neurites in
Parkinson's disease and cortical Lewy
body disease contain alpha-synuclein
immunoreactivity, J. Neuropathol. Exp.
Neurol. 57 (1998) 334–337.
112.A.B. Singleton, M. Farrer, J. Johnson,
A. Singleton, S. Hague, J. Kachergus, M.
Hulihan, T. Peuralinna, A. Dutra, R.
Nussbaum, S. Lincoln, A. Crawley, M.
Hanson, D. Maraganore, C. Adler, M.R.
Cookson, M. Muenter, M. Baptista, D.
Miller, J. Blancato, J. Hardy, K. GwinnHardy, alpha-Synuclein locus triplication
causes Parkinson's disease, Science 302
(2003) 841.
113. K.A. Conway, S.J. Lee, J.C. Rochet,
T.T. Ding, R.E. Williamson, P.T. Lansbury
Jr., Acceleration of oligomerization, not
fibrillization, is a shared property of both
alpha-synuclein mutations linked to earlyonset Parkinson's disease: implications
for pathogenesis and therapy, Proc. Natl.
Acad. Sci. U. S. A. 97 (2000)
571–576. 114. E. Masliah, E. Rockenstein,
I. Veinbergs, M. Mallory, M. Hashimoto, A.
Takeda, Y. Sagara, A. Sisk, L. Mucke,
Dopaminergic loss and inclusion body
formation
in
alpha-synuclein
mice:
implications
for
neurodegenerative
disorders, Science 287 (2000) 1265–1269.
115. J.M. Souza, B.I. Giasson, Q. Chen,
V.M. Lee, H. Ischiropoulos, Dityrosine
crosslinking promotes formation of stable
alpha-synuclein polymers. Implication of
nitrative and oxidative stress in the
pathogenesis of neurodegenerative
synucleinopathies, J. Biol. Chem. 275
18344–18349, 2000.
116. A. Abeliovich, Y. Schmitz, I. Farinas,
D. Choi-Lundberg, W.H. Ho, P.E. Castillo,
N. Shinsky, J.M. Verdugo, M. Armanini, A.
Ryan, M. Hynes, H. Phillips, D. Sulzer, A.
Rosenthal, Mice lacking alpha-synuclein
display functional deficits in the
nigrostriatal dopamine system, Neuron 25
239–252, 2000.
117. D.D. Murphy, S.M. Rueter, J.Q.
Trojanowski, V.M. Lee, Synucleins are
developmentally expressed, and alphasynuclein regulates the size of the
presynaptic vesicular pool in primary
hippocampal neurons, J. Neurosci. 20
3214–3220, 2000.
118. T.R. Flower, L.S. Chesnokova, C.A.
Froelich, C. Dixon, S.N. Witt, Heat shock
prevents
alpha-synuclein-induced
apoptosis in a yeast model of Parkinson's
disease, J. Mol. Biol. 351 1081–1100,
2005.
6
119. A.R. Saha, N.N. Ninkina, D.P.
Hanger, B.H. Anderton, A.M. Davies, V.L.
Buchman, Induction of neuronal death by
alpha-synuclein, Eur. J. Neurosci. 12
3073–3077, 2000.
120. E. Leroy, R. Boyer, G. Auburger, B.
Leube, G. Ulm, E. Mezey, G. Harta, M.J.
Brownstein, S. Jonnalagada, T. Chernova,
A. Dehejia, C. Lavedan, T. Gasser, P.J.
Steinbach,
K.D.
Wilkinson,
M.H.
Polymeropoulos, The ubiquitin pathway in
Parkinson's disease, Nature 395 451–452,
1998.
121. T. Kitada, S. Asakawa, N. Hattori, H.
Matsumine, Y. Yamamura, S. Minoshima,
M. Yokochi, Y. Mizuno, N. Shimizu,
Mutations in the parkin gene cause
autosomal
recessive
juvenile
parkinsonism, Nature 392 605–608, 1998.
122. Y. Imai, M. Soda, R. Takahashi,
Parkin suppresses unfolded protein stressinduced cell death through its E3
ubiquitin–protein ligase activity, J. Biol.
Chem. 275 35661–35664, 2000.
123. K.K. Chung, Y. Zhang, K.L. Lim, Y.
Tanaka, H. Huang, J. Gao, C.A. Ross,
V.L. Dawson, T.M. Dawson, Parkin
ubiquitinates
the
alpha-synucleininteracting
protein,
synphilin-1:
implications for Lewy-body formation in
Parkinson disease, Nat. Med. 7 1144–
1150, 2001.
124. H. Mori, T. Kondo, M. Yokochi, H.
Matsumine, Y. Nakagawa-Hattori, T.
Miyake, K. Suda, Y. Mizuno, Pathologic
and biochemical studies of juvenile
parkinsonism linked to chromosome 6q,
Neurology 51 890–892,1998.
125. K.S. McNaught, C. Mytilineou, R.
Jnobaptiste, J. Yabut, P. Shashidharan, P.
Jennert, C.W. Olanow, Impairment of the
ubiquitin–proteasome
system
causes
dopaminergi cell death and inclusion body
formation in ventral mesencephalic
cultures, J. Neurochem. 81 301–306,
2002.
126. J. Klucken, Y. Shin, E. Masliah, B.T.
Hyman, P.J. McLean, Hsp70 reduces
alphasynuclein aggregation and toxicity, J.
Biol. Chem. 279 25497–25502, 2004.
127. M.G. Tansey, M.K. McCoy, T.C.
Frank-Cannon,
Neuroinflammatory
mechanisms in Parkinson's disease:
potential
environmental
triggers,
pathways, and targets for early therapeutic
intervention, Exp. Neurol. 208 1–25, 2007.
128. E. Esposito, V. Di Matteo, A.
Benigno, M. Pierucci, G. Crescimanno, G.
Di
Giovanni,
Non-steroidal
antiinflammatory drugs in Parkinson's disease,
Exp. Neurol. 205 295–312, 2007.
129. P.L. McGeer, S. Itagaki, B.E. Boyes,
E.G. McGeer, Reactive microglia are
positive for HLA-DR in the substantia nigra
of Parkinson's and Alzheimer's disease
brains, Neurology 38 1285–1291, 1988.
130. P.L. McGeer, C. Schwab, A. Parent,
D. Doudet, Presence of reactive microglia
in monkey substantia nigra years after 1methyl-4-phenyl-1,2,3,6-tetrahydropyridine
administration, Ann. Neurol. 54 599–604,
2003.
131. C.F. Orr, D.B. Rowe, Y. Mizuno, H.
Mori, G.M. Halliday, A possible role for
humoral immunity in the pathogenesis of
Parkinson's disease, Brain 128 2665–
2674, 2005.
132. M. Mogi, M. Harada, T. Kondo, P.
Riederer, H. Inagaki, M. Minami, T.
Nagatsu, Interleukin-1 beta, interleukin-6,
epidermal growth factor and transforming
growth factor-alpha are elevated in the
brain
from
parkinsonian
patients,
Neurosci. Lett. 180 147–150, 1994.
133 W. Zhang, T.Wang, Z. Pei, D.S.Miller,
X.Wu,M.L. Block, B.Wilson, Y. Zhou,
J.S.Hong, J. Zhang, Aggregated alphasynuclein activates microglia: a process
leading to disease progression in
Parkinson's disease, FASEB J. 19 533–
542, 2005.
134. A.D. Reynolds, J.G. Glanzer, I.
Kadiu, M. Ricardo-Dukelow, A. Chaudhuri,
P. Ciborowski, R. Cerny, B. Gelman, M.P.
Thomas, R.L. Mosley, H.E. Gendelman,
Nitrated
alpha-synuclein-activated
microglial profiling for Parkinson's disease,
J. Neurochem. 104 1504–1525, 2008.
135. A.D. Reynolds, I. Kadiu, S.K. Garg,
J.G. Glanzer, T. Nordgren, P. Ciborowski,
R. Banerjee, H.E. Gendelman, Nitrated
alpha-synuclein
and
microglial
neuroregulatory
activities,
J.
Neuroimmune. Pharmacol. 3 59–74, 2008.
136. E.J. Benner, R. Banerjee, A.D.
Reynolds, S. Sherman, V.M. Pisarev, V.
Tsiperson, C. Nemachek, P. Ciborowski,
S. Przedborski, R.L. Mosley, H.E.
Gendelman,
Nitrated
alpha-synuclein
7
immunity accelerates degeneration of
nigral dopaminergic neurons, PLoS ONE 3
e1376, 2008.
137. S. Theodore, S. Cao, P.J. McLean,
D.G. Standaert, Targeted overexpression
of
human
alpha-synuclein
triggers
microglial activation and an adaptive
immune response in a mouse model of
Parkinson disease, J. Neuropathol. Exp.
Neurol. 67. 2007.
138. A. Ghosh, A. Roy, X. Liu, J.H.
Kordower, E.J. Mufson, D.M. Hartley, S.
Ghosh, R.L. Mosley, H.E. Gendelman, K.
Pahan, Selective inhibition of NF-kappaB
activation prevents dopaminergic neuronal
loss in a mouse model of Parkinson's
disease, Proc. Natl. Acad. Sci. U. S. A.
104 18754–18759, 2007.
139. J.H. Bower, D.M. Maraganore, B.J.
Peterson, J.E. Ahlskog,W.A. Rocca,
Immunologic diseases, anti-inflammatory
drugs, and Parkinson disease: a casecontrol study, Neurology 67 494–496,
2006.
140. H. Chen, E. Jacobs, M.A.
Schwarzschild, M.L. McCullough, E.E.
Calle,
M.J.
Thun,
A.
Ascherio,
Nonsteroidal antiinflammatory drug use
and the risk for Parkinson's disease, Ann.
Neurol. 58 963–967, 2005.
141. H. Chen, S.M. Zhang, M.A. Hernan,
M.A. Schwarzschild,W.C. Willett, G.A.
Colditz, F.E. Speizer, A. Ascherio,
Nonsteroidal anti-inflammatory drugs and
the risk of Parkinson disease, Arch.
Neurol. 60 1059–1064, 2003.
142. A randomized, double-blind, futility
clinical trial of creatine and minocycline in
early Parkinson disease, Neurology 66
664–671, 2006.
143. I. Mody, J.F. MacDonald, NMDA
receptor-dependent excitotoxicity: the role
of intracellular Ca2+ release, Trends
Pharmacol. Sci. 16 356–359, 1995.
144. V.L. Dawson, T.M. Dawson, Nitric
oxide neurotoxicity, J. Chem. Neuroanat.
10 179–190, 1996.
145. L. Turski, K. Bressler, K.J. Rettig,
P.A. Loschmann, H. Wachtel, Protection of
substantia nigra from MPP+ neurotoxicity
by N-methyl-D-aspartate antagonists,
Nature 349 414–418, 1991.
146. E. Brouillet, M.F. Beal, NMDA
antagonists partially protect against MPTP
induced neurotoxicity in mice, Neuroreport
4 387–390, 1993.
147. J. Jankovic, C. Hunter, A doubleblind, placebo-controlled and longitudinal
study of riluzole in early Parkinson's
disease, Parkinsonism Relat. Disord. 8
271–276, 2002
148. J. Kornhuber, M. Weller, K.
Schoppmeyer, P. Riederer, Amantadine
and memantine are NMDA receptor
antagonists
with
neuroprotective
properties, J. Neural. Transm. (Suppl. 43)
91–104, 1994.
149. T.J. Counihan, G.B. Landwehrmeyer,
D.G. Standaert, C.M. Kosinski, C.R.
Scherzer, L.P. Daggett, G. Velicelebi, A.B.
Young, J.B. Penney Jr., Expression of Nmethyl-Daspartate receptor subunit mRNA
in the human brain: mesencephalic
dopaminergic neurons, J. Comp. Neurol.
390 91–101, 1998.
150. P. Anglade, S. Vyas, F. Javoy-Agid,
M.T. Herrero, P.P. Michel, J. Marquez, A.
Mouatt- Prigent, M. Ruberg, E.C. Hirsch,
Y. Agid, Apoptosis and autophagy in nigral
neurons of patients with Parkinson's
disease, Histol. Histopathol. 12
25–31, 1997.
151. M.M. Tompkins, E.J. Basgall, E.
Zamrini, W.D. Hill, Apoptotic-like changes
in Lewy-body-associated disorders and
normal aging in substantia nigral neurons,
Am. J. Pathol. 150 119–131, 1997.
152. E.C. Hirsch, S. Hunot, B. Faucheux,
Y. Agid, Y. Mizuno, H. Mochizuki, W.G.
Tatton, N. Tatton, W.C. Olanow,
Dopaminergic neurons degenerate by
apoptosis in Parkinson's disease, Mov.
Disord. 14 383–385, 1999.
153. Sun,Xin; Huang,Luqi; Zhang,Min;
Sun,Shenggang; Wu,Yan, Insulin like
growth factor-1 prevents 1-mentyl-4phenylphyridinium-induced apoptosis in
PC12 cells through activation of glycogen
synthase kinase-3beta, Toxicology, 271,
1-2, 5-12, 2010.
154. M.P. Mattson, Neuronal life-anddeath
signaling,
apoptosis,
and
neurodegenerative disorders, Antioxid.
Redox Signal. 8 1997–2006, 2006.
155. D.W. Howells, M.J. Porritt, J.Y.
Wong, P.E. Batchelor, R. Kalnins, A.J.
Hughes, G.A. Donnan, Reduced BDNF
mRNA expression in the Parkinson's
8
disease substantia nigra, Exp. Neurol. 166
127–135, 2000.
156. N.B. Chauhan, G.J. Siegel, J.M. Lee,
Depletion of glial cell line-derived
neurotrophic factor in substantia nigra
neurons of Parkinson's disease brain, J.
Chem. Neuroanat. 21 277–288, 2001.
157. M. Mogi, A. Togari, T. Kondo, Y.
Mizuno, O. Komure, S. Kuno, H. Ichinose,
T. Nagatsu, Brain-derived growth factor
and nerve growth factor concentrations
are decreased in the substantia nigra in
Parkinson's disease, Neurosci. Lett. 270
45–48, 1999.
158. Dauer, W. ] Neurotrophic Factors and
Parkinson’s Disease: The Emergence of a
New Player? Sci. STKE, 6 November Vol.
2007, Issue 411, p. pe60, 2007.
159. Lindholm P, Voutilainen MH, Laure´n
J, Pera¨nen J, Leppa¨nen VM, Andressoo
JO, Lindahl M, Janhunen S, Kalkkinen N,
Timmusk T, Tuominen RK, Saarma M
Novel neurotrophic factor CDNF protects
and rescues midbrain dopamine neurons
in vivo. Nature 448:73–77, 2007.
160. Nutt JG, Burchiel KJ, Comella CL,
Jankovic J, Lang AE, Laws ER Jr, Lozano
AM, Penn RD, Simpson RK Jr, Stacy M,
Wooten GF; ICV GDNF Study Group.
Implanted intracerebroventricular. Glial cell
line-derived
neurotrophic
factor
Randomized, double-blind trial of glial cell
linederived neurotrophic factor (GDNF) in
PD. Neurology 60:69 –73, 2003.
161. Hamilton JF, Morrison PF, Chen MY,
Harvey-White J, Pernaute RS, Phillips H,
Oldfield E, Bankiewicz KS Heparin
coinfusion during convection-enhanced
delivery (CED) increases the distribution of
the glial-derived neurotrophic factor
(GDNF) ligand family in rat striatum and
enhances the pharmacological activity of
neurturin. Exp Neurol 168:155–161, 2001.
162. Salvatore MF, Ai Y, Fischer B, Zhang
AM, Grondin RC, Zhang Z, Gerhardt GA,
GashDM Point source concentration of
GDNF may explain failure of phase II
clinical trial. Exp Neurol 202:497–505,
2006.
163. Petrova P, Raibekas A, Pevsner J,
Vigo N, Anafi M, Moore MK, Peaire AE,
Shridhar V, Smith DI, Kelly J, Durocher Y,
Commissiong
JW
MANF:
a new
mesencephalic
astrocyte-derived
neurotrophic factor with selectivity for
dopaminergic neurons. J Mol Neurosci
20:173–188, 2003.
164. Apostolou A, Shen Y, Liang Y, Luo J,
Fang S Armet, a UPRupregulated protein,
inhibits cell proliferation and ER stressinduced cell death. Exp Cell Res 314:2454
–2467, 2008.
165. Merja H. Voutilainen, Susanne Bäck,
Eeva Pörsti, Liisa Toppinen, Lauri
Lindgren, Päivi Lindholm, Johan Peränen,
Mart Saarma, and Raimo K. Tuominen
Mesencephalic
Astrocyte-Derived
Neurotrophic Factor Is Neurorestorative in
Rat Model of Parkinson's Disease
J. Neurosci. 29: 9651-9659;
166. B.M. Ravina, S.C. Fagan, R.G. Hart,
C.A. Hovinga, D.D. Murphy, T.M. Dawson,
J.R. Marler, Neuroprotective agents for
clinical trials in Parkinson's disease: a
systematic assessment, Neurology 60
1234–1240, 2003.
167. G.W. Ross, R.D. Abbott, H.
Petrovitch, D.M. Morens, A. Grandinetti,
K.H. Tung, C.M.Tanner, K.H. Masaki, P.L.
Blanchette, J.D. Curb, J.S. Popper, L.R.
White, Association of coffee and caffeine
intake with the risk of Parkinson disease,
JAMA 283 2674–2679, 2000.
168. A. Ascherio, S.M. Zhang, M.A.
Hernan, I. Kawachi, G.A. Colditz, F.E.
Speizer, W.C. Willett, Prospective study of
caffeine consumption and risk of
Parkinson's disease in men and women,
Ann. Neurol. 50 56–63, 2001.
169. S. Ferre, K. Fuxe, Dopamine
denervation leads to an increase in the
intramembrane
interaction
between
adenosine A2 and dopamine D2 receptors
in the neostriatum, Brain Res. 594 124–
130, 1992.
170. S. Ferre, W.T. O'Connor, K. Fuxe, U.
Ungerstedt, The striopallidal neuron: a
main locus for adenosine–dopamine
interactions in the brain, J. Neurosci. 13
5402–5406, 1993.
171. W. Bara-Jimenez, A. Sherzai, T.
Dimitrova, A. Favit, F. Bibbiani, M.
Gillespie, M.J. Morris, M.M. Mouradian,
T.N. Chase, Adenosine A(2A) receptor
antagonist treatment of Parkinson's
disease, Neurology 61 293–296, 2003.
172. R.A. Hauser, J.P. Hubble, D.D.
Truong, Randomized trial of the adenosine
A(2A) receptor antagonist istradefylline in
9
advanced PD, Neurology 61 297–303,
2003.
173. J.F. Chen, K. Xu, J.P. Petzer, R.
Staal, Y.H. Xu, M. Beilstein, P.K. Sonsalla,
K. Castagnoli, N. Castagnoli Jr., M.A.
Schwarzschild,
Neuroprotection
by
caffeine and A(2A) adenosine receptor
inactivation in a model of Parkinson's
disease, J. Neurosci. 21 RC143, 2001.
174. K. Ikeda, M. Kurokawa, S. Aoyama,
Y. Kuwana, Neuroprotection by adenosine
A2A receptor blockade in experimental
models of Parkinson's disease, J.
Neurochem. 80 262–270, 2002.
175. M.G. Tansey, M.K. McCoy, T.C.
Frank-Cannon,
Neuroinflammatory
mechanisms in Parkinson's disease:
potential
environmental
triggers,
pathways, and targets for early therapeutic
intervention, Exp. Neurol. 208 1–25, 2007.
176. E. Esposito, V. Di Matteo, A.
Benigno, M. Pierucci, G. Crescimanno, G.
Di
Giovanni,
Non-steroidal
antiinflammatory drugs in Parkinson's disease,
Exp. Neurol. 205 295–312, 2007.
177. E.G. McGeer, P.L. McGeer, The role
of anti-inflammatory agents in Parkinson's
disease, CNS Drugs 21 789–797, 2007.
178. H. Chen, S.M. Zhang, M.A. Hernan,
M.A. Schwarzschild,W.C. Willett, G.A.
Colditz, F.E. Speizer, A. Ascherio,
Nonsteroidal anti-inflammatory drugs and
the risk of Parkinson disease, Arch.
Neurol. 60 1059–1064, 2003.
179. J.H. Bower, D.M. Maraganore, B.J.
Peterson, J.E. Ahlskog,W.A. Rocca,
Immunologic diseases, anti-inflammatory
drugs, and Parkinson disease: a casecontrol study, Neurology 67 494–496,
2006.
180. M.A. Hernan, G. Logroscino, L.A.
Garcia Rodriguez, Nonsteroidal antiinflammatory drugs and the incidence of
Parkinson disease, Neurology 66 1097–
1099, 2006.
181. P. Di Napoli, A.A. Taccardi, M. Oliver,
R. De Caterina, Statins and stroke:
evidence
for
cholesterol-independent
effects, Eur. Heart J. 23 1908–1921, 2002.
182. T.G. Ton, S.R. Heckbert, W.T.
Longstreth Jr., M.A. Rossing, W.A. Kukull,
G.M. Franklin, P.D. Swanson, T. SmithWeller, H. Checkoway, Nonsteroidal
antiinflammatory drugs and risk of
Parkinson's disease, Mov. Disord. 21 964–
969, 2006.
183. M.L. Selley, Simvastatin prevents 1methyl-4-phenyl-1,2,3,6
tetrahydropyridineinduced
striatal
dopamine depletion and protein tyrosine
nitration in mice, Brain Res. 1037 1–6,
2005.
184. T. Tikka, B.L. Fiebich, G. Goldsteins,
R. Keinanen, J. Koistinaho, Minocycline, a
tetracycline derivative, is neuroprotective
against
excitotoxicity
by
inhibiting
activation and proliferation of microglia, J.
Neurosci. 21 2580–2588, 2001.
185. T.M. Tikka, J.E. Koistinaho,
Minocycline
provides
neuroprotection
against Nmethyl- D-aspartate neurotoxicity
by inhibiting microglia, J. Immunol.166
(2001) 7527–7533.
186. Y. Du, Z. Ma, S. Lin, R.C. Dodel, F.
Gao, K.R. Bales, L.C. Triarhou, E.
Chernet, K.W. Perry, D.L. Nelson, S.
Luecke, L.A. Phebus, F.P. Bymaster, S.M.
Paul, Minocycline prevents nigrostriatal
dopaminergic neurodegeneration in the
MPTP model of Parkinson's disease, Proc.
Natl. Acad. Sci. U. S. A. 98 14669–14674,
2001.
187. A.F. Haywood, B.E. Staveley, Parkin
counteracts symptoms in a Drosophila
model of Parkinson's disease, BMC
Neurosci. 5 14, 2004.
188. M.G. Spillantini, M.L. Schmidt, V.M.
Lee, J.Q. Trojanowski, R. Jakes, M.
Goedert, Alpha-synuclein in Lewy bodies,
Nature 388 839–840, 1997.
189. J. Klucken, Y. Shin, E. Masliah, B.T.
Hyman, P.J. McLean, Hsp70 reduces
alphasynuclein aggregation and toxicity, J.
Biol. Chem. 279 25497–25502, 2004.
190.J.M. Souza, B.I. Giasson, Q. Chen,
V.M. Lee, H. Ischiropoulos, Dityrosine
crosslinking promotes formation of stable
alpha-synuclein polymers. Implication of
nitrative and oxidative stress in the
pathogenesis of neurodegenerative
synucleinopathies, J. Biol. Chem. 275
18344–18349, 2000.
191. L. Chen, M.B. Feany, Alphasynuclein
phosphorylation
controls
neurotoxicity and inclusion formation in a
Drosophila model of Parkinson disease,
Nat. Neurosci. 8 657–663, 2005.
192. A.M. Bodles, O.M. El-Agnaf, B.
Greer, D.J. Guthrie, G.B. Irvine, Inhibition
10
of fibril formation and toxicity of a fragment
of alpha-synuclein by an N-methylated
peptide analogue, Neurosci. Lett. 359 89–
93, 2004.
193 D.A. Amer, G.B. Irvine, O.M. El-Agnaf,
Inhibitors
of
alpha-synuclein
oligomerization and toxicity: a future
therapeutic strategy for Parkinson's
disease and related disorders, Exp. Brain
Res. 173 223–233, 2006.
194, H. Deng, W. Le, Y. Guo, C.B. Hunter,
W. Xie, J. Jankovic, Genetic and clinical
identification of Parkinson's disease
patients with LRRK2 G2019S mutation,
Ann. Neurol. 57 933–934, 2005.
195, W.P. Gilks, P.M. Abou-Sleiman, S.
Gandhi, S. Jain, A. Singleton, A.J. Lees,
K. Shaw, K.P. Bhatia, V. Bonifati, N.P.
Quinn, J. Lynch, D.G. Healy, J.L. Holton,
T. Revesz, N.W. Wood, A common
LRRK2 mutation in idiopathic Parkinson's
disease, Lancet 365 415–416, 2005.
196. A.B. West, D.J. Moore, S. Biskup, A.
Bugayenko, W.W. Smith, C.A. Ross, V.L.
Dawson, T.M. Dawson, Parkinson's
disease-associated mutations in leucinerich repeat kinase 2 augment kinase
activity, Proc. Natl. Acad. Sci. U. S. A. 102
16842–16847, 2005.
197. Guan, J., Krishnamurthi, R.,
Waldvogel, H.J., Faull, R.L., Clark, R.,
Gluckman, P., . N-terminal tripeptide of
IGF-1 (GPE) prevents the loss of TH
positive neurons after 6-OHDA induced
nigral lesion in rats. Brain Res. 859, 286–
292, 2000.
198. Lin, L.F., Doherty, D.H., Lile, J.D.,
Bektesh, S., Collins, F., GDNF: a glial cell
line-derived
neurotrophic
factor
for
midbrain dopaminergic neurons. Science
260, 1130–1132, 1993.
199. B.N. Ames, R. Cathcart, E. Schwiers,
P. Hochstein, Uric acid provides an
antioxidant defense in humans against
oxidant- and radical-caused aging and
cancer: a hypothesis, Proc. Natl. Acad.
Sci. U. S. A. 78 6858–6862, 1981.
J.W. Davis, A. Grandinetti, C.I. Waslien,
200. G.W. Ross, L.R. White, D.M. Morens,
Observations on serum uric acid levels
and the risk of idiopathic Parkinson's
disease, Am. J. Epidemiol. 144 480–484,
1996.
201. M.G. Weisskopf, E. O'Reilly, H. Chen,
M.A. Schwarzschild, A. Ascherio, Plasma
urate and risk of Parkinson's disease, Am.
J. Epidemiol. 166 561–567, 2007.
202. M.A. Schwarzschild, S.R. Schwid,
K.Marek, A.Watts, A.E. Lang, D. Oakes, I.
Shoulson, A. Ascherio, C. Hyson, E.
Gorbold, A. Rudolph, K. Kieburtz, S. Fahn,
L. Gauger, C. Goetz, J. Seibyl, M. Forrest,
J. Ondrasik, Serum urate as a predictor of
clinical and radiographic progression in
Parkinson disease, Arch. Neurol. 65 716–
723, 2008.
203. W. Duan, B. Ladenheim, R.G. Cutler,
I.I. Kruman, J.L. Cadet, M.P. Mattson,
Dietary folate deficiency and elevated
homocysteine
levels
endanger
dopaminergic neurons in models of
Parkinson's disease, J. Neurochem. 80
101–110, 2002.
204. X. Gao, H. Chen, H.K. Choi, G.
Curhan, M.A. Schwarzschild, A. Ascherio,
Diet, urate, and Parkinson's disease risk in
men, Am. J. Epidemiol. 167 831–838,
2008.
205. Ritz B, Ascherio A, Checkoway H,
Marder KS, Nelson LM, Rocca WA, et al.
Pooled analysis of tobacco use and risk of
Parkinson disease. Arch Neurol;64:990–7,
2007.
206. O’Reilly EJ, McCullough ML, Chao A,
Henley SJ, Calle EE, Thun MJ, et al.
Smokeless tobacco use and the risk of
Parkinson’s disease mortality. Mov
Disord;20:1383–4, 2005.
207. Allam MF, Campbell MJ, Hofman A,
Del Castillo AS, Fernandez-Crehuet
Navajas R. Smoking and Parkinson’s
disease: systematic review of prospective
studies. Mov Disord;19:614–21, 2004.
208. Tanner CM, Goldman SM, Aston DA,
Ottman R, Ellenberg J, Mayeux R, et al.
Smoking and Parkinson’s disease in twins.
Neurology;58:581–8, 2002.
209. Ross GW, Petrovitch H. Current
evidence for neuroprotective effects of
nicotine and caffeine against Parkinson’s
disease. Drugs Aging;18: 797–806, 2001.
210. Hernan MA, Zhang SM, RuedadeCastro AM, Colditz GA, Speizer FE,
Ascherio A. Cigarette smoking and the
incidence of Parkinson’s disease in two
prospective studies. Ann Neurol;50:780–6,
2001.
211. Gorell JM, Rybicki BA, Johnson CC,
Peterson EL. Smoking and Parkinson’s
11
disease: a dose-response relationship.
Neurology;52:115–9, 1999.
212. Baron JA. Beneficial effects of
nicotine and cigarette smoking: the real,
the possible and the spurious. Br Med
Bull;52:58–73, 1996.
213. Morens DM, Grandinetti A, Reed D,
White LR, Ross GW. Cigarette smoking
and protection from Parkinson’s disease:
false association or etiologic clue?
Neurology;45:1041–51, 1995.
214. Picciotto MR, Zoli M. Neuroprotection
via nAChrs: the role of nAChrs in
neurodegenerative disorders such as
Alzheimer’s and Parkinson’s disease.
Front Biosci;13:492–504, 2008.
215. Quik M, O’Neill M, Perez XA. Nicotine
neuroprotection
against
nigrostriatal
damage: importance of the animal model.
Trends Pharmacol Sci 2007.
216. O’Neill MJ, Murray TK, Lakics V,
Visanji NP, Duty S. The role of neuronal
nicotinic acetylcholine receptors in acute
and chronic neurodegeneration. Curr Drug
Target CNS Neurol Disord;1:399–411,
2002.
217. Miksys S, Tyndale RF. Nicotine
induces brain CYP enzymes: relevance to
Parkinson’s disease. J Neural Transm
Suppl;177–80, 2006.
218. Quik M, Parameswaran N, McCallum
SE, Bordia T, Bao S, McCormack A, et al.
Chronic oral nicotine treatment protects
against striatal degeneration in MPTPtreated primates. J Neurochem;98:1866–
75, 2006.
219. Grady SR, Salminen O, Laverty
DC,Whiteaker P, McIntosh JM, Collins AC,
et al. The subtypes of nicotinic
acetylcholine receptors on dopaminergic
terminals of mouse striatum. Biochem
Pharmacol;74:1235–46, 2007.
220. Gotti C, Moretti M, Gaimarri A,
Zanardi A, Clementi F, Zoli M.
Heterogeneity and complexity of native
brain
nicotinic
receptors.
Biochem
Pharmacol;74:1102–11, 2007.
221. Quik M, Bordia T, O’Leary K.
Nicotinic receptors as CNS targets for
Parkinson’s
disease.
Biochem
Pharmacol;74:1224–34, 2007.
222. Dani JA, Bertrand D. Nicotinic
acetylcholine receptors and nicotinic
cholinergic mechanisms of the central
nervous system. Annu Rev Pharmacol
Toxicol; 47:699–729, 2007.
223. Albuquerque EX, Pereira EF,
Alkondon M, Rogers SW. Mammalian
nicotinic acetylcholine receptors: from
structure to function. Physiol Rev;89:73–
120, 2009.
224. Millar NS, Gotti C. Diversity of
vertebrate
nicotinic
acetylcholine
receptors. Neuropharmacology; 56:237–
46, 2009.
225. Exley R, Cragg SJ. Presynaptic
nicotinic receptors: a dynamic and diverse
cholinergic filter of striatal dopamine
neurotransmission.
Br
J
Pharmacol;153(Suppl. 1):S283–97, 2008.
226. Quik M, McIntosh JM. Striatal alpha6*
nicotinic acetylcholine receptors: potential
targets for Parkinson’s disease therapy. J
Pharmacol Exp Ther; 316:481–9, 2006.
227. Salminen O, Murphy KL, McIntosh
JM, Drago J, Marks MJ, Collins AC, et al.
Subunit composition and pharmacology of
two classes of striatal presynaptic nicotinic
acetylcholine
receptors
mediating
dopamine
release
in
mice.
Mol
Pharmacol;65:1526–35, 2004.
228. Perry DC, Mao D, Gold AB, McIntosh
JM, Pezzullo JC, Kellar KJ. Chronic
nicotine differentially regulates {alpha}6and
{beta}3-containing
Nicotinic
Cholinergic Receptors in Rat Brain. J
Pharmacol Exp Ther 2007.
229. Perez XA, Bordia T, McIntosh JM,
Grady SR, Quik M. Long-term nicotine
treatment differentially regulates striatal
alpha6alpha4beta2*
and
alpha6(nonalpha4)beta2* nAChr expression and
function. Mol Pharmacol;74: 844–53,
2008.
230. Bordia T, Grady SR, McIntosh JM,
QuikM. Nigrostriatal damage preferentially
decreases
a
subpopulation
of
{alpha}6{beta}2* nAChrs in mouse,
monkey and Parkinson’s disease striatum.
Mol Pharmacol;72:52–61, 2007.
231. Costa G, Abin-Carriquiry JA, Dajas F.
Nicotine prevents striatal dopamine loss
produced by 6-hydroxydopamine lesion in
the substantia nigra. Brain Res;888:336–
42, 2001.
232. Ryan RE, Ross SA, Drago J,
Loiacono
RE.
Dose-related
neuroprotective effects of chronic nicotine
in 6-hydroxydopamine treated rats, and
12
loss of neuroprotection in alpha4 nicotinic
receptor subunit knockout mice. Br J
Pharmacol;132:1650–6, 2001.
233. Picciotto MR, Zoli M. Neuroprotection
via nAChrs: the role of nAChrs in
neurodegenerative disorders such as
Alzheimer’s and Parkinson’s disease.
Front Biosci;13:492–504, 2008.
234. Dajas-Bailador F, Wonnacott S.
Nicotinic acetylcholine receptors and the
regulation of neuronal signalling. Trends
Pharmacol Sci;25:317–24, 2004.
235. Gahring LC, Rogers SW. Neuronal
nicotinic acetylcholine receptor expression
and function on nonneuronal cells. Aaps
J;7:E885–94, 2005.
236.
Tracey KJ.
Physiology and
immunology of the cholinergic antiinflammatory
pathway.
J
Clin
Invest;117:289–96, 2007.
237. Belluardo N, Blum M, Mudo G,
Andbjer B, Fuxe K. Acute intermittent
nicotine treatment produces regional
increases of basic fibroblast growth factor
messenger RNA and protein in the tel- and
diencephalon
of
the
rat.
Neuroscience;83:723–40, 1998.
238. Belluardo N, Mud G, Blum M, Cheng
Q, Caniglia G, Dell’Albani P, et al. The
nicotinic acetylcholine receptor agonist
(+/_)-epibatidine increases FGF-2 mRNA
and protein levels in the rat brain. Brain
Res Mol Brain Res;74:98–110, 1999.
239. Massey KA, Zago WM, Berg DK.
BDNF up-regulates alpha7 nicotinic
acetylcholine
receptor
levels
on
subpopulations
of
hippocampal
interneurons. Mol Cell Neurosci; 33:381–8.
2006.
240. Zhou X, Nai Q, Chen M, Dittus JD,
Howard MJ, Margiotta JF. Brain-derived
neurotrophic factor and trkB signaling in
parasympathetic neurons: relevance to
regulating
alpha7-containing
nicotinic
receptors and synaptic function. J
Neurosci; 24:4340–50, 2004.
241. Shih JC, Chen K, Ridd MJ.
Monoamine oxidase: from genes to
behavior. Annu Rev Neurosci; 22:197–
217, 1999.
242. Kurth JH, Kurth MC, Poduslo SE,
Schwankhaus JD. Association of a
monoamine oxidase B allele with
Parkinson’s disease. Ann Neurol; 33:368–
72, 1993.
243. Costa P, Checkoway H, Levy D,
Smith-Weller T, Franklin GM, Swanson
PD, Costa LG. Association of a
polymorphism in intron 13 of the
monoamine oxidase B gene with
Parkinson disease. Am J Med Genet;
74:154–6, 1997.
244. Checkoway H, Franklin GM, CostaMallen P, Smith-Weller T, Dilley J,
Swanson PD, Costa LG. A genetic
polymorphism of MAO-B modifies the
association of cigarette smoking and
Parkinson’s disease. Neurology;50:1458–
61, 1998.
245. Mellick GD, McCann SJ, Le Couter
DG. Parkinson’s disease, MAO-B, and
smoking. Neurology;53:658, 1999.
246. Hernan MA, Checkoway H, O’Brien
R, Costa-Mallen P, De Vivi I, Colditz GA,
Hunter DJ, Kelsey KT, Ascherio A.
Monoamine oxidase B intron 13 and
catechol-O-methyltransferase codon 158
polymorphisms, cigarette smoking, and
the risk of Parkinson’s disease. Neurology;
58:1381–7, 2002.
247. Baldereschi M, Di Carlo A, Rocca
WA, Vanni P, Maggi S, Perissinotto E,
Grigoletto F, Amaducci L, Inzitari D.
Parkinson’s disease and Parkinsonism in
a longitudinal study: two-fold higher
incidence in men. ILSAWorking Group.
Italian Longitudinal Study on Aging.
Neurology;55:1358–63, 2000.
248. Kelada SN, Costa-Mallen P, Costa
LG, Smith-Weller T, Franklin GM,
Swanson PD, Longstreth Jr. WT,
Checkoway H Gender Difference in the
Interaction of Smoking and Monoamine
Oxidase B Intron 13 Genotype in
Parkinson’s Disease NeuroToxicology 23
515–519, 2002.
249. W. Linert , M.H. Bridge, M. Huber ,
K.B. Bjugstad , S. Grossman ,G.W.
Arendash, In vitro and in vivo studies
investigating possible antioxidant actions
of nicotine: relevance to Parkinson's and
Alzheimer’s diseases, Biochimica et
Biophysica Acta 1454 143-152, 1999.
250. Fredholm BB. Adenosine, adenosine
receptors and the actions of caffeine.
Pharmacol Toxicol;76:93–101, 1995.
251. Schwarzschild MA, Chen J, Ascherio
A. Caffeinated clues and the promise of
adenosine A2A antagonists in Parkinson’s
disease. Neurology; 58:1154–60, 2002.
13
252. Ascherio A, Zhang SM, Hernán MA,
et al. Prospective study of caffeine
consumption and risk of Parkinson’s
disease in men and women. Ann
Neurol;50:56–63. 2001.
253. Ross GW, Abbott RD, Petrovich H, et
al. Association of coffee and caffeine
intake with the risk of Parkinson disease.
JAMA;283:2674–9 2000.
254.
Benedetti
MD,
Bower
JH,
Maraganore DM, et al. Smoking, alcohol,
and
coffee
consumption
preceding
Parkinson’s disease: a case-control study.
Neurology 2000;55:1350–8.
255. Ascherio A, Chen H, Schwarzschild
MA, et al. Caffeine, postmenopausal
estrogen, and risk of Parkinson’s disease.
Neurology;60:790–5. 2003.
256. Ascherio, Alberto, Weisskopf, Marc
G., O’Reilly, Eilis J., McCullough, Marjorie
L., Calle, Eugenia E., Rodriguez, Carmen
and Thun, Michael J. Coffee Consumption,
Gender, and Parkinson's Disease Mortality
in the Cancer Prevention Study II Cohort:
The Modifying Effects of Estrogen
American
journal
of
epidemiology,
Volume: 160, Issue: 10, pp: 977,
November 15, 2004.
257. Nakaso K, Ito S, Nakashima K
Caffeine activates the PI3K/Akt pathway
and prevents apoptotic cell death in a
Parkinson’s disease model of SH-SY5Y
cells Neuroscience Letters 432, 2008.
258. Mayeux R, Denaro J, Hemenegildo
N, Marder K, Tang M-X, Cote LJ, Stern Y
A population-based investigation of
Parkinson’s disease with and without
dementia. Relationship to age and gender.
Arch Neurol 1992; 49: 492-7
259. Wright CE, Sisson TL, Ichhpurani AK,
Peters GR, Steady-state pharmacokinetic
properties of pramipexole in healthy
volunteers J Clin Pharmacol; 37: 520-5,
1997.
260. Kraus PH, Klotz P, Przuntek H Sex
differences for dopaminergic therapy in
Parkinson’s
disease
[abstract]
Parkinsonism Related Dis 1999; 5; S77-88
261. Marder, K, Tang M-X, Alfaro B, Mejia
H, Cote L, Jacobs D, Stern Y, Sano M,
Mayeux R Postmenopausal estrogen use
and Parkinson’s disease with and without
dementia Neurology;50:1141-3, 1998.
262. Blanchet PJ, Fang J, Hyland K,
Arnold LA, Mouradien MM, Chase TN.
Short term effects of high-dose 17βestradiol in postmenopausal PD patients
Neurology; 53:91-5, 1999.
263. Razandi M, Pedram, A, Greene Gl,
Levin ER, Cell membrane and uclear
estrogen receptors (ERs) originate from a
single transcript: studies of ERα and ERβ
expressed in Chinese hamster ovary cells
Mol endocrinol; 13:307-19, 1999.
264. Carson- Jurica MA, Schrader WT,
O’malley BW Steroid receptor family:
structure and functions Endocr Rev;
11:201-20, 1990.
265. McEwen BS The molecular and
neuroanatomical basis for estrogen effects
in the central nervous system J Clin
Endocrinol Metab; 84: 1790-7, 1999.
266. Gundlah C, Kohama SG, Mirkes SJ,
Garyfallou VT, Urbansky HF, Bethea CL
Distribution of estrogen receptor beta
mRNA in hypothalamus, midbrain and
temporal lobe of spayed macaque:
continued expression with hormone
replacement Brain Res Mol Brain Res; 76:
191-204, 2000.
267. Sawada H, Ibi M, Kihara T, Urushitani
M, Honda K, Nakanishi M, Akaike A,
Shimohama
S
Mechanisms
of
antiapoptotic effects of estrogens in nigral
dopaminergic neurons FASEB J; 14:
1201-14, 2000.
268. Pappas TC, Gametchu B, Watson CS
Membrane estrogen receptors identified
by multiple antibody labelling and
impeded-ligand binding FASEB J; 9:40410, 1995.
269. Beyer C, Raab H Nongenomic effects
of estrogen: embryonic mouse midbrain
neurones respond with a rapid release of
calcium from intracellular stores Eur J
Neurosci;10:255-62, 1998.
270. Dluzen D. Estrogen decreases
corpus striatal neurotoxicity in response to
6-hydroxydopamine Brain Res;767:340-4,
1997.
157. Disshon KA, Dluzen DE Estrogen as
a neuromodulator of MPTP- induced
neurotoxicity:
effects
upon
striatal
dopamine release Brain Res;9-16, 1997.
271. Dluzen DE, McDermott JL, Liu B
Estrogen as a neuroprotectant against
MPTP-induced neurotoxicity in C57/B1
mice Neurotoxicol Teratol;18:603-6, 1996.
272. Dluzen DE, McDermott JL, Liu B
Estrogen
alters
MPTP-induced
14
neurotoxicity in female mice: effects on
striatal dopamine concentrations and
release J neurochem;66:658-66, 1996.
273. Leranth C, Roth RH, Elswoth JD,
Naftolin Fm Norvath TL, Redmond Jr. DE
Estrogen is essential for maintaining
nigrostriatal dopamine neurons in primates
: implications for Parkinson’s disease and
memory J Neurosci;20:8604-9, 2000.
274. Kang UJ Potential of gene therapy for
Parkinson’s
disease:
neurobiological
issues and new developments in gene
transfer methodologies Mov Disord;13:5972, 1998.
275. Lapchak PA, Gash DM, Jiao S, Miller
PJ, Hilt D Glial cell line- derived
neurotrophic factor: a novel therapeutic
approach to treat motor dysfunction in
Parkinson’s disease. Exp Neurol;144:2934, 1997.
276.
Lapchak
PA
A
preclinical
development
strategy
designed
to
optimize the use of glial cell-line derived
neurotrophic factor in the treatment of
Parkinson’s disease Mov Disord;13:49-54,
1998.
15
Appendix 1 (Eeden et al. [46])
Incidence/prevalence in Developed Countries (USA)
The United States of America consists of many different race/ ethnicity groups from
‘black’ to ‘whites’ and Asian to Hispanics and is also a well-developed country. It is of
this interest to compare data of incidence rates with that of other developing
countries like the Netherlands. In contrast with the study in the Netherlands of
Leentjens et al. (2003), in the USA study of Van Den Eeden et al. (2003) [46] the
authors made a distinction in PD incidence rates between different ethnicities and
race within the USA.
I.III.I Incidence/ prevalence USA
Before the authors could analyse the incidence rates, the cases of PD had to be
defined. The cases were defined as members of KPNCP and were diagnosed with
idiopathic PD between January 1, 1994, and December 31, 1995. All cases had to
meet modified Core Assessment Program for Intracerebral Transplantation
(CAPIT)/Hughes diagnostic criteria at the time of diagnosis and within the study
period, according to the following symptoms: 1) the presence of at least two of the
following signs: resting tremor, cogwheel rigidity, bradykinesia, and postural reflex
impairment, at least one of which must be either resting tremor or bradykinesia; 2) no
suggestion of a cause for another Parkinsonian syndrome such as drugs, trauma,
brain tumor, or treatment within the last 12 months with dopamine-blocking or
dopamine-depleting agents; and 3) no atypical features such as prominent
oculomotor palsy, cerebellar signs, vocal cord paresis, severe orthostatic
hypotension, pyramidal signs, amyotrophy, or limb apraxia. The base population for
this study was the membership of the Kaiser Permanente Medical Care Program
(KPMCP), northern California, a large group practice model prepaid health
maintenance organization. The authors found the KPMCP data very representative
for the general population in gender and race/ethnicity and, because 25-30 percent of
the population in these geographical area belonged to the health plan. Besides,
according to the Internal survey data the KPMCP membership reflects a broad
household income range and is representative for the geographic area except for
having a slightly higher education and income level. After defining cases and
establishing the study population, the data was collected. Race/ethnicity was
categorized as non-Hispanic White, Black, Hispanic, Asian/Pacific Islander, and
other. The latter category included Native Americans (n = 3) and unknown (n = 1).
When all data was collected the authors statistical analysis was been used. Crude
and adjusted annual rates were calculated per 100,000 person-years. Age- and/or
gender-adjusted rates and 95 percent confidence intervals were calculated using
2
direct standardization with the age and/or gender distribution of the 1990 US
population as the reference population. The results of this study show 588 cases of
incident Parkinson disease that met modified Core Asessment Program for
Intracerebral Transplantation. The distribution by age, gender, and race/ethnicity for
cases and the population at risk is presented in table II. The mean age at diagnosis
was 70.5 (range, 38–91) years for men and 70.5 (range, 31–93) years for women.
Non-Hispanic Whites were significantly older at diagnosis than either Hispanics or
Asian/Pacific Islanders, and they were slightly but not significantly older than Blacks.
The estimated crude incidence rate was 12.3 per 100,000, for persons over the age
of 50 the incidence was 44.0 per 100,000. The age- and gender- adjusted incidence
rate was 13,4 per 100,000 with a 95 percent CI of 11.4, 15.5. When looking at man
and women, the incidence rate for men was 19.0 per 100.000 and for women it was
9.9 per 100,000. In table III the incidence by age for men and women is shown. The
incidence rates for both men and women rose rapidly after the age of 60 years. The
overall incidence increases with age, going from 0.50 per 100,000 in the 30- to 39year category to 119.01 per 100,000 in the oldest age category. This same pattern
was observed among men and women, except for a slight drop in the incidence rate
for the 80- to 89-year age category among women. The age- and gender-adjusted
incidence rates were highest among Hispanics, followed by non-Hispanic Whites,
Asians, and Blacks. The comparisons of age- and gender-adjusted incidence rates
between individual groups were none of all statistically significant. In all groups other
than Asians, the incidence of PD among men was approximately twofold higher than
the incidence among women. Among Asians, however, PD incidence was slightly
lower among men than women. It seems that in this study the overall incidence rate
is lower than in the Leentjens et al. (2003) study but show a similar age/ Parkinson
trend. And as in the study of Leentjens et al.(2003) also the results of this study show
a similar trend of PD ratio amongst men and women, with man being more
susceptible to PD than women. Although there were differences between
ethnicity/race and PD in the van den Eeden et al. (2002) study, it is not justifiable to
take the conclusion that one race is more susceptible for PD than other races or to
take any other conclusions about these results. This is due to the relatively low
number of cases amongst the non-white study population. Besides, the comparisons
of age- and gender-adjusted incidence rates between individual groups were none of
all statistically significant. Before we can say something about differences in PD
incidence rates in different ethnicity/ race groups, more studies need to be done on
this topic. Besides, we also have to look at the PD incidence rates amongst people in
non- developing countries.
Table II: Parkinson’s disease cases and
population by gender, age, race/ethnicity, and
year, Kaiser Permanente, 1994-1995 [46]
3
Table III: Annual incidence rate* of Parkinson’s disease by gender and age, all ethnic
groups combined Kaiser Permanente, 1994- 1995 [46]
4